Full Length Research Paper
ABSTRACT
Major socioeconomic disparities persist in the management and outcomes of peripheral artery disease (PAD) globally. Allostatic load, which is described as a measure of physiologic adaptation to socio-environmental stress, has been reported to partially explain higher mortality rates in US Blacks. However, it is not clear if allostatic load is associated with PAD severity. The National Health and Nutrition Examination Survey (NHANES), 2003-2004 data was used to identify individuals with PAD based on the calculated Ankle-Brachial Index (
Key words: Allostatic load, outcomes, peripheral arterial disease, severity, socioeconomic.
INTRODUCTION
Major disparities persist in the management of peripheral artery disease (PAD) around the world. While milder
forms of PAD pose a relatively low risk of limb loss (less than 5% over 5 years), more severe PAD (referred to as critical limb ischemia) poses a particularly high risk for major amputation (as high as 40% within 6 months) (Norgren et al., 2007). In order to prevent amputation, patients with critical limb ischemia require prompt restoration of blood flow to their legs (revascularization). Unfortunately, it is reported that Blacks presenting with PAD are more likely to undergo a major amputation as compared to Whites, sometimes as high as three to four times more likely (Feinglass et al., 2008, 2000; Guadagnoli et al., 1995; Huber et al., 1999). This disparity has persisted for decades. In one study, utilizing a statewide database, Huber et al. (1999) reported that Blacks and Whites in Florida did, in fact, receive treatment for PAD at the same rate as whites. Nonetheless, while Whites were more likely to receive limb-saving revascularization, Blacks were more likely to be treated with an amputation (Huber et al., 1999). While some have suggested that this disparity is largely explained by an increased burden of diabetes mellitus in the Black population (Brothers et al., 1997), it has been shown that this disparity exists and is even more pronounced among patients who do not have diabetes (Guadagnoli et al., 1995). In a study of Medicare beneficiaries, the authors concluded that there is “evidence for both segregation and discrimination: site of care was an important factor in a patient’s likelihood of amputation, yet racial gaps persisted even after accounting for differences in the providers caring for Black and White patients” (Regenbogen et al., 2009). Despite the suggestion that a major cause of this disparity may be because Blacks tend to seek care at low-volume institutions with inadequate vascular surgical capabilities, our group and others have documented that these differences persist among patients seeking care at institutions with significant vascular surgical capability (Hughes et al., 2014; Regenbogen et al., 2009)Furthermore, data indicates that a high-volume practice while offering a decrease in the number of amputations for Whites does not confer the same advantage to Blacks. What rather makes a significant difference in the amputation-revascularization racial disparity is the diversity of the surgeon’s practice (Stapleton et al., 2018). The higher the percentage of Black patients a surgeon sees, the more likely the surgeon is to perform a revascularization procedure rather than an amputation on a Black patient (Stapleton et al., 2018).
In a study utilizing the Area Resource File, Hayanga et al. (2009) to examine the association between access to surgical services and the proportion of minorities living in a particular US county, the authors identified that each percentage point increases in Blacks and/or Hispanics was associated with a significant decrease in surgeons, and surgical volume (Hayanga et al., 2009). Decreased access to health care by Blacks in the United States has long been reported (Nelson, 2002). This is particularly true for cardiovascular disease (Davis et al., 2007). More specifically, it has been well described that even when presenting with similar symptoms, Blacks are significantly less likely to receive cardiovascular interventions (Davis et al., 2007; Kressin et al., 2004). Consistent with the ongoing debate as to whether the amputation-revascularization racial disparity is largely sociologic or biological in etiology, some have postulated that PAD in Blacks may, in fact, be biologically different from, and more severe than, PAD in Whites (Sidawy et al., 1990)and that Black race is a strong and independent risk factor for PAD (Criqui et al., 2005). Indeed, using the Vascular Quality Initiative, a prospectively-maintained regional database, recently has been shown that Black patients present with more advanced vascular disease at the time of their initial major vascular operation (Soden et al., 2018). Presentation with more advanced disease at the time of initial major vascular operation may suggest that vascular disease in Blacks is potentially more complex and, perhaps, more difficult to treat successfully. What is not known is whether this “potentially more severe vascular disease” is a result of sociologic factors such as access to care, or if this is inherently biologic in nature.
Allostasis and allostatic load have been described as concepts proposed to explain the physiologic responses to environmental stressful stimuli (Carlson and Chamberlain, 2005; Logan and Barksdale, 2008). Allostasis is an extension of the concept of homeostasis, and represents successful physiologic adaptation to socio-environmental stress. It is postulated that repeated life stressors lead to a response pattern in which elements of the physiologic system, the immune system, the sympathetic nervous system and the hypothalamic–pituitary–adrenal axis, remain at heightened levels of activation. Thus, a high allostatic load would be proposed to result in this dysregulated physiologic profile. Allostatic load, which is calculated as a cumulative measure of several clinical/biologic factors including blood pressure, waist-hip ratio, glycated hemoglobin, cholesterol, albumin and CRP, has been reported to partially explain higher mortality rates in US Blacks (Duru et al., 2012). Allostatic load in the current study was calculated as previously described by Beckie (2012)using ten biologic indicators. Allostatic load has been associated with clinical outcomes of patients with cardiovascular and mental health diseases. Whether a greater allostatic load is associated with more severe PAD and a greater risk of amputation in Blacks is currently unknown. Therefore, this study was undertaken to evaluate if allostatic load is associated with PAD severity.
METHODOLOGY
Data source and patient selection
The National Health and Nutrition Examination Survey (NHANES) is a nationally representative, stratified, population survey that employs interview data collected in subjects’ homes as well as data from physical examination and blood samples. Beginning in 1999, NHANES uses a complex, multistage, probability sampling design to select study participants representative of the civilian, non-institutionalized US population (NCHS, 2003 - 2004). About 5000 participants are surveyed every year. Ankle-Brachial Indices (ABI’s), the gold standard for diagnosing PAD, were calculated for all subjects participating in NHANES Wave for 2003 to 2004 (last year when ABI’s were recorded).
PAD was diagnosed by calculating the ABI. An average of the two posterior tibial artery doppler occlusion pressures recorded for each participant in NHANES was divided by the higher of the two brachial artery doppler occlusion pressures to determine the ABI for each leg. Subjects with one or both ABI’s ≤0.9 were diagnosed as having PAD. Subjects with an ABI >1.40, suggestive of calcified non-compressible vessels, were excluded. To eliminate atypical etiologies for PAD and given the extremely low prevalence of PAD among young patients, patients younger than 40 years old were excluded from analysis (Conte et al., 2015). Study subjects’ demographic data including age, sex, educational background, Body Mass Index (BMI) and racial/ethnic self-identification were collected. Participants’ comorbidities including a history of smoking, hypertension and diabetes mellitus were also recorded.
Determination of allostatic load
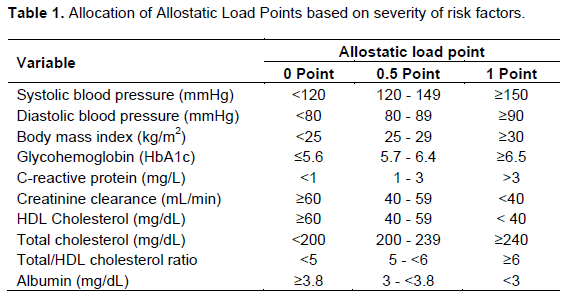
Allostatic load was calculated as previously described by Beckie (2012). Ten biologic indicators that measure cardiopulmonary function, parasympathetic function, cardiometabolic risk, glucose metabolism and inflammation will be examined. Parameters measured included systolic blood pressure, diastolic blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol, total/HDL cholesterol ratio, creatinine clearance, body mass index, glycohemoglobin, albumin and C-reactive protein. These ten biologic indicators which represent cardiometabolic risk, glucose metabolism, cardiopulmonary functioning, parasympathetic functioning, and inflammation have been used in past research using NHANES data (Beckie, 2012). Allostatic load was determined for each participant with each indicator defined as high-, moderate-, or low-risk categories using the following respective designations: systolic blood pressure: ≥150 mmHg, 120 to <150 mmHg, and <120 mmHg; diastolic blood pressure: ≥90 mmHg, 80 to <90 mmHg, and <80 mmHg; body mass index (BMI): ≥30 kg/m3, 25 to <30 kg/m3, and 18 to <25 kg/m3; glycohemoglobin: ≥6.5%, 5.7% to <6.5%, and <5.7%; total cholesterol: ≥240 mg/dL, 200 to <240 mg/dL, and <200 mg/dL; HDL cholesterol: <40 mg/dL, 40 to <60 mg/dL, and ≥60 mg/dL; total/HDL cholesterol ratio: ≥6, 5 to <6, and <5; C-reactive protein: ≥3 mg/L, 1 to <3 mg/L, and <1 mg/L; albumin: <3.0 μg/mL, 3.0 to <3.8 μg/mL, and ≥3.8 μg/mL; and creatinine clearance: <30 mL/min/1.73 m2, 30 to <60 mL/min/1.73 m2, and ≥60 mL/min/1.73 m2. Allostatic load was calculated by assigning one point for the high-risk category, a half point for moderate-risk, and zero points for low-risk. The details of this point allocation are shown in Table 1. Following previous research, a half point was added to the allostatic load score of participants who report taking medication for hypertension, diabetes, and/or cholesterol and who had a low-risk value for blood pressure, glycohemoglobin, or lipids, respectively. The maximum possible allostatic load score was 10 points (Rodriquez et al., 2018).
Outcome measures
The primary outcome measure was the severity of PAD as determined by the ABI (ABI < 0.4 severe PAD; ABI 0.4 – 0.79 moderate; and ABI 0.8 – 0.9 mild PAD). Effects of demographics including race/ethnicity and gender as well as insurance status were also evaluated. Subjects with missing variables pertaining to ABI were excluded from analysis.
Institutional Review Board (IRB)
Given that this study, utilized de-identified patient data, an IRB waiver was granted the following submission of an IRB application.
Statistical analyses
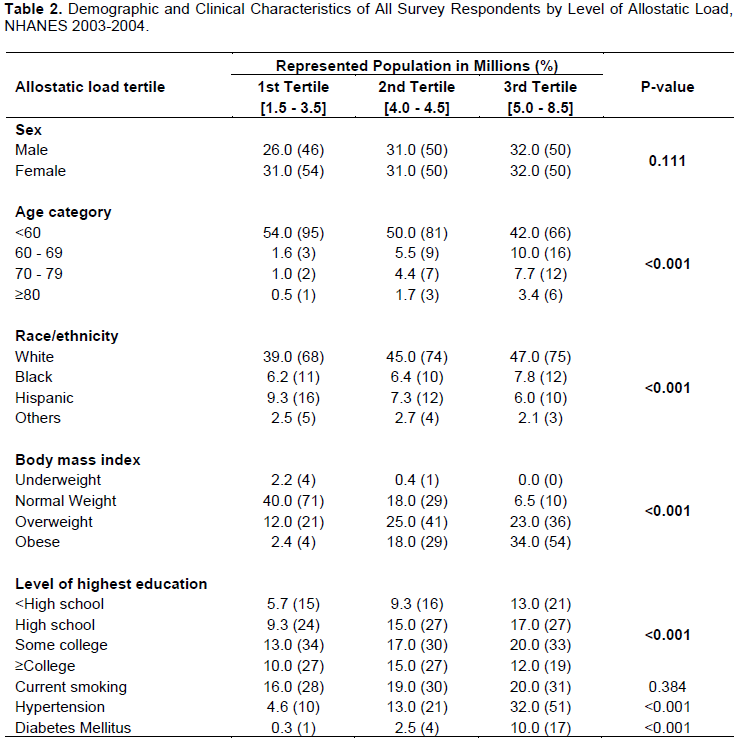
All participants in the survey were divided into three roughly equal parts (tertiles) based on their allostatic loads, because there are no widely accepted thresholds for high or low allostatic loads in the literature. Individuals with relatively low allostatic loads (1.5 - 3.5) were in the first tertile, those with moderate allostatic loads (4.0 - 4.5) were in the second tertile, while those with relatively higher allostatic loads (5.0 - 8.5) were in the third tertile.
Using Pearson Chi-square tests, characteristics of individuals in the different levels of allostatic load were compared. The differences in the distribution of allostatic load between those with PAD and those without PAD were compared using Pearson Chi-square tests. Using similar methodology, differences in the severity of PAD (mild, moderate, or severe) across different tertiles of allostatic load were evaluated. The distribution of PAD severity across levels of each of the 10 stress biomarkers included in the allostatic load score were also evaluated.
Allostatic load was examined as a continuous variable and the association between this variable and ABI (0.1 - 0.9) was evaluated in a correlation plot. ABI was then used as the dependent variable in a multivariable linear regression analysis and factors associated with a 1 decimal point decrease in ABI (increased PAD severity) were examined. To further determine predictors of PAD severity, a multivariable logistic regression model was built and independent associations between individuals having moderate-severe PAD vs. mild PAD were determined. Lastly, to evaluate the independent association between allostatic load and the diagnosis of PAD, patients with PAD were compared to those without PAD in a multivariate logistic regression model.
All analyses were performed using NHANES survey weights in order to provide nationally representative estimates. Analyses were done using STATA Statistical software: 14.2 (College Station, TX: StataCorp LLC) and the level of significance was set at P <0.05.
RESULTS
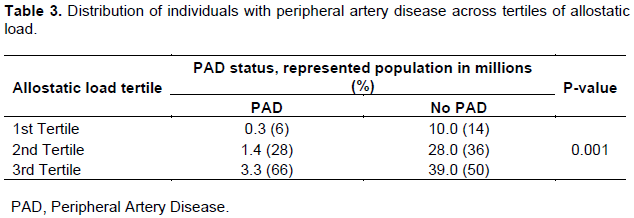
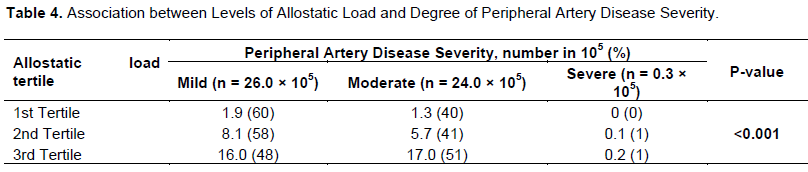
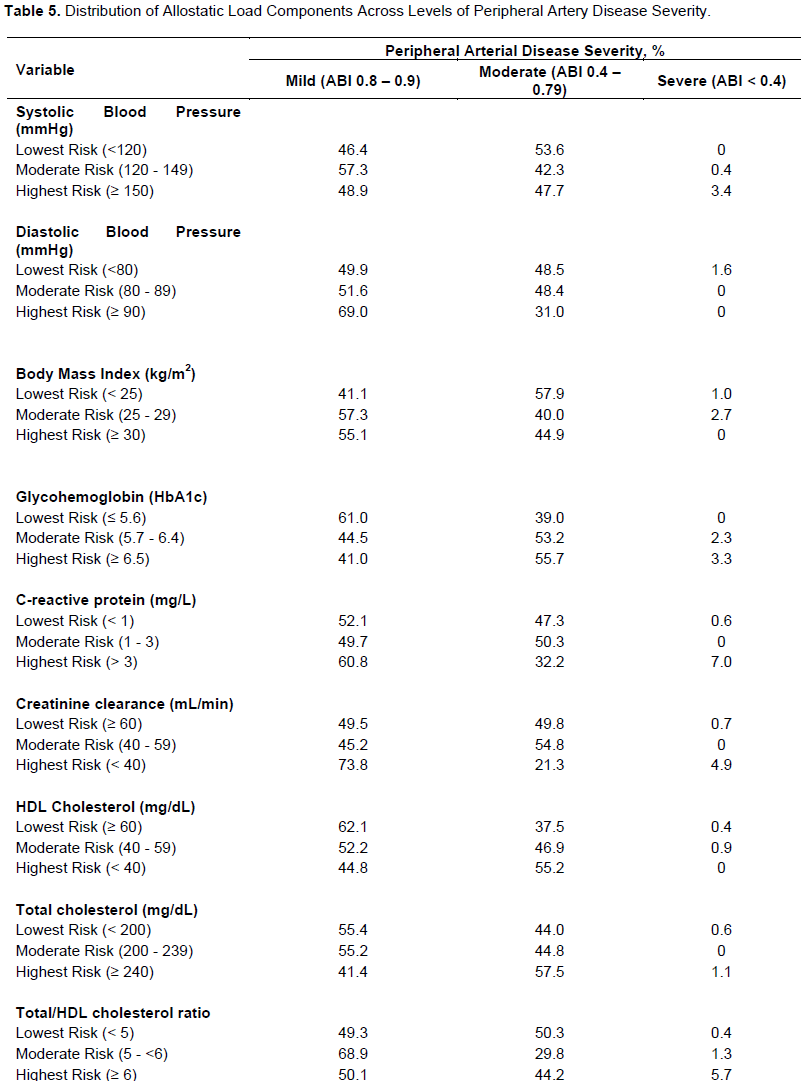
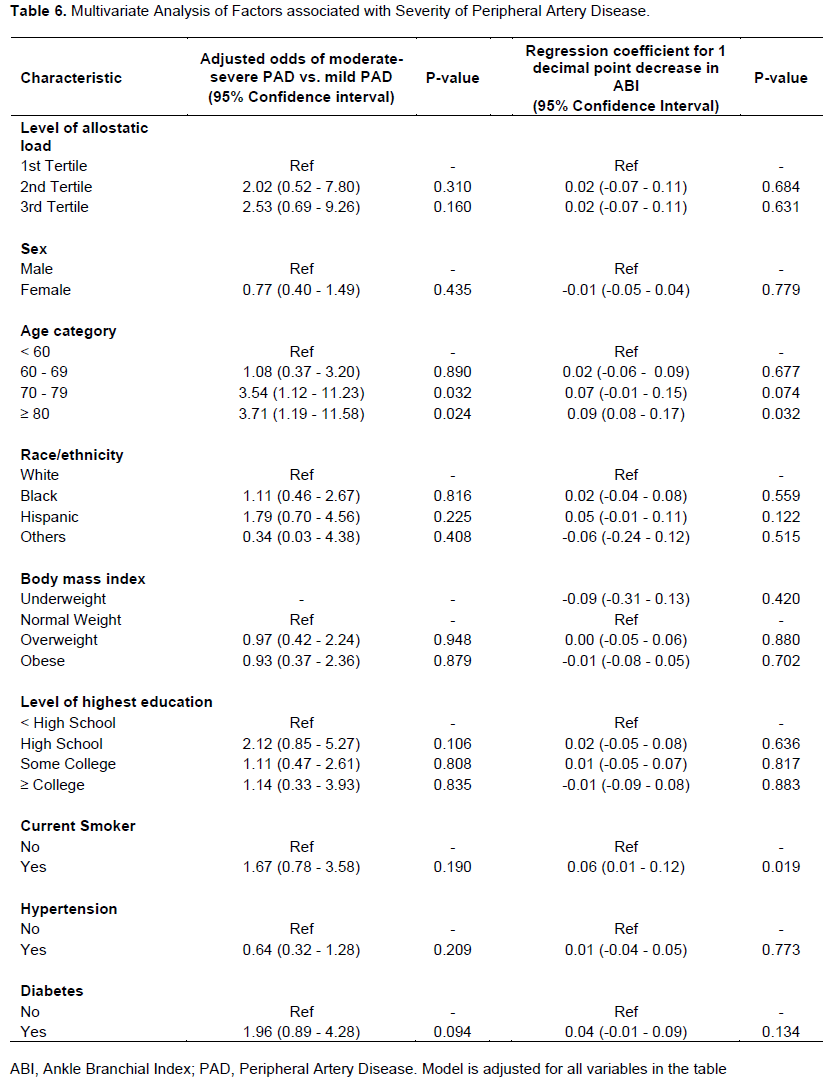
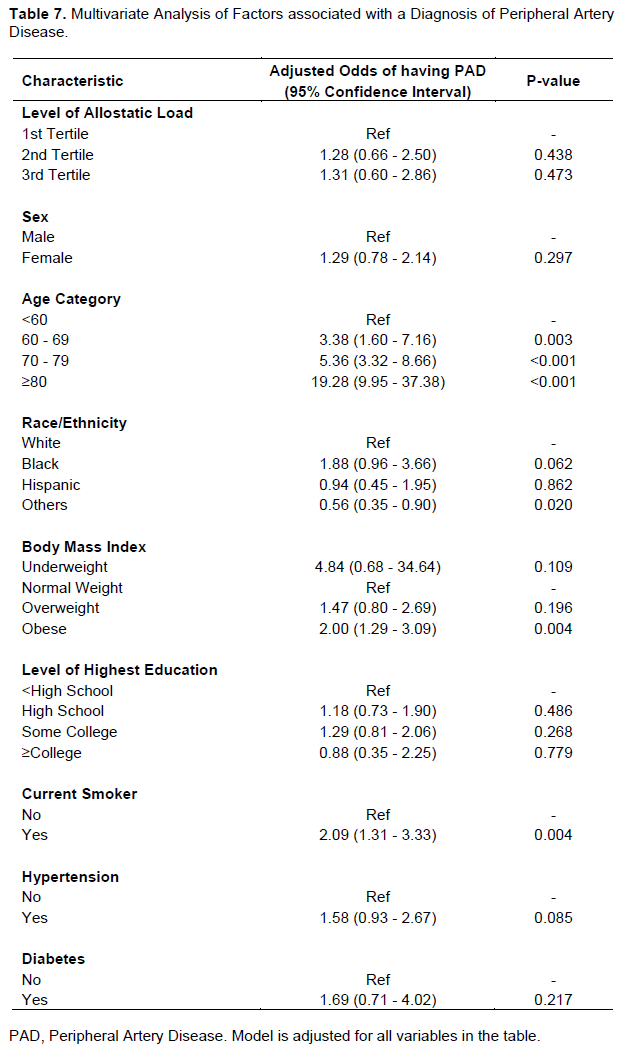
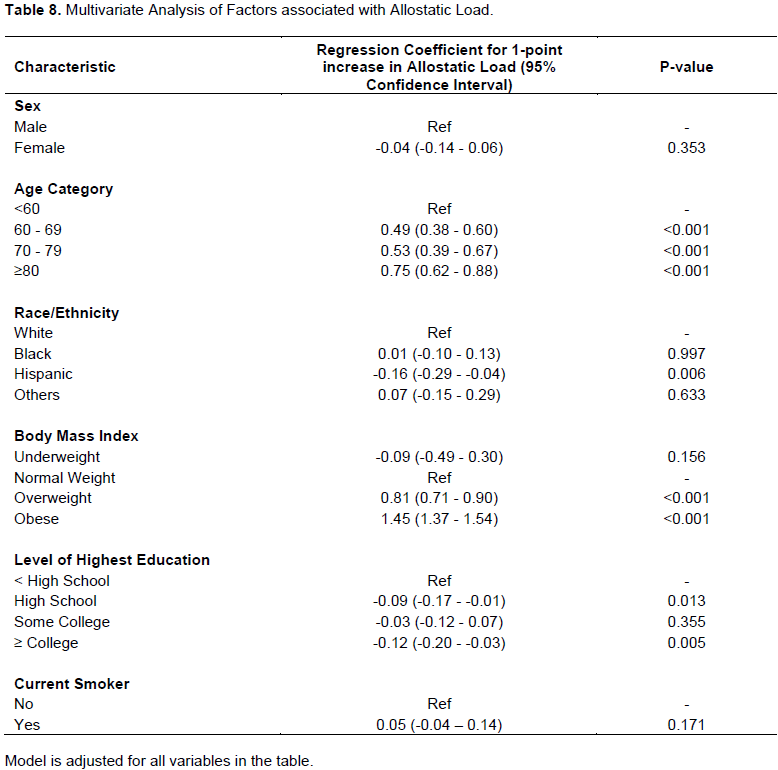
The 2003 - 2004 NHANES wave identified 5589 individuals. Since there are no well-defined cut-offs for allostatic load burden, the NHANES subjects were divided up into three equal groups (tertiles) based on their allostatic load scores and three tertiles of allostatic load severity were created: 1.5 to 3.5, 4 - 4.5 and 5 - 8.5. Demographic and clinical characteristics of survey respondents by level of allostatic load tertile are shown in Table 2. The sample had an equal split of male to female proportions for allostatic load scores representing the second and third tercile. Females, however predominated (54% female and 46% male) in the first tercile of allostatic load (< 4). Of these NHANES subjects, 239 (5.9%) individuals were diagnosed as having PADthat is, an ABI ≤ 0.9. Using survey weights, this would correspond to 5.9 million individuals. The likelihood of a PAD diagnosis appeared to be related to the level of allostatic load: 6% of the PAD cohort was in the first allostatic load tertile, 28% was in the second tertile and 71% was in the 3rd tertile. Furthermore, amongst individuals with PAD two-thirds were in the highest tertile of allostatic load burden/severity compared to only half of the non-PAD individuals in this highest tertile of allostatic load burden (Table 3). In each allostatic load tertile, the overwhelming majority (99%) of PAD diagnosed was mild or moderate (Table 4). The distribution of allostatic load components across levels of PAD severity is illustrated in Table 5. Multivariate analysis of factors associated with severity of PAD as well as regression coefficient for 1 decimal point increase in ABI are depicted in Table 6. A statistically significant association between allostatic load and PAD severity was not identified. A scatter plot depicting allostatic load and PAD severity shows a slight downward slope with correlation coefficient of -0.135 suggestive of little to no correlation. A multivariate analysis of factors associated with a diagnosis of PAD is shown in Table 7, and a multivariate analysis of factors associated with allostatic load is represented in Table 8.

DISCUSSION
The current study was unable to identify an association between PAD severity and allostatic load. The study, however, suggests that individuals with PAD tend to have higher allostatic load scores. This latter finding is consistent with the study by Nelson et al. (2007) using an earlier NHANES wave that showed that individuals with PAD had higher allostatic load scores. Furthermore, this corroborates the previously reported finding associating a higher PAD prevalence in the setting of a higher allostatic load (Eraso et al., 2014; Nelson et al., 2007). It is possible that the inability to conclusively prove an association within the confidence intervals could be a result of Type II Error. The small sample size of individuals with PAD of 239 representing only 5.9% of this NHANES wave may have simply been too small to conclusively uncover an existing association.
Allostatic load is a concept that refers to the biologic response of environmental stressors (Carlson and Chamberlain, 2005; Logan and Barksdale, 2008). It represents the cumulative effect of chronic “wear and tear” leading to a failure of allostasis that result in permanent pathophysiologic changes. This concept would also explain the phenomenon referred to as “The Biology of Poverty” - how poverty “gets under the skin”. This is the observation that prolonged exposure to deprivation in early childhood predisposes to certain biological changes that persist throughout life (Lupien et al., 2001). Other investigators have long described this phenomenon of “weathering” in Blacks related to the long-term effect of perceived discrimination (Geronimus, 1992). While there are several potential “upstream” factors that may lead to the development of allostasis leading to more severe PAD and potential future amputation, it has been suggested that allostatic load could be a mechanism of sociodemographic health disparities (Szanton et al., 2005). It has been reported that Blacks have a higher allostatic load burden as compared to whites independent of SES, and that this may explain negative health outcomes and higher mortality among Blacks (Duru et al., 2012). This current study supports this hypothesis, and places allostatic load as a likely candidate in the pathway of sociodemographic PAD disparities.
Some have suggested that the disparity in amputation-revascularization is largely as a result of socioeconomic status. There is a strong link between low socioeconomic status (as defined by education and/or income) and PAD.
There is also a positive correlation between low socioeconomic status and Black race. This is true both for educational attainment as well as for family income (Pande and Creager, 2014). In fact, certain authors have proposed that race may simply be a surrogate for socioeconomic status. It is postulated that lower
socioeconomic status, which is more commonly seen in Blacks than Whites and is correlated with decreased access to care, leads to delayed presentation of PAD which, in turn, results in this apparent race-dependent treatment selection for PAD (Ho et al., 2005; Nguyen and Henry, 2010). This implies that by the time Blacks with
PAD present to the physician/surgeon, it is too late to perform limb-saving revascularization procedures, leaving an amputation as the only available option for these patients. Some authors have submitted that it may not so much be individual SES that impacts negatively on one’s health, but rather socioeconomic neighborhood stress associated with living in a deprived neighborhood (Do et al., 2008; Sundquist et al., 2012, 2004). While there are significant similarities between the PAD disparities emanating from low SES and Black ethnicity, data, however, suggest that low SES and race are independent, though perhaps synergistic, factors contributing to worse outcomes for PAD (Henry et al, 2011). This pathway of allostatic load may serve as a common denominator explaining both race-based and SES-based amputation-revascularization disparities.
Under-treatment of risk factors has also been blamed for the existence of these amputation-revascularization disparities. Blacks have a significantly higher prevalence of traditional cardiovascular risk factors such as diabetes, hypertension and dyslipidemia as compared to Whites (Wong et al., 2002). Unfortunately, there is also significant evidence demonstrating that these key cardiovascular risk factors are often undertreated in Blacks. Hypertension is under-treated and the glycemic indices for Blacks undergoing treatment for diabetes mellitus are consistently higher than Whites (Malik et al., 2007). In addition, there is significant under-utilization of statins (Lipworth et al., 2014)in Blacks so that this population is not fully benefitting from the tremendous advantages of statins in combatting vascular disease. Furthermore, ever since Kevin Shulman’s 1999 landmark New England Journal of Medicine article portraying the effect of physician racial and gender bias in referring patients for cardiac catheterization (Schulman et al., 1999), the role of physician bias has been increasingly recognized as playing a role in healthcare disparities.
One key limitation of this second (NHANES) study is that the NHANES wave used 2003 - 2004 is relatively dated. These data were used, however, as this is the most recent NHANES wave that includes Doppler occlusion pressures that allow for the calculation of ABI. These data are particularly pertinent because a limitation of other, similar studies is their reliance on surrogates for PAD (such as clinical symptoms) while this current study uses ABI, the gold standard for PAD diagnosis (Conte et al., 2019). There, nonetheless remains a potential negative impact to using this 15-year old data. Indeed, data suggests that while overall national amputation rates have decreased over the past two decades, amputation rates among Blacks have not decreased (Goodney et al., 2015). This suggests that this amputation-revascularization disparity is at least as bad today as it was during the 2003-2004 NHANES survey period.
This study may also be considered to highlight the need for continued collection of this clinical data. Our study is unable to establish allostatic load as a factor in the pathogenesis of this amputation-revascularization disparity. It is possible that the inability to conclusively prove this as a factor could be as a result of Type II Error relating to a sample size that was simply too small. In addition to continued study of allostatic load in better-powered studies, additional investigations regarding the molecular mechanisms by which this disparity operates still need to be studied. Current data point to the potential pathways of inflammation (Libby et al., 2002; Sullivan et al., 2000) and endothelial dysfunction. In vitro and in vivo racial differences in inflammation have been identified (Feairheller et al., 2011)and Blacks, with early life adversity, have been noted to have high concentrations of inflammatory biomarkers in mid-life (Slopen et al., 2010). There are studies that suggest race-specific differences in endothelial function and a propensity of Blacks towards endothelial dysfunction (Freedman et al., 2000; Grubbs et al., 2002; Mulukutla et al., 2010; Qureshi et al., 2007). The multi-factorial nature of this health disparity indicates a highly complex process that spans health policy, health economics and medical care as well as biologic and cellular processes. This current study was unable to identify a clear association between PAD severity and allostatic load. Therefore, we were unable to establish allostatic load as a probable down-stream factor in the amputation-revascularization disparities pathway.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
This project was supported in part by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number 2U54MD007597.
REFERENCES
|
Beckie TM (2012). A systematic review of allostatic load, health, and health disparities. Biological Research for Nursing 14(4):311-346. |
|
|
Brothers TE, Robison JG, Sutherland SE, Elliott BM (1997). Racial differences in operation for peripheral vascular disease: results of a population-based study. Cardiovascular Surgery 5(1):26-31. |
|
|
Carlson ED, Chamberlain RM (2005). Allostatic load and health disparities: a theoretical orientation. Research in Nursing and Health 28(4):306-315. |
|
|
Conte MS, Bradbury AW, Kolh P, White JV, Dick F, Fitridge R, Joint GWG (2019). Global vascular guidelines on the management of chronic limb-threatening ischemia. European Journal of Vascular and Endovascular Surgery 58(1):S1-S109. |
|
|
Conte MS, Pomposelli FB, Clair DG, Geraghty PJ, McKinsey JF, Mills JL, Sidawy AN (2015). Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: management of asymptomatic disease and claudication. Journal of Vascular Surgery 61(3):2S-41S. |
|
|
Criqui MH, Vargas V, Denenberg JO, Ho E, Allison M, Langer RD, Fronek A (2005). Ethnicity and peripheral arterial disease: the San Diego Population Study. Circulation 112(17):2703-2707. |
|
|
Davis AM, Vinci LM, Okwuosa TM, Chase AR, Huang ES (2007). Cardiovascular health disparities. Medical Care Research and Review 64(5):29S-100S. |
|
|
Do DP, Finch BK, Basurto-Davila R, Bird C, Escarce J, Lurie N (2008). Does place explain racial health disparities? Quantifying the contribution of residential context to the Black/white health gap in the United States. Social Science and Medicine 67(8):1258-1268. |
|
|
Duru OK, Harawa NT, Kermah D, Norris KC (2012). Allostatic load burden and racial disparities in mortality. Journal of the National Medical Association 104(1-2):89-95. |
|
|
Eraso LH, Fukaya E, Mohler III ER, Xie D, Sha D, Berger JS (2014). Peripheral arterial disease, prevalence and cumulative risk factor profile analysis. European Journal of Preventive Cardiology 21(6):704-711. |
|
|
Feinglass J, Abadin S, Thompson J, Pearce WH (2008). A census-based analysis of racial disparities in lower extremity amputation rates in Northern Illinois, 1987-2004. Journal of Vascular Surgery 47(5):1001-1007. |
|
|
Feinglass J, Kaushik S, Handel D, Kosifas A, Martin GJ, Pearce WH (2000). Peripheral bypass surgery and amputation: northern Illinois demographics, 1993 to 1997. Archives of Surgery 135(1):75-80. |
|
|
Freedman BI, Yu H, Anderson PJ, Roh BH, Rich SS, Bowden DW (2000). Genetic analysis of nitric oxide and endothelin in end?stage renal disease. Nephrology Dialysis Transplantation 15(11):1794-1800. |
|
|
Geronimus AT (1992). The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethnicity and Disease 2(3):207-221. |
|
|
Goodney PP, Tarulli M, Faerber AE, Schanzer A, Zwolak RM (2015). Fifteen-year trends in lower limb amputation, revascularization, and preventive measures among medicare patients. JAMA Surgery 150(1):84-86. |
|
|
Grubbs AL, Anstadt MP, Ergul A (2002). Saphenous vein endothelin system expression and activity in African American patients. Arteriosclerosis, thrombosis, and Vascular Biology 22(7):1122-1127. |
|
|
Guadagnoli E, Ayanian JZ, Gibbons G, McNeil BJ, LoGerfo FW (1995). The influence of race on the use of surgical procedures for treatment of peripheral vascular disease of the lower extremities. Archives of Surgery 130(4):381-386. |
|
|
Hayanga AJ, Kaiser HE, Sinha R, Berenholtz SM, Makary M, Chang D (2009). Residential segregation and access to surgical care by minority populations in US counties. Journal of the American College of Surgeons 208(6):1017-1022. |
|
|
Henry AJ, Hevelone ND, Belkin M, Nguyen LL (2011). Socioeconomic and hospital-related predictors of amputation for critical limb ischemia. Journal of Vascular Surgery 53(2):330-339. |
|
|
Ho V, Wirthlin D, Yun H, Allison J (2005). Physician supply, treatment, and amputation rates for peripheral arterial disease. Journal of Vascular Surgery 42(1):81-87. |
|
|
Huber TS, Wang JG, Wheeler KG, Cuddeback JK, Dame DA, Ozaki CK, Seeger JM (1999). Impact of race on the treatment for peripheral arterial occlusive disease. Journal of vascular surgery 30(3):417-425. |
|
|
Hughes K, Boyd C, Oyetunji T, Tran D, Chang D, Rose D, Obisesan T (2014). Racial/ethnic disparities in revascularization for limb salvage: an analysis of the National Surgical Quality Improvement Program database. Vascular and Endovascular Surgery 48(5-6):402-405. |
|
|
Kressin NR, Chang BH, Whittle J, Peterson ED, Clark JA, Rosen AK, Petersen LA (2004). Racial differences in cardiac catheterization as a function of patients' beliefs. American Journal of Public Health 94(12):2091-2097. |
|
|
Libby P, Ridker PM, Maseri A (2002). Inflammation and atherosclerosis. Circulation 105(9):1135-1143. |
|
|
Lipworth L, Fazio S, Kabagambe EK, Munro HM, Nwazue VC, Tarone RE, Sampson UK (2014). A prospective study of statin use and mortality among 67,385 blacks and whites in the Southeastern United States. Clinical Epidemiology 6:15-25. |
|
|
Logan JG, Barksdale DJ (2008). Allostasis and allostatic load: expanding the discourse on stress and cardiovascular disease. Journal of Clinical Nursing 17(7B):201-208. |
|
|
Lupien SJ, King S, Meaney MJ, McEwen BS (2001). Can poverty get under your skin? Basal cortisol levels and cognitive function in children from low and high socioeconomic status. Development and Psychopathology 13(3):653-676. |
|
|
Malik S, Lopez V, Chen R, Wu W, Wong ND (2007). Undertreatment of cardiovascular risk factors among persons with diabetes in the United States. Diabetes Research and Clinical Practice 77(1):126-133. |
|
|
Mulukutla SR, Venkitachalam L, Bambs C, Kip KE, Aiyer A, Marroquin OC, Reis SE (2010). Black race is associated with digital artery endothelial dysfunction: results from the Heart SCORE study. European Heart Journal 31(22):2808-2815. |
|
|
National Center for Health Statistics (NCHS), Centers for Disease Control and Prevention (2003 - 2004). National Health and Nutritional Examination Survey Retrieved from https://www.cdc.gov/nchs/nhanes/index.htm |
|
|
Nelson A (2002). Unequal treatment: confronting racial and ethnic disparities in health care. Journal of the National Medical Association 94(8):666-668. |
|
|
Nelson KM, Reiber G, Kohler T, Boyko EJ (2007). Peripheral arterial disease in a multiethnic national sample: the role of conventional risk factors and allostatic load. Ethnicity and Disease 17(4):669-675. |
|
|
Nguyen LL, Henry AJ (2010). Disparities in vascular surgery: is it biology or environment?. Journal of vascular surgery 51(4):S36-S41. |
|
|
Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG (2007). Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). Journal of Vascular Surgery 45:S5-67. |
|
|
Pande RL, Creager MA (2014). Socioeconomic inequality and peripheral artery disease prevalence in US adults. Circulation: Cardiovascular Quality and Outcomes 7(4):532-539. |
|
|
Qureshi G, Brown R, Salciccioli L, Qureshi M, Rizvi S, Farhan S, Lazar J (2007). Relationship between aortic atherosclerosis and non-invasive measures of arterial stiffness. Atherosclerosis 195(2):190-194. |
|
|
Regenbogen SE, Gawande AA, Lipsitz SR, Greenberg CC, Jha AK (2009). Do differences in hospital and surgeon quality explain racial disparities in lower-extremity vascular amputations? Annals of Surgery 250(3):424-431. |
|
|
Rodriquez EJ, Livaudais-Toman J, Gregorich SE, Jackson JS, Nápoles AM, Pérez-Stable EJ (2018). Relationships between allostatic load, unhealthy behaviors, and depressive disorder in US adults, 2005-2012 NHANES. Preventive Medicine 110:9-15. |
|
|
Schulman KA, Berlin JA, Harless W, Kerner JF, Sistrunk S, Gersh BJ, Escarce JJ (1999). The effect of race and sex on physicians' recommendations for cardiac catheterization. New England Journal of Medicine 340(8):618-626. |
|
|
Sidawy AN, Schweitzer EJ, Neville RF, Alexander EP, Temeck BK, Curry KM (1990). Race as a risk factor in the severity of infragenicular occlusive disease: study of an urban hospital patient population. Journal of Vascular Surgery 11(4):536-543. |
|
|
Slopen N, Lewis TT, Gruenewald TL, Mujahid MS, Ryff CD, Albert MA, Williams DR (2010). Early life adversity and inflammation in African Americans and whites in the midlife in the United States survey. Psychosomatic Medicine 72(7):694-701. |
|
|
Soden PA, Zettervall SL, Deery SE, Hughes K, Stoner MC, Goodney PP (2018). Society for Vascular Surgery Vascular Quality Initiative. Black patients present with more severe vascular disease and a greater burden of risk factors than white patients at time of major vascular intervention. Journal of Vascular Surgery 67(2):549-556. |
|
|
Stapleton SM, Bababekov YJ, Perez NP, Fong ZV, Hashimoto DA, Lillemoe KD, Chang DC (2018). Variation in amputation risk for black patients: uncovering potential sources of bias and opportunities for intervention. Journal of the American College of Surgeons 226(4):641-649. |
|
|
Sullivan GW, Sarembock IJ, Linden, J. (2000). The role of inflammation in vascular diseases. Journal of Leukocyte Biology 67(5):591-602. |
|
|
Sundquist J, Li X, Sundquist K (2012). Neighborhood deprivation and mortality in individuals with cancer: a multilevel analysis from Sweden. European Journal of Cancer Prevention 21(4):387-394. |
|
|
Sundquist K, Malmstrom M, Johansson SE (2004). Neighbourhood deprivation and incidence of coronary heart disease: a multilevel study of 2.6 million women and men in Sweden. Journal of Epidemiology and Community Health 58(1):71-77. |
|
|
Szanton SL, Gill JM, Allen JK (2005). Allostatic load: a mechanism of socioeconomic health disparities? Biological Research For Nursing 7(1): 7-15. |
|
|
Wong MD, Shapiro MF, Boscardin WJ, Ettner SL (2002). Contribution of major diseases to disparities in mortality. The New England Journal of Medicine 347(20):1585-1592. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


