Full Length Research Paper
ABSTRACT
Anaesthetic modalities for arteriovenous fistula (AVF) creation include general (GA), local (LA) and regional anaesthesia (RA). Ultrasound guided regional anaesthesia (USRA) proved to have more benefits in AVF creation than the other two. This study conducted at the Douala General Hospital aimed to assess these benefits over GA and RA. A retrospective review was performed on 217 records of patients who underwent an AVF creation between January 2015 and December 2018. The socio-demographic and clinical characteristics of patients were recorded. Analysis of variance, Pearson’s chi-square test and binomial logistic regression were performed and a p value of <0.05 was considered significant. Of the 217 records reviewed, age ranged between 51 and 60 years old, and 71.9% were males. The distribution of AVF according to the anaesthetic type was: 83 (38.2%) for GA, and 68 (31.3%) for USRA. The rate of changeover was significantly associated with the anaesthetic type [GA: null vs. USRA: 8 (11.8%), p < 0.001]. The total anaesthesia administration time and surgical time were significantly associated with the anaesthetic type. The association between the anaesthetic type and the complication was of no statistical importance. This study thus showed that USRA was superior to either GA in AVF creation. The surgical duration mitigated the time required for its performance as compared to GA. It was the most stable in term of cost of anaesthesia and yielded higher rates of functional patency 3 months after the fistulae were created.
Key words: Brachial plexus block, arteriovenous fistula, ultrasound, cost of anaesthesia, patency.
INTRODUCTION
Arteriovenous fistula (AVF) creation is the established ideal vascular access for End Stage Renal Disease (ESRD) patients who undergo haemodialysis (Schmidli et al., 2018). These patients are already weakened by their present comorbidities, therefore the objectives of the anaesthetic modality during an AVF creation are to ensure intraoperative patient comfort, optimize surgical conditions, minimize risk of anaesthetic complications (perioperative cardiac events) and improve postoperative state by avoidance of prolonged sedation and a minimal requirement for strong postoperative analgesia (Rang et al., 2006). Anaesthetic options for AVF creation include general anaesthesia, regional anaesthesia and local anaesthesia. Regional anaesthesia is more cost-effective and there is minor use of anaesthetics (Gonano et al., 2009). Equally, regional anaesthesia targets a limited region of the operated limb with minimal cardiovascular impairment and the presence of an associated sympathetic nerve block both intraoperatively and postoperatively (Shemesh et al., 2017). Intraoperatively, there is a good hemodynamic stability with vasodilation, which facilitates the tracking of vessels by the surgeon (Terkanlioglu et al., 2017). While postoperatively, using regional anaesthesia contributes both to a better management of pain with less consumption of painkillers (Andreae and Andreae, 2012), and the maintenance of an adequate blood flow through the fistula, hence improving maturation by preventing early failure due to thrombosis (Mouquet et al., 1989). Lastly, since 2016 evidence was made that brachial plexus block enhances AVF patency even 3 months after the surgery (Aitken et al., 2016). The introduction of ultrasound guidance has improved peripheral nerve block as compared to electrical nerve stimulation (Ozturk et al., 2016; Abrahams et al., 2009). A study carried out at the Douala General Hospital (DGH) showed that out of 85 vascular accesses created only two-third were functional (done under either general anaesthesia or local anaesthesia) for haemodialysis sessions (Ngatchou et al., 2016). However, in 2017 ultrasound regional anaesthesia came-in at the aforementioned health institution as the main anaesthetic modality for AVF creation. In order to improve the quality of anaesthetic care and outcomes of AVF, we aimed to compare the contribution of ultrasound regional anaesthesia over general anaesthesia in terms of cost of anaesthesia, time analysis, patency periods and complications.
MATERIALS AND METHODS
Retrospective study was conducted at the anaesthesiology and haemodialysis units of Douala General Hospital including all patients above the age of 18, who underwent a primary AVF creation surgery between January 2015 and December 2018. Untraceable patients were excluded who did not show up for haemodialysis sessions at our study site or patients who received local anaesthesia for the AVF creation.
For all the patients, data concerning demographics, pre-existing conditions, preoperative and operative characteristics, American Society of Anaesthesiology (ASA) class, anaesthetic technique, type of AVF and perioperative incidents were collected. Changeovers were defined as the supplementation of another anaesthesia type to the initial anaesthesia, due to a perioperative incident which aggravated the operation.
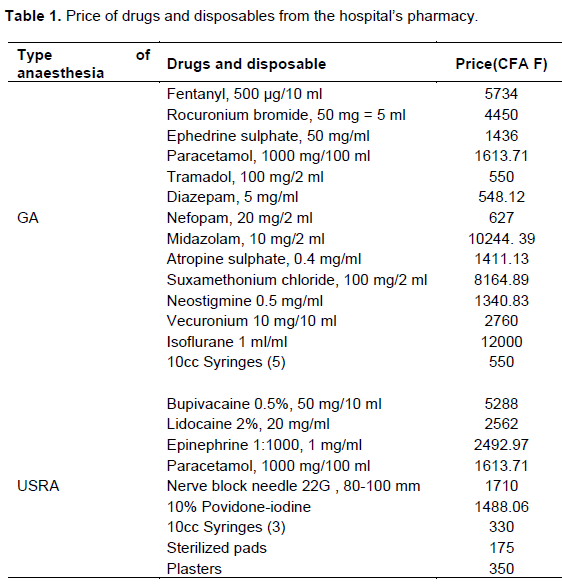
The technical procedures were carried out by a team made up of two vascular surgeons and a general surgeon for the surgery; and three experienced anaesthetists. The cost of anaesthesia was defined as the price of all drugs and disposables used in performing the anaesthesia (personnel and monitor care cost were excluded). A unit price of each item was obtained from the hospital’s pharmacy and expressed in CFA franc (Table 1). In case one type of anaesthesia was required supplemental to another, the cost of additional drugs and disposables were added to the cost of the previous. Total anaesthesia time was defined as the time required to perform the anaesthesia and the duration of surgery as the time recorded in the file to create an AVF. Both were expressed in minutes. The presence of a thrill and murmur, assessed immediately after the operation defined an immediate patency.
All patients were followed up in the immediate postoperative period and after discharge, the perioperative length of stay was recorded. Follow-up was maintained at the haemodialysis unit, firstly to assess the maturity of the fistula and the time at which the haemodialysis cannulation was successful; this was the primary patency. Secondly, to verify the permeability of the AVF three months after their creation. All along the follow-up if a complication occurred, it was recorded. The primary endpoint was the patency at three months. Secondary endpoints were, the primary patency, immediate patency, complications, cost of anaesthesia, duration of surgery, total anaesthesia time. The medical records were accessed and the information therein used to fill our data collection form. Data collection forms were coded and processed using the software EPI-INFO version 7.2.2.16. Continuous variables were presented as means and standard deviations while qualitative variables were presented as frequencies and percentages. All data points were stratified among each anaesthesia type. Bivariate analysis was performed using 2 tests; the one-way analysis of variance (ANOVA), and the Pearson’s chi-square test to display the significant differences between the types of anaesthesia. The significance level was set at 0.05. Approval from Institutional Ethics Committee for Research on Human Health of the University of Douala and the DGH was obtained prior to initiation of the study, and the patient consent requirement was waived due to the retrospective nature of the data.
RESULTS
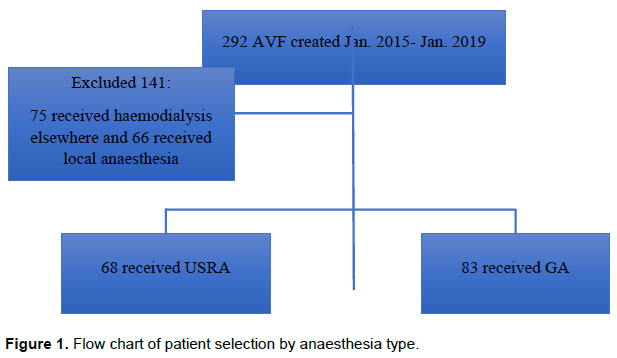
Over the study period, 292 AVF were created, 141 were excluded (75 received haemodialysis elsewhere and 66 were performed under local anaesthesia) and the final sample of 151 remained. Of these, 68 (45.0%) received ultrasound regional anaesthesia and 83 (55.0%) received general anaesthesia (Figure 1).
Demographic and clinical characteristics
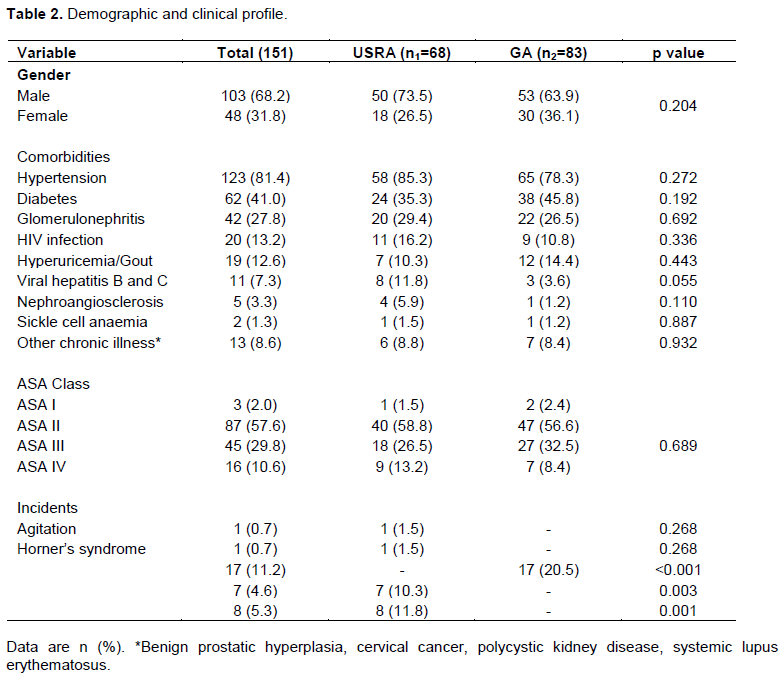
A sex ratio of 2.1 was observed (male predominance of 68.2%); the mean age was 51.1± 12.6 ranging from 18 to 87 years and 56.3% of the sample was aged between 41-60 years. Comorbidities such as hypertension, diabetes and glomerulonephritis were prevalent at 81.4, 41.0 and27.8% respectively. ASA score II held the highest proportion of patients (57.6%) and 81.5% of the AVF created were radiocephalic (Table 2). Both the resurgence of pain and hypotension were significantly associated with the USRA and GA respectively (10.3%; p = 0.003 and 20.5%; p <0.001, respectively). Agitation and resurgence of pain were the only perioperative complications in the USRA group which triggered changeovers.
Outcomes
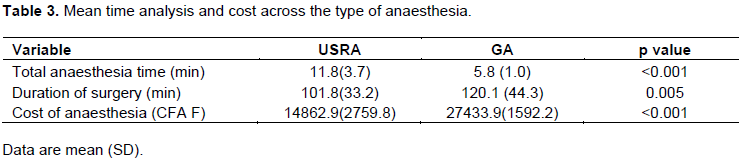
The mean time taken to administer anaesthesia was significantly longer in the USRA group as compared to the GA group (11.8 ± 3.7 vs 5.8 ± 1.0 min for USRA and GA respectively; p <0.001) (Table 3). Nevertheless we found a significant difference in the mean duration of surgery and the type of anaesthesia, where USRA group displayed less time to create an AVF (101.8±33.2 min, for USRA vs 120.1±44.3 min, for GA; p =0.005). Patients who received USRA spent significantly less money to purchase both drugs and disposables than those who had received GA (14862.9 ± 2759.8 vs27433.9 ± 1592.2; p <0.001).
Significant association between the type of anaesthesia and the proportion of patients who had a primary patency six weeks after the operation was found (83.8% for USRA and 63.9% for GA; p = 0.006) (Table 4). The patency three months after the surgery was significantly associated with the type of anaesthesia (USRA 82.3% vs GA 55.4%; p < 0.004). Regarding the complications encountered, only thrombosis was significantly associated with the anaesthesia type (Table 4). Significantly fewer patients in the USRA group suffered from thrombosis than in the GA group.

DISCUSSION
Our study was meant to demonstrate the achievements of the implementation of ultrasound regional anaesthesia as the main anaesthetic modality for arteriovenous fistula creation by assessing its cost-effectiveness, patency at three months, and the complications encountered.
Anesthesia time
Significantly, more time was required to perform an effective ultrasound guided block than the GA procedure. Two studies corroborate our results: regional anaesthesia (47.0 ± 2.2 min) vs. general anaesthesia (32.0 ±37 min) (Siracuse et al., 2014). Equally, Gonano et al. (2009) had similar results where the “interscalene block (ISB) time” added to the “sensory onset time of ISB” was 19.0 ± 10.0 against 13.0± 5.0 min for general anaesthesia group. In practice the performance of a block might always take a longer procedural time. Various factors influence these parameters as the anaesthesiologist experience, where there might be faster recognition and visualisation of neural structure but the difficulty still resides in the administration of the local anaesthetic around the plexus (Picard and Meek, 2010; Vazin et al., 2016).
Surgical time
Regarding the duration of surgery, the USRA group displayed significantly less time for the AVF creation than the general (101.8 ± 33.2 min vs 120.1 ± 44.3 min; p=0.005). Regional blocks with ultrasound guidance have a beneficial sympathetic blockade causing venous dilation at the operative site, and blood vessels tend to be more traceable by the surgeon, who might take less time to perform the fistula (Shemesh et al., 2017). Siracuse et al. (2014) study was the only study to express complete different results from our, where regional anaesthesia was associated significantly with higher surgical time (125.0 min ± 3.3; p<0001) than general anaesthesia (115.0 ±1.4). Also the brachial plexus blocks were performed in the operating room and not in a dedicated block section as in our study, hence the duration of surgery comprised both the time allocated to perform the block and the surgical time itself. The block might have increased the operative time.
Anesthesia cost
The mean total cost per anaesthesia type was significantly lower in the USRA than in the GA group (14862.9±2759.8 CFA F vs27433.9±1592.2 CFA F; p<0.001). With the lingering effect of the sensory block induced by brachial plexus block, it would be possible to reduce the consumption of analgesics and thus of total costs. The cost estimated for USRA is similar to that found in a study conducted in our environment comparing two adjuvants used for ultrasound regional anaesthesia for the upper limb (Metogo et al., 2018). It is all the more affordable as the minimum wage in Cameroon is 36270CFA francs (Ministry of Labor and Social Security, Cameroon, 2014). In addition, this technique of anaesthesia decreases the time of surgery according to our data, therefore could consequently decrease the quantity of drugs used for the anaesthesia.
Patency periods
Although the association between ultrasound regional anaesthesia and immediate patency did not reach statistical significance (p=0.212), records of patients in the ultrasound regional anaesthesia group (97.1%) had the highest rate of immediate patency as compared to the general anaesthesia group(91.6%). Sahin et al. (2011) had a 100% immediate patency in the brachial plexus block against 90% in the control group, but this was statistically irrelevant. Elsharawy and Al-Metwalli (2010) found similar result, where AVFs created both under regional and general anaesthesia were not significantly associated with the success rates (86.0% vs. 89.0%; p=0.80). Regional anaesthesia improves the success of vascular access procedure by producing significant vasodilation enhancing fistula blood flow (Malinzak and Gan, 2009). The functional patency of arteriovenous fistulae was significantly associated with the type of anaesthesia where ultrasound regional anaesthesia displayed the greatest proportion against either general. Similar to Aitken et al. (2016) in the present study, USRA displayed the better functional patency. Indeed, this team was the first to demonstrate the superiority of brachial plexus block over local anaesthesia when assessing the primary patency three months after the operation (84.0% vs.62.0%, OR 3.3, 95% CI 1.4-7.6; p=0.005). Brachial plexus block enhances arterial inflow (Sahin et al., 2011; Shemesh et al., 2006) and increases venous compliance (Schmidli et al., 2018), which both promote blood flow immediately after AVF creation.
Complications
No significant association was found between the anaesthetic type and the complications. However, thrombosis was the most prevalent complication occurring in our population. Three studies was discovered which displayed similar results where no significant association was found between the type of anaesthesia and the complications, but were different in terms of proportion. Aitken et al. (2016) instead revealed that vascular induced ischaemia was the most frequent complication. Meena et al. (2015) recorded the occurrence of four cases of thrombosis in the local anaesthesia group as compared to axillary brachial plexus block where none was encountered. However, this result was of no statistical importance. Sahin et al. (2011) found that thrombosis was instead the second most frequent complications seen in the control group against the infraclavicular block group (2.0 vs. 1.0 p=0.36), after surgical infection. However, these results did not reach statistical significance. In the above studies, preoperative vein mapping and Doppler Ultrasound assessment were performed to measure arterial diameters, identify venous lesions, all of which cancel the risk of thrombosis (Schmidli et al., 2018)
CONCLUSION
Our findings suggest that there is a great difference between ultrasound regional anaesthesia and general anaesthesia. The time performance for ultrasound regional anaesthesia was significantly greater than that in general anaesthesia, but significantly less time was required to create an AVF.
USRA was also superior regarding the cost of anaesthesia and the patency of AVF at three months. In our context where financial resources and access to care are not easy, USRA represent a significant option. This is a major step considering the fact that the lifespans of AVF are highly reduced in our country because of access-related complications.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abrahams MS, Aziz MF, Fu RF, Horn J (2009). Ultrasound guidance compared with electrical neurostimulation for peripheral nerve block?: a systematic review and meta-analysis of randomized controlled trials. British Journal of Anaesthetics 102(3):408-417. |
|
|
Aitken E, Jackson A, Kearns R, Steven M, Kinsella J, Clancy M (2016). Effect of regional versus local anaesthesia on outcome after arteriovenous fistula creation: a randomised controlled trial. The Lancet 388(10049):1067-1074. |
|
|
Andreae MH, Andreae DA (2012). Local anaesthetics and regional anaesthesia prevents chronic pain after surgery (Review). Cochrane Database of Systematic Reviews 17(10):CD007105. |
|
|
Elsharawy MA, Al-Metwalli R (2010). Does regional anesthesia influence early outcome of upper arm arteriovenous fistula? Saudi Journal of Kidney Disease and Transplant 21(6):1048-1052. |
|
|
Gonano C, Kettner SC, Ernstbrunner M, Schebesta K, Chiari A, Marhofer P (2009). Comparison of economical aspects of interscalene brachial plexus blockade and general anaesthesia for arthroscopic shoulder surgery. British Journal of Anaesthetics 103(3):428-433. |
|
|
Malinzak EB, Gan TJ (2009). Regional anesthesia for vascular access surgery. Anesthesia and Analgesia 109(3):976-980. |
|
|
Meena S, Arya V, Sen I, Minz M, Prakash M (2015). Ultrasound-guided supraclavicular brachial plexus anaesthesia improves arteriovenous fistula flow characteristics in end-stage renal disease patients. Southern African Journal of Anaesthesia and Analgesia 21(5):131-134. |
|
|
Mbengono JM, Ngondo FK, Ntock FN, Minkande JZ (2018). Dexaméthasone versus Clonidine utilisés comme adjuvant en ALR pour chirurgie du membre supérieur. Revue de Médecine et de Pharmacie 8(2):801-812. |
|
|
Mouquet C, Bitker MO, Bailliart O, Rottembourg J, Clergue F, Montejo L (1989). Anesthesia for creation of a Forearm Fistula in Patients with Endstage Renal Failure. Anesthesiology 70(6):909-914. |
|
|
Ngatchou W, Evina AN, Halle MP, Massom A, Ekane S, Basile E (2016). Outcome of permanent vascular access for haemodialysis in patients with end-stage renal disease in Cameroon?: results from the pilot experience of the Douala general hospital. Acta Chirurgica Belgica 116(1):36-40. |
|
|
Ozturk O, Bilge A, Tezcan AH, Yagmurdur H, Ulusoy GR, Gezgin I (2016). Comparison of ultrasound and electrical neurostimulation guidance in axillary brachial plexus block. Anaesth Pain and Intensive Care 20(1):50-53. |
|
|
Picard J, Meek T (2010). Complications of regional anaesthesia. Anaesthesia 65:105-115. |
|
|
Rang ST, West NL, Howard J, Cousins J (2006). Anaesthesia for Chronic Renal Disease and Renal Transplantation. EAU-EBU Update Series 4(6):246-256. |
|
|
Sahin L, Gul R, Mizrak A, Deniz H, Sahin M, Koruk S (2011). Ultrasound-guided infraclavicular brachial plexus block enhances postoperative blood flow in arteriovenous fistulas. Journal of Vascular Surgery 54(3):749-753. |
|
|
Schmidli J, Widmer MK, Basile C, de Donato G, Gallieni M, Gibbons CP (2018). Editor's Choice - Vascular Access: 2018 Clinical Practice Guidelines of the European Society for Vascular Surgery (ESVS). European Journal of Vascular and Endovascular Surgery 55(6):757-818. |
|
|
Shemesh D, Olsha O, Orkin D, Raveh D, Goldin I, Reichenstein Y (2006). Sympathectomy-Like Effects of Brachial Plexus Block in Arteriovenous Access Surgery. Ultrasound in Medicine and Biology 32(6):817-822. |
|
|
Shemesh D, Raikhinstein Y, Goldin I, Olsha O (2017). General, regional or local anesthesia for successful radial cephalic arteriovenous fistula. Journal of Vascular Accessment 18(Suppl 1):S24-28. |
|
|
Siracuse JJ, Gill HL, Parrack I, Huang ZS, Schneider DB, Connolly PH (2014). Variability in anesthetic considerations for arteriovenous fistula creation. Journal of Vascular Accessment 15(5):364-369. |
|
|
Terkanlioglu S, Mogul EB, Signak IS, Turker G, Goren S, Kaya FN (2017). Comparison of local and regional anaesthesia in arteriovenous fistula surgery. Journal of Cardiothoracic and Vascular Anesthesia 31:S38-S39. |
|
|
Vazin M, Jensen K, Kristensen DL, Hjort M, Tanggaard K, Karmakar MK (2016). Low-Volume Brachial Plexus Block Providing Surgical Anesthesia for Distal Arm Surgery Comparing Supraclavicular, Infraclavicular, and Axillary Approach: A Randomized Observer Blind Trial. BioMed Research International 21:1-10. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


