Full Length Research Paper
ABSTRACT
INTRODUCTION
Despite continued efforts to control the epidemic, rates of infection with human immunodeficiency virus(HIV) and acquired immune deficiency syndrome (AIDS) remain high, especially among women and children in low and middle income countries (UNAIDS, 2012). Countries such as India are struggling to control the epidemic, particularly among the most vulnerable groups (NACO, 2013). According to the World Bank (2012), an estimated 2.4 million persons in India are HIV positive. Women comprise thirty-nine percent of those in India living with HIV, with children under the age of fifteen representing another almost four percent (World Bank, 2012). Infection rates are highest in the southern and western parts of the country, particularly among rural populations. The southern states of Andhra Pradesh, Maharashtra, Karnataka, and Tamil Nadu have some of the highest rates in the nation, with actual infection assumed to be substantially higher than what is reported (World Bank, 2012). A generation of women in India is struggling with the physical and mental health implications of being HIV positive. These stressors may be compounded by high rates of exposure to interpersonal violence among women in India (Simister and Mehta, 2010), and often limited social supportfrom family and community members for persons living with HIV (Sivaram et al., 2009).
Rising HIV infection rates among vulnerable populaions in India have been linked, in part, to the status of women and children (Claeson and Alexander, 2008). Traditional family systems and associated sex-role expectations mean that women have limited power or control, often resulting in an inability to protect themselves from infection (World Bank, 2012). Intimate partner violence (IPV), specifically sexual violence, has also been linked to the spread of HIV (Karamagi et al., 2006). Lifetime partner violence, including emotional, physical, and/or sexual abuse is estimated to be nearly forty percent among married women in India (Silverman et al., 2008), with some recent research suggesting that rates of IPV have further increased in recent years (Simister and Mehta, 2010). Another survey of three-hundred ninety-seven rural southern Indian women found that thirty-four percent had been hit and/or forced in other ways to have sex with their husbands (Coast, 2013). Exposure to this type of interpersonal violence has been associated with negative mental health consequences including depression, social isolation, and hopelessness (Silverman et al., 2008).
Research indicates that social support can prevent or mitigate mental health and other consequences of exposure to potentially traumatic stressors, including interpersonal violence and life-threatening health conditions such as HIV and AIDS. For example, in one study of sixty-five men and women living with HIV and AIDS, higher rates of satisfaction with social networks and social support were associated with fewer HIV and AIDS symptoms (Ashton et al., 2005). Results from another study indicate that social support is associated with medication adherence for persons with HIV (Gonzalez et al., 2004). Social support has also been linked to decreased risk of adverse mental health consequences in persons with a history of exposure to stressful life events (Ozbay et al., 2007) The association between social support and health-related outcomes highlights the importance of access to support for those living with HIV (Ashton et al., 2005).It is noteworthy however, that most studies of social support and HIV have been conducted in the U.S. and Western Europe, with limited research having been done in settings such as Southern India.
Some research does exist however, on the social experiences of persons living with HIV in India, suggesting that social support can play a critical role in wellbeing. For example, people living with HIV in Chennaihave been found to have relatively low levels of social support, higher feelings of isolation, and a sense of loss of control compared to those without HIV (Sivaram et al., 2009). It is not uncommon for persons living with HIV to report loss of social support from family and friends, the larger community, and even health workers following disclosure of status. Research indicates that some doctors in Southern India have even refused to see or touch an HIV positive patient and have been known to wear masks, mistakenly assuming that they can contract HIV through airborne transmission (Thomas et al., 2009). This type of social rejection, along with other forms of prejudice and discrimination typically associated with HIV- related stigma, has been linked to increased risk of depression and anxiety among HIV positive persons in India (Nyamathi et al., 2013b).
Being HIV positive has been associated with a varietyof stressors as outlined here. As such, it is not surprising that living with HIV can tax coping abilities, potentially having a significant impact on mental health outcomes (Varni et al., 2012). Research suggests that some HIV positive individuals, perhaps due to fear of being socially ostracized, engage in avoidant coping (e.g. attempting to pass as a member of the uninfected majority, hiding medications, or avoiding healthcare facilities). Such avoidant coping, in conjunction with limited social support, can lead to negative health outcomes, reduced quality of life, and psychological distress (Nyamathiet al., 2013a). Some stigma-reduction interventions have shown promise in reducing avoidant coping among HIV positive women in rural India (Nyamathi et al., 2013a).
In addition to mental health symptoms such as depression, anxiety, and low self-esteem, culturally-specific expressions of distress can be a useful means of understanding the experience of HIV positive women in rural India. Somatic complaints including headaches, back pain, gastric problems, painful urination, visual disturbances, palpitations, high blood pressure, and fainting attacks have been reported among South Asian populations with a history of exposure to potentially traumatic stressors (Kohrt and Hruschka, 2010; Pereira et al., 2007). While it is important to rule out other health problems, such complaints may be indicative of psychological distress. Physical complaints are often viewed as more acceptable to report than overt mental health concerns. Little is known about the mental health consequences of living with the various physical and psychological stressors that can accompany HIV, especially in communities where persons may be socially ostracized because of their status. The primary aimof this exploratory study is to address gaps in the literature, increasing understanding of the experience of HIV positive women in rural Southern India. Specific objectives of this study include obtaining a better understanding of the psychological difficulties such women encounter, including treatment by family and community members, and preferred forms of coping with HIV-associated stressors. All of the women in this study were receiving supportive services through a local organization known for assisting HIV positive women with a history of interpersonal violence exposure. As we conducted open-ended focus groups and examined thematic content, many of the struggles, concerns, and coping strategies of the women became clear. This exploratory qualitative study makes a significant contribution to the literature by emphasizing the voices of typically marginalized HIV positive women in Southern India.
METHODS
Participants
Twenty women receiving services from a local non-governmental organization (NGO) participated in two focus groups over the course of two weeks. The specific service provider was selected based on a prior relationship with members of the research team, and because it is one of the only agencies in the area providing services for women living with HIV.
In an effort to encourage open discussion, demographic data was not collected for focus group participants. This decision was made based on concerns from the research team and NGO staff that collecting demographic data may discourage some women from participating, or may result in unrealistic expectations of some additional benefit from participating. However, demographic data for a random sample of women also utilizing services through this same NGO was collected for a related study (author, in prepara-tion). Although the demographics from this randomly selected group may not reflect the specific composition of the focus groups, this information is reported below as a point of reference.
Demographics for random sample of women engaged with the service provider: average age M = 42.5 years; SD=7.10; range=28-55 years; 85% Hindu, 10% Christian; 100% reported being married, although only 15% were living with their spouse - 25% reported being separated and 60% were widowed; 95% of participants indicated they have children; 75% of women had no more than fifth standard year of education; 75% were employed - although 90% reported having “less” or “much less” money than other members of the community. Rates of exposure to traumatic stressors were high: 80% of women surveyed reported a history of interpersonal violence, primarily in the form of abuse by close family members (e.g., husband, mother-in-law).
Procedure
Women were approached by NGO staff at regular social gatherings held at the center as well as contacted by phone and invited to participate in focus groups. Both means of contact were utilized in order to minimize the potential for recruitment biasassociated with only reaching out to women who utilize social services provided by the NGO. They were told they would be asked to discuss topics related to their HIV status. Participants were offered compensation in the form of bus fare to cover transport to and from the center on the day of the focus group. Snacks, coffee, and tea were also provided. In accordance with local standards consent was verbally discussed with each participant. Ethical concerns were minimized by emphasizing the voluntary nature of the focus group in the consent form, emphasizing an ‘opt-in’ procedure for participation; thus making it easy for women to choose to not participate, and explaining that no identifying demographic data would be collected. Confirmation of consent was obtained by either a signature or thumbprint for those who could not write. Study procedures were approved by a university institutional review board at a US-based university and an equivalent in New Delhi before data collection began.
Focus groups
Two focus groups, comprising nine and eleven members, were con-ducted two weeks apart. At the start of each group, the interpreter reviewed informed consent, emphasized the importance of confidentiality, and requested permission to audio record the session.
Focus groups lasted between 30-60 min. One NGO staff member facilitated the discussion while two to three researchers observed.It is the belief of the research team that the NGO staff facilitator was a trusted familiar face to many of the women, increasing the possibility that women would feel comfortable providing honest responses. Both focus groups were conducted in the local language of Tamil, audio recorded, and later transcribed.
Measures
Open-ended questions were used to guide focus group discussion.
Questions were developed by researchers with the intention of eliciting responses related to distress, social support, and coping. Questions were developed in collaboration with staff and previous volunteers working at the NGO, based on anecdotal reports of common issues brought up by women utilizing the center. Specifically, the following questions were asked (back-translated English version provided): 1) “What type of physical and mental difficulties do women in your situation typically experience?”, 2) “Does your community or family treat you differently because of your health status?”, 3) “In difficult times, what do you do to overcome the situation?”, 4) “What gives your life meaning?”, 5) “How do you keep others close to you?” (maintain social ties), 6) “What advice would you give to other women with the same HIV status?”, 7) “Is there anything else you think is important for us to know about women in your situation?”
Translation
Responses were transcribed from Tamil to English, and then back translated from English into Tamil. The NGO-provided interpreter worked closely with other members of the research team throughout this process in an attempt to maintain equivalence of constructs between Tamil and English.
Qualitative data analysis
Two researchers independently coded the back translated English data from the focus groups in order to derive themes based on grounded theory and the constant comparative method (Glaser, 1965; Lincoln and Guba 1985). This has been recognized as a useful approach to coding qualitative data (Maxwell 1996; Maycut and Morehouse 1994; Powell 1997; Westbrook 1994). Coders first independently generated themes based on frequency of responses, resulting in over forty categories. Next, categories were consolidated based on consensus, collapsing overlapping categories into broader themes. This resulted in between three and five categories for each of the seven questions. For example, in response to the focus group question “What type of physical and mental difficulties do women in your situation typically experience?”The following categories emerged: physicalreactions; psychological reactions; rejection by family members; rejection by community; difficulties with employment.
RESULTS
Common themes emerging from focus groups with detailed examples are provided in Table 1 and elaborated here.
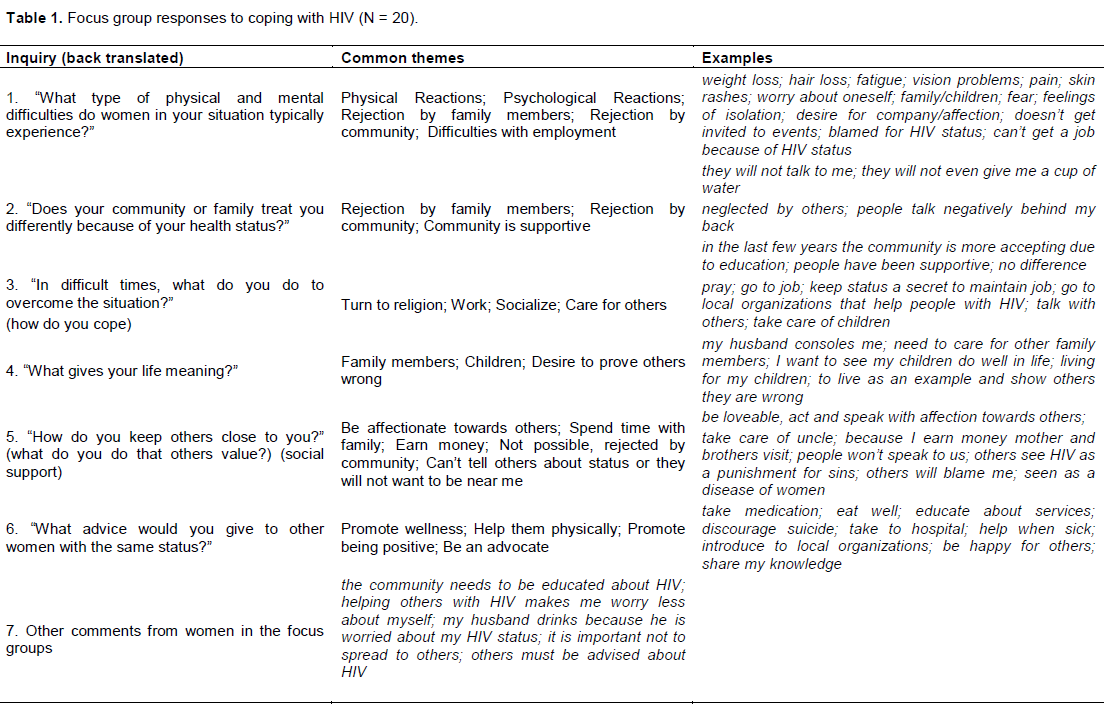
In response to the question “What type of physical and mental difficulties do women in your situation typically experience?” respondents provided descriptions of physical reactions, psychological reactions, examples of rejection by family members and community, and stories about difficulty finding and maintaining employment.
Physical difficulties included: weight loss; hair loss; fatigue; vision problems; pain; and skin rashes. Psychological reactions included: worry about oneself; worry about family/children; fear; feelings of isolation; desire for company/affection: not being invited to community events; being blamed for HIV status; and an inability to get a job because of HIV status.
When asked specifically about how they are treated by family and community members, most women were quick to explain that many people reject them. Examples of rejection included: they will not talk to me; and they will not even give me a cup of water. One women stated that even her own mother will not give her water; another explained that cups used by HIV positive persons are often thrown away. Some women went on to explain, my children aren’t allowed to play with others; (I’m) neglected by others; people talk negatively behind my back; and stated, the community blames women for HIV. Some went on to explain that fear of rejection is why they have not shared their status with others. A few women however, provided examples of community support and explained, in the last few years the community is more accepting due to education.
Given the challenges associated with being HIV positive, we were interested in understanding how the women cope. Specifically we asked, “In difficult times, what do you do to overcome (cope with) the situation?” Common themes included turning to religion – praying often, working to take one’s mind off the situation, socializing with supportive family and community members, participating in HIV positive support groups provided by a local organization, and caring for others, including children and other HIV positive women.
In order to better understand how some women are able to maintain an optimistic outlook despite the challenges associated with being HIV positive, we asked, “What gives your life meaning?” Several women indicated that supportive family members(my husband consoles me) and the desire to ensure their children’s wellbeing (I want to see my children do well in life), give their lives purpose and meaning. Interestingly, some women indicated that a desire to prove others wrong, to show the community that HIV positive persons can make valuable contributions, enables them to get out of bed each day.
Many of the women mentioned the importance of family and community, so we asked a follow up question about how they have been able to find and maintain social support. Some women indicated that they did not have social support because of their HIV positive status (others see HIV as a punishment for sins). Other suggested however, that they had been able to find and maintain social ties by being especially loving/loveable in the eyes of others (act and speak with affection towards others) and providing material support to others (I take care of my uncle; I earn money so my mother and brothers visit).
Finally, we wanted to know what advice these women would give to other HIV positive women. Women spoke at length about the importance of being an advocate for others with HIV, encouraging healthy behaviors such as taking medication and eating well, and the importance of access to material assistance and emotional support. Some mentioned that it is important to learn about what resources exist locally, others stated that HIV positive women should not consider suicide an option. The issue of suicide came up several times, with a few women providing examples of how to take one’s mind off suicide – e.g. I think about my daughter, I live for her.
When provided an opportunity to share additional comments, several women emphasized the importance of HIV positive women such as themselves advocating for others and educating the community about HIV. Other women emphasized that helping others can be therapeutic - helping other with HIV makes me worry less about myself. Some also shared examples about difficulties family members face in coping with a loved one who is HIV positive (my husband drinks because he is worried about my HIV status).
DISCUSSION
This study involved a unique sample of HIV positive women in rural Southern India. Through focus groups, researchers were able to collect data about various challenges and hopes, as women shared experiences of familial rejections, changes in social status, concerns about their children’s future, and a strong desire for social support. Women offered rich examples of what they can and want to do for themselves and others. The results of this exploratory study contribute to our understanding of the psychological difficulties women living with HIV in Southern India encounter, including treatment by family and community members, and preferred forms of coping with HIV-associated stressors.
The results of this study are also consistent with previous research in Southeast Asia, highlighting somatic complaints among those experiencing both acute and chronic stressors (Kohrt and Hruschka, 2010). Many of the women in this study reported weight loss, physical pain, vision problems, and hair loss in response to questions about distress associated with their HIV status. While some of these physical symptoms may be a direct result of their illness, women repeatedly emphasized these complaints when asked about mental health concerns. Another theme that emerged from focus groups was feeling ostracized, specifically, social isolation, and overt rejection by family members and concerns about employment related to their HIV status. Many women reported a change in familial and other social ties following community awareness of their HIV status. Participants indicated that this social rejection has implications for access to healthcare, social support, general wellbeing, and hampers daily functioning. This is consistent with previous research indicating that such forms of social rejection can have negative effects on mental health (Sivaram et al., 2009).
Although women did not speak openly about inter-personal violence in focus groups, research indicates that women who experience physical abuse by their partners are more likely to contract HIV (Dunkle et al., 2004). In fact, there is a growing body of research on the bidirectional nature of domestic violence and HIV in India, with women victims of violence at greater risk for contracting HIV, and HIV positive women more vulnerable to various types of interpersonal abuse (Desai, 2005; Go et al., 2003; Blanchard et al., 2005) This, along with the high rates of interpersonal violence (80%) reported by a random sample of women utilizing the same service provider, suggests that the women in this study are likely coping with multiple stressors, including exposure to interpersonal violence.
Women also expressed substantial worry about the future. Women repeatedly expressed concerns for their children’s wellbeing including worry over what will happen in the event of their death, how to financially support their children considering their deteriorating health and limited income earning potential, and/or the social implications for the children (e.g. social rejection) as a result of their HIV status.Participants reported that focusing on children, religion (e.g. praying), and the potential to prove others wrong (e.g. stabilizing medically, maintaining employment, or being active socially) were things that give their life meaning. Participants also indicated a desire to remain active in their children’s lives and to continue to act as caregivers for their children. Participants identified religion as a comfort in that it provided opportunities for social support through conversations with others about spirituality and spiritual connection through prayer.
Participants emphasized that pursuing education about HIV, engaging in advocacy about HIV, and taking advantage of social support opportunities such as gathering at the local NGO, are important elements of coping with HIV. Many of the women were eager to share this advice with other HIV positive women and expressed a desire to act as role models for others. Several women indicated that community education and raising awareness is critical for addressing stigma surrounding HIV. Several participants explained that there are many reasons to live, highlighting the importance of medication adherence and social support in maintaining physical and mental wellbeing.
Future research
Future research should investigate the themes arising in this exploratory study in a larger sample of HIV positive women in South Asia using mixed methods. Intervention research should also be conducted to determine the potential for HIV stigma reduction strategies to prevent interpersonal violence, increase community acceptance and enhance social support for individuals struggling with the effects of HIV. Specifically, public service announcements emphasizing safe sex practices, means of HIV transmission, dispelling myths, and highlighting the experience of those living with HIV and AIDS should be investigated to determine if these approaches might address some aspects of prevention and treatment. Finally, future research should further examine the inter-section between HIV status and interpersonal violence with an eye towards violence mitigation.
CONCLUSION
This research examined the experience of rural Indian women living with HIV and AIDS. Specifically we considered the psychosocial impact of the epidemic on 20 women engaged with a local service provider. All women expressed some feelings of despair relating to their HIV status, including concerns about the implications of disclosure. Common HIV-related physical and mental health difficulties included feelings of sadness, shame, body aches, and fatigue. Most women provided examples of being socially ostracized by family and other community members: “they will not even give me a drink of water.” However, a few noted that attitudes about HIV positive persons appear to be changing. Popular adaptive coping strategies used to mitigate ongoing stressors included use of religion, engagement with children, accessing social support, and other services through a local NGO. Results suggest service providers should employ strategies designed to enhance effective coping and mitigate distress, especially the distress associated with community rejection.
CONFLICT OF INTERESTS
The author has not declared any conflict of interest.
ACKNOWLEDGEMENTS
Thanks to the C.A.R.E. Center for making this research possible, including M. Stella, and Dr. Buela. We appreciate the CARE Center participants who were warm and welcoming, allowing us to bear witness to their stories. Thanks too for support from the University of Denver, International Disaster Psychology (IDP) program, including Dr. Judith Fox, and former IDP students Tracie Abbott, Andrea Varner, Laura Poole, Alex Weber, Kendall Sauer and Sara Anderson.
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


