Full Length Research Paper

ABSTRACT
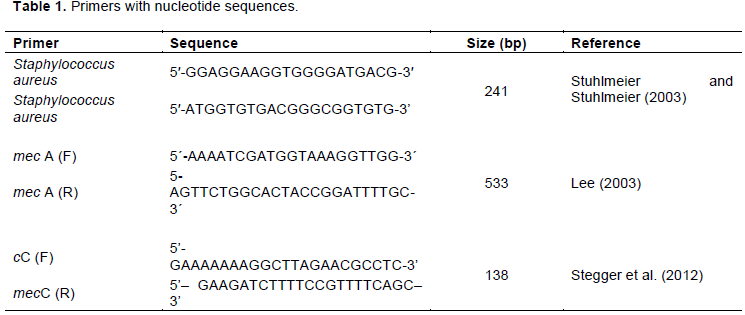
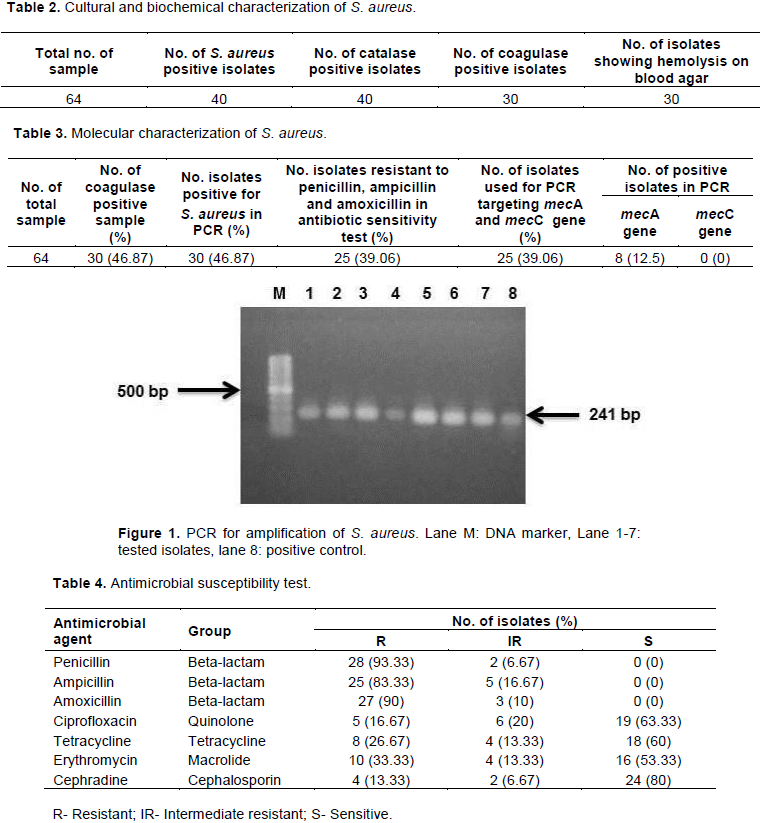
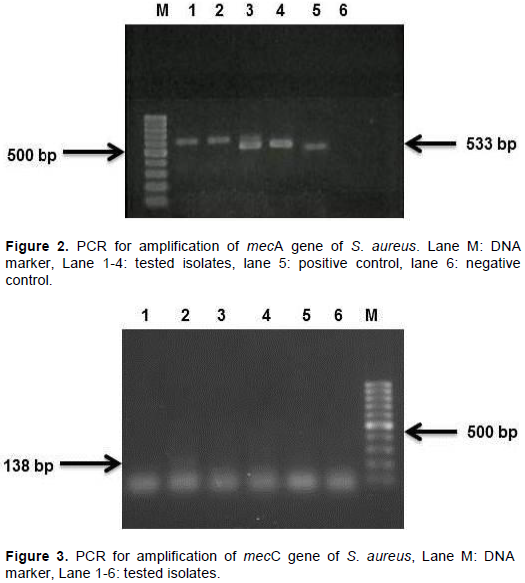
Staphylococcus aureus is an opportunistic pathogen causing dental infection and systemic infections in human body. This organism decreases susceptibility to several types of antibiotics every day and becomes more resistant which is a growing sense of concern in this era. Considering this fact, the study was attempted to characterize the S. aureus from human dental infection and to determine the antibiogram profile of isolates. Sixty four (64) samples were collected from the patients with dental infection who visited different dental clinics and hospitals in Mymensingh, Bangladesh for treatment. Isolation and identification of S. aureus were conducted by using cultural, morphological, and biochemical characteristics. Polymerase chain reaction was performed for final confirmation of S. aureus followed by detection of methicillin resistant S. aureus (MRSA) targeting mecA and mecC genes. Antibiotic susceptibility test of isolated bacteria was tested against seven antibiotics by disk diffusion methods. Forty isolates among 64 samples were found positive for S. aureus based on cultural characteristics. Among them 30 isolates were found positive in coagulase test. Depending on the result of coagulase test, all the 30 isolates were subjected to antibiotic sensitivity test and among them 25 were 100% resistant to penicillin, ampicillin and amoxicillin. All the 25 isolates were subjected to polymerase chain reaction (PCR) to identify methicillin resistant gene mecA and mecC. Eight isolates were positive for mecA gene while no isolates were positive for mecC. The present findings conclude that S. aureus is prevalent in dental infections and contain methicillin resistant genes.
Key words: Dental infection, Staphylococcus aureus, antibiotic resistance, methicillin resistant S. aureus (MRSA).
INTRODUCTION
MATERIALS AND METHODS
RESULTS AND DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
REFERENCES
|
Ayepola OO, Olasupo NA, Egwari LO, Becker K, Schaumburg F (2015). Molecular characterization and antimicrobial susceptibility of Staphylococcus aureus isolates from clinical infection and asymptomatic carriers in Southwest Nigeria. Plos One 10(9):e0137531. |
|
|
Bannerman T, Peacock S (2007). Staphylococcus, Micrococcus, and other catalase positive cocci. In: Murray, P., Baron, E., Jorgensen, J., Landry, M., Pfaller, M. (Eds.), Manual of Clinical Microbiology 9th ed. ASM Press, Washington, DC, pp. 390-411. |
|
|
Bauer A, Kirby W, Sherris JC, Turck M (1966). Antibiotic susceptibility test¬ing by a standardized single disk method. American Journal of Clinical Pathology 45(4):493-496. |
|
|
Cheesbrough M (1985). Medical laboratory manual for tropical coun¬tries. In: Microbiology. 1st edition, English Language Book Society, London, pp 400-480. |
|
|
Clinical and Laboratory Standards Institute (CLSI) (2016). Performance standards for antimicrobial susceptibility testing. 26th edition, CLSI supplement M100s. Clinical and Laboratory Standards Institute, Wayne, Pennsylvania. |
|
|
Dashti AA, Jadaon MM, Abdulsamad AM, Dashti HM (2009). Heat treatment of bacteria: A simple method of DNA extraction for molecular techniques. Kuwait Medical Journal 41(2):117-122. |
|
|
David MZ, Daum RS (2010). Community-associated methicillin-resistant Staphylococcus aureus: epidemiology and clinical consequences of an emerging epidemic. Clinical Microbiology Reviews 23(3):616-687. |
|
|
Faden A (2018). Methicillin-resistant Staphylococcus aureus (MRSA) screening of hospital dental clinic surfaces. Saudi Journal of Biological Sciences. |
|
|
Gibson J, Wray D, Bagg J (2000). Oral staphylococcal mucositis: A new clinical entity in orofacial granulomatosis and Crohn's disease. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 89(2):171-176. |
|
|
Harte JA (2010). Standard and transmission-based precautions: an update for dentistry. The Journal of the American Dental Association 141(5):572-581. |
|
|
Heitzâ€Mayfield LJ, Lang NP (2010). Comparative biology of chronic and aggressive periodontitis vs. periâ€implantitis. Periodontology 53(1):167-181. |
|
|
Karmakar A, Dua P, Ghosh C (2016). Biochemical and molecular analysis of Staphylococcus aureus clinical isolates from hospitalized patients. Canadian Journal of Infectious Diseases and Medical Microbiology 2016:9041636. |
|
|
Khan AH, Shamsuzzaman AKM, Paul SK, Alam MM, Mahmud MC (2007). Antimicrobial susceptibility and coagulase typing of MRSA strains at Mymensingh Medical College. Bangladesh Journal of Medical Microbiology 1(2):56-60. |
|
|
Kim GY, Lee CH (2015). Antimicrobial susceptibility and pathogenic genes of Staphylococcus aureus isolated from the oral cavity of patients with periodontitis. Journal of Periodontal and Implant Science 45(6):223-228. |
|
|
Kim Y (2012). Multiple antimicrobial resistance patterns of Staphylococcus aureus isolated from periodontitis patients in Seoul, Korea. Korean Journal of Oral and Maxillofacial Pathology 36:317-339. |
|
|
Kurita H, Kurashina K, Honda T (2006). Nosocomial transmission of methicillin-resistant Staphylococcus aureus via the surfaces of the dental operatory. British Dental Journal 201(5):297-300. |
|
|
Lee JH (2003). Methicillin (oxacillin)-resistant Staphylococcus aureus strains isolated from major food animals and their potential transmission to humans. Applied and Environmental Microbiology 69(11):6489-6494. |
|
|
Loir LY, Baron F, Gautier M (2003). Staphylococcus aureus and food poisoning. Genetics and Molecular Research Journal 2(1):63-76. |
|
|
McCormack MG, Smith AJ, Akram AN, Jackson M, Robertson D, Edwards G (2015). Staphylococcus aureus and the oral cavity: An overlooked source of carriage and infection? American Journal of Infection Control 43(1):35-37. |
|
|
Mohapatra SB, Pattnaik M, Ray P (2012). Microbial association of dental caries. Asian Journal of Experimental Biological Sciences 3(2):360-367. |
|
|
Moussa IM, Al-Qahtani AA, Gassem MA, Ashgan MH, Ismail DK, Ghazy AI, Shibl AM (2011). Pulsed-field gel electrophoresis (PFGE) as an epidemiological marker for typing of methicillin-resistant Staphylococcus aureus recovered from King Saudi Arabia (KSA). African Journal of Microbiology Research 5(12):1492-1499. |
|
|
Naeem M, Adil M, Naz SM, Abbas SH, Khan I, Khan A, Khan MU (2012). Resistance and sensitivity pattern of Staphylococcus aureus; a study in lady reading hospital peshawar. Journal of Postgraduate Medical Institute 27(1):42-47. |
|
|
Ohara-Nemoto Y, Haraga H, Kimura S, Nemoto TK (2008). Occurrence of staphylococci in the oral cavities of healthy adults and nasal oral trafficking of the bacteria. Journal of Medical Microbiology 57(1):95-99. |
|
|
Passariello C, Puttini M, Iebba V, Pera P, Gigola P (2012). Influence of oral conditions on colonization by highly toxigenic Staphylococcus aureus strains. Oral Diseases 18(4):402-409. |
|
|
Paterson GK, Harrison EM, Holmes MA (2014). The emergence of mecC methicillin-resistant Staphylococcus aureus. Trends in Microbiology 22(1):42-47. |
|
|
Peters PJ, Brooks JT, McAllister SK, Limbago B, Lowery HK, Fosheim G, Guest JL, Gorwitz RJ, Bethea M, Hageman J, Mindley R, McDougal LK, Rimland D (2013). Methicillin-resistant Staphylococcus aureus colonization of the groin and risk for clinical infection among HIV-infected adults. Emerging Infectious Diseases 19(4):623-629. |
|
|
Poeschl PW, Crepaz V, Russmueller G, Seemann R, Hirschl AM, Ewers R (2011). Endodontic pathogens causing deep neck space infections: clinical impact of different sampling techniques and antibiotic susceptibility. Journal of Endodontics 37(9):1201-1205. |
|
|
Rajaduraipandi K, Mani KR, Panneerselvam K, Mani M, Bhaskar M, Manikandan P (2006). Prevalence and antimicrobial susceptibility pattern of methicillin resistant Staphylococcus aureus: A multicentre study. Indian Journal of Medical Microbiology 24(1):34-38. |
|
|
Ray C, Ryan KJ (2003). Sherris medical microbiology: an introduction to infectious diseases. Appleton and Lange Paramount Publishing Business and Professional Group, 237. |
|
|
Renvert S, Lindahl C, Renvert H, Persson GR (2008). Clinical and microbiological analysis of subjects treated with Brånemark or AstraTech implants: a 7â€year followâ€up study. Clinical Oral Implants Research 19(4):342-347. |
|
|
Smith AJ, Robertson D, Tang MK, Jackson MS, MacKenzie D, Bagg J (2003). Staphylococcus aureus in the oral cavity: a three-year retrospective analysis of clinical laboratory data. British Dental Journal 195(12):701-703. |
|
|
Stegger Á, Andersen PS, Kearns A, Pichon B, Holmes MA, Edwards G, Laurent F, Teale C, Skov R, Larsen AR (2012). Rapid detection, differentiation and typing of methicillinâ€resistant Staphylococcus aureus harbouring either mecA or the new mecA homologue mecALGA251. Clinical Microbiology and Infection 18(4):395-400. |
|
|
Stuhlmeier R, Stuhlmeier KM (2003). Fast, simultaneous, and sensitive detection of staphylococci. Journal of Clinical Pathology 56(10):782-785. |
|
|
Vellappally S, Divakar DD, Al Kheraif AA, Ramakrishnaiah R, Alqahtani A, Dalati MHN, Anil S, Khan AA, Varma HPR (2017). Occurrence of vancomycin-resistant Staphylococcus aureus in the oral cavity of patients with dental caries. Acta Microbiologica et Immunologica Hungarica 64(3):343-351. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


