Full Length Research Paper

ABSTRACT
A clinico-laboratory investigation of multidrug resistant (MDR) characteristics of extended spectrum β-lactamase (ESBL) producing Escherichia coli pathotypes from some hospitals in Bauchi metropolis, Nigeria, was carried out. A total of 198 E. coli isolates were recovered from different patients’ age group (0 to above 70 years), comprising of 134 males and 85 females, as both out-patient (126) and in-patient (93). The antimicrobial susceptibility tests show a high multidrug resistance among Ampicillin (97.0%), Amoxycillin (96.0%), the newer generation Cephalosporins like Cefuroxime (81.3%), Cefotaxime (85.4%) and Ceftazidime (60.6%). The isolates were sensitive to Ceftriaxone (62.1%), Amikacin (71.7%) and Imipenem (80.8%). Out of the multidrug resistant isolates, 163 were ESBL producers, with frequency of (26.9%) found within age group (31 to 40 years), mostly in males (59.1%) and out-patients (51.5%). Fifty four (27.3%) of the isolates were recovered from stool specimens with MDR and ESBL prevalence of (27.1%) and (26.9%) respectively. Based on clinical diagnosis, prevalence of MDR (29.5%) and ESBL production (28.2%) was found among cases of Urinary tract infections (UTIs), followed by Gastroenteritis (25.3%) and (25.8) respectively. These results indicate a strong association between multidrug resistance and ESBL production in E. coli pathotypes. The Amikacin and Imipenem sensitivity in this study advocates the usage of the carbapenem as the therapeutic alternative in the event of the increasing resistance rates observed with conventional beta-lactam antibiotics.
Key words: Multidrug resistant (MDR), extended spectrum β-lactamase (ESBL), urinary tract infections (UTIs), gastroenteritis, carbapenem, beta-lactam antibiotics.
INTRODUCTION
Escherichia coli is one of the most important opportunistic Gram negative bacteria, resistant to many antimicrobial agents and cause different infections possession of many virulence genes encoding to some important virulence factors (Baker et al., 2017). It is a major human pathogen, causing up to 80% of uncomplicated UTI and 30% of bacteraemia cases (Ejikeugwu et al., 2012). E. coli strains can be separated into three broad groups based on interaction with their host: commensal, intestinal/diarrhoeagenic, and extraintestinal pathogenic strains.
Diarrhoeagenic Escherichia coli (DEC) are major causes of gastroenteritis in children in the developing world and are associated with high resistance levels to antibiotics. E. coli associated with diarrhoea have been classified into seven groups based on clinical, epidemiologic, and molecular criteria: enteropathogenic E. coli (EPEC); enterotoxigenic E. coli (ETEC); Shiga toxin-producing E. coli (STEC), also known as enterohaemorrhagic E. coli (EHEC) or verotoxin-producing E. coli (VTEC); enteroinvasive E. coli (EIEC); enteroaggregative E. coli (EAEC); and diffusely adherent E. coli (DAEC), Cell detaching effacing E. coli (CDEC) and Cytolethal distending toxin-producing E. coli (CLDTEC). The most commonly encountered strains are the EHEC and EPEC strains capable of causing life threatening diseases (Ochoa et al., 2009; Rono et al., 2015).
Acute or chronic diarrhoea caused by different pathotypes of E. coil is an emerging problem in many parts of the world. In developing countries more than 77% of diarrhoeagenic E. coli strains were resistant to the commonly used antibiotics with high minimum inhibitory concentration. The four pathotypes of intestinal E. coli, EPEC, ETEC, EHEC and EAEC, had a high prevalence of multidrug resistance especially to ampicillin and chloramphenicol (Aibinu et al., 2003). Diarrhoeagenic E.coli remain an important aetiological agent of infantile diarrhoea in Nigeria (Okeke et al., 2005).
Extraintestinal pathogenic E. coli (ExPEC) causes extraintestinal infections with high incidence of morbidity and mortality (Al-Mayahie et al., 2011). The strains of E. coli that cause extra-intestinal infections are an increasingly important endemic problem and they are under-appreciated as killers (Pitout, 2010). Extra-intestinal pathogenic E. coli (ExPEC) are responsible for urinary tract, intra-abdominal and soft tissue infections, meningitis, pneumonia and osteomyelitis and they are often associated with bacteraemia (Chakraborty et al., 2012). As one of the most common gram-negative blood culture isolates in hospitalized patients, E. coli has become a very important pathogen associated with hospital infection (Nagdeo et al., 2012).
In a clinical setting, E. coli infections are treated with beta-lactam antibiotics, whose extensive use has led to emergence of extended-spectrum beta-lactamases (ESBLs) producing strains (Drawz et al., 2014). ESBLs are enzymes produced by Gram-negative bacilli that have the ability to hydrolyze beta-lactam antibiotics containing an oxyimino group. In Gram-negative bacteria, the production of beta-lactamases represents the most important contributing factor to resistance against beta-lactam antibiotics (Olusolabomi et al., 2011; Hansen et al., 2016). During the last couple of years increasing numbers of antibiotic-resistant bacteria have become a problem in the field of infection control. Pathogenic E. coli constitutes a significant threat to public health, and the emergence of extended-spectrum beta-lactamase (ESBL)-producing E. coli with high virulence potential is alarming (Umadevi et al., 2011; Chakraborty et al., 2012; Baker et al., 2017).
Antimicrobial resistance is a growing threat worldwide. Resistance mechanisms have been found for every class of antibiotic agents. The predominant mechanism for resistance to the β-lactam antibiotics in gram-negative bacteria such as E. coli is the production of β-lactamase (Zasowski et al., 2015; Wright, 2016). The production of extended-spectrum β-lactamases (ESBLs) is an important mechanism which is responsible for the resistance to the third-generation cephalosporins. During the last 2 decades, ESBL producing gram-negative bacilli have emerged as a major problem in many settings (Motayo et al., 2012). The problems which are associated with ESBLs include multidrug resistance, difficulty in detection and treatment, and increased mortality. Multidrug-resistant E. coli (MDR-ECO) strains have increased with the application of broad-spectrum antibiotics (Saeidi et al., 2014; Baker et al., 2017).
ESBL-producing bacteria have been reported increasingly worldwide. They cause many clinical diseases including urinary tract infections, peritonitis, cholangitis and intra-abdominal abscess (Yazdi et al., 2012). The incidence of ESBL producing strains of E. coli among clinical isolates has been steadily increasing over the past few years resulting in limitation of therapeutic options (Olowe and Aboderin, 2010; Rajan and Prabavathy, 2012; Drawz et al., 2014). Therefore, this study was aimed to determine the multidrug resistant characteristics of ESBL-producers among the intestinal and extra-intestinal E. coli pathotypes from clinical samples.
MATERIALS AND METHODS
Study design
This research is a clinico-laboratory investigation of multidrug resistant characteristics of extended spectrum β-lactamase (ESBL) producing E. coli pathotypes in Bauchi State, Nigeria.
Subjects
The research includes all categories of patients with clinical illness on hospital admission or outpatient treatment in some hospitals in Bauchi metropolis. For intestinal E. coli, the target group were mainly children patients, aged between 1 and 5 years; diagnosed by a physician as having acute diarrhoea, on the basis of frequent watery, or bloody stools (usually more than three times daily (WHO, 2012).
Clinical variables such as age, gender, patient group and underlying medical conditions/clinical diagnosis were collected from the patients. Bacteraemia were recorded as hospital-acquired, in case of blood culture collected less than 48 h after admission of the patients. In cases of UTI patients who receive antimicrobial drugs during the past one month was excluded from this study. Control subjects were apparently healthy subjects of the same age range, with no history of diarrhoea for at least one month, including those on immunization, medical check-up and antenatal visit.
In general, only those patients whose samples (stool, urine, blood, swabs, CSF,) that produce E. coli were selected for this study. Informed consent was obtained from each subject participant (where possible). Ethical clearance was obtained before collecting samples, patient clinical data and demographic details.
Sample size determination
The sample size was determined using the formula derived by Hawkey (2008) as described by Yasmin et al. (2012).

Where: n= Desired sample size, p= Previous prevalence of the disease in a community,
q= (1-p), d= 0.05 (Degree of accuracy), Z = 1.96 (for 95% confidence level).
Prevalence rate of 17.2% (0.172) in a similar study by Yusuf and Haruna (2013) was considered as the previous prevalence used in this study.
Sample collection
A total of two hundred and nineteen (219) samples were collected for this study, according to standard laboratory techniques as described by Vandepitte et al. (2003), Mahon et al. (2007), Chessbrough, (2012). Fifty four (54) stool samples/rectal swabs were collected from patients (mainly children between less than 1 – 5 years old) with cases of acute diarrhoea. One hundred and sixty five (165) urine, blood, swabs, cerebrospinal fluid (CSF) and sputum samples were collected from patients with cases of extraintestinal infections.
Sample processing
Faecal samples appearance were examined and recorded for presumptive diagnosis of E.coli diarrhoeal/intestinal infections. The samples were inoculated onto MacConkay (MAC) and Eosine methylene Blue (EMB) agar media (Biotech). Bloody watery stool samples were inoculated onto Sorbitol MacConkay (SMAC) agar media for detecting suspected cases of haemorrhagic colitis due to Enterohaemorrhagic E.coli (EHEC)/verotoxin, E. coli (VTEC) 0157.
The urine samples were inoculated onto MacConkay (MAC) and Cystein Lactose Electrolyte Deficient (CLED) agar media (Biotech). The appearance of the urine samples were examined and recorded. Only cloudy and/or smelly urine were considered significant for this study. The blood samples from septicaemic patients collected by peripheral veni-puncture were inoculated into Brain heart infusion (BHI) broth (Neogen) and processed in BACTEC 9050 (Becton Dickinson, USA). The resulting growth were sub-cultured onto MacConkay (Difco/BD Diagnostics Systems, Sparks, MI, USA) and Blood agar media (Oxoid Ltd, Basingstoke, UK), as described by Vandepitte et al. (2003) and Cheesbrough (2012).
Morphological Identification and Microscopy
The culture plates were incubated at 37°C for 18 to 24 h and then examined for typical morphological characteristics of E. coli. Further colony identification was made by Gram stain and microscopy according to the method of Mackenzie (2004).
Biochemical identification methods
The isolates were confirmed by indole production, methyl red; citrate utilization and urease tests as described by Mackenzie (2004) and Chessbrough (2012).
Antibiotic susceptibility testing
This was done on nutrient agar plates inoculated with 0.5 McFarland standard inoculums using modified Kirby-Bauer disk diffusion method as described by Mahon et al. (2007); Cheesbrough (2012). Commonly used antibiotics in our area were selected and tested; these include multidisc, Ampicillin (10 µg), Amoxycillin (25 µg), Erythromycin (25 µg), Tetracycline (30 µg), Cotrimoxazole (25 µg), Streptomycin (10 µg), Gentamycin (10 µg), Amoxicillin/Clavulanate (30 µg), Nalidixic acid (30 µg), Ciprofloxacin (30 µg), Nitrofurantoin (300 µg), Imipenem (10 µg) (Mast Diagnostics, U.K.) and single disks Cefuroxime (30 µg), Cefotaxime (30 µg) Ceftazidime (30 µg), Ceftriaxone(30 µg), Amikacin (30 µg) (Oxoid U.K.). The results were interpreted according to CLSI guidelines (2012).
Detection of ESBL producing E. coli by double disk synergy test (DDST)
The E. coli isolates resistant to two or more of the third generation cephalosporins were tested phenotypically for ESBL production by Double Disk Synergy Test (DDST) as described by Mackenzie (2004) and Iroha et al. (2008).
A suspension of the ESBL-producing E. coli isolate adjusted to 0.5 McFarland turbidity standards were aseptically inoculated on Muller-Hinton agar (Oxoid, UK) plate using sterile swab sticks. With the help of a template, a combination disk of amoxycillin-clavulanic acid, AMC (20/10 μg) was placed at the centre of the plate and cefotaxime (30 μg), ceftriazone (30 μg) and ceftazidime (30 μg) disks were each placed on either sides of the central disk (AMC-20/10 μg) at a distance of 15 mm apart. The plates were incubated for 18 to 24 h at 37°C. After incubation, a ≥5 mm increase in zone diameter for either of the cephalosporins (CEF and CTX) tested in combination with AMC (20/10 μg) compared to its zone when tested alone, phenotypically confirms ESBL production in the test isolate (CLSI, 2012).
RESULTS
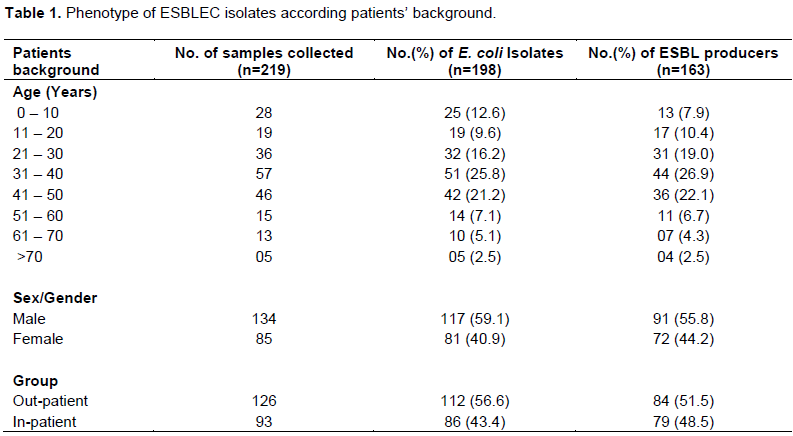
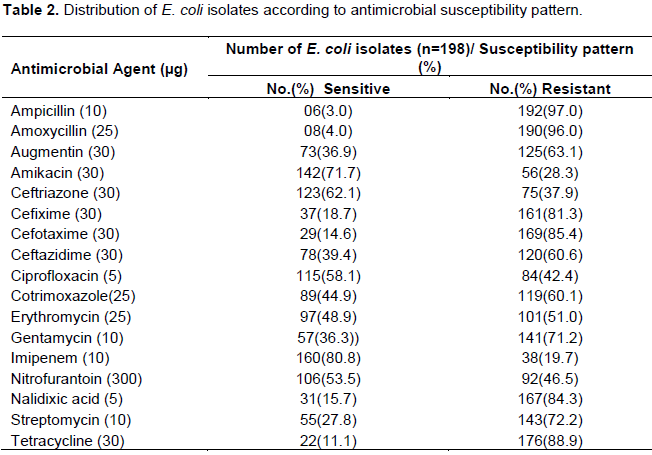
In this study, a total of 198 E. coli isolates were recovered from 219 clinical specimens (stool, urine, swabs, sputum, blood, and CSF) from different group of patients attending some hospitals in Bauchi metropolis, using standard bacteriological laboratory techniques. A 163 ESBL producers were isolated (Table 1) from different age group (1 to 70 years), comprising of 134 males and 85 females, as both out-patient (126) and in-patient (93). Highest frequency of ESBL producers (26.9%) was found within age group (31 to 40 years), mostly in males (59.1%) and out-patients (51.5%)(Table 2). In this study, high multidrug resistance was observed among such Beta lactam drugs as Ampicillin (97.0%), Amoxycillin (96.0%), the newer generation Cephalosporins like Cefuroxime (81.3%), Cefotaxime (85.4%) and Ceftazidime (60.6%). The isolates were sensitive to Ceftriazone (62.1%), Amikacin (71.7%) and Imipenem (80.8%) (Tables 3 and 4).
DISCUSSION
The presence of multidrug resistance in this study may be related to the dissemination of antibiotic resistance among hospital isolates of E. coli, as it is one of the main bacterial pathogens responsible for nosocomial infections especially in immunocompromised patients. A high sensitivity of E. coli strains to imipenem has been previously reported by Shahid et al. (2012). It seems this antibiotic can serve as a medication of choice for the treatment of UTI caused by E. coli. However, it should be noted that unlimited use of a medicine can gradually lead to rising antibiotic resistance.
The results of antibiotic susceptibility pattern in our study are consistent with the previous studies of Kukanur et al. (2015) on drug resistance in E. coli, where their study revealed that 92.5, 75 and 57.1% of E. coli isolates were sensitive to nitrofurantoin, amikacin and gentamicin respectively. Among pus and sputum samples amikacin was highly sensitive (100%). The greater prevalence of resistance to common antibiotics has also been reported by Mohajeri et al. (2014), where maximum number of isolates (100%) was resistant to ampicillin, carbenicillin and ceftazidime and the lowest to chloramphenicol (37%).
The result of similar study by Enwuru et al. (2011) showed relatively low resistance to ceftazidime, Ofloxacin, gentamycin, nitrofurantoin and Nalidixic acid by E. coli in the community, when compared with the pattern from the hospital. The indication may imply that these drugs have not been grossly misused in the vicinity studied. Therefore, they may still be useful for treating uncomplicated cases where E. coli is indicated as aetiological agents of diseases in hospital settings. Hospital-acquired infections by these agents may require a different approach since they have shown in vitro resistance patterns that may require alternative drugs or in combination with other drugs.
Resistance of bacteria like E. coli to most antibiotics used was seen as a consequence of excessive antibiotic use. The emergence of antibiotic resistant pathogenic bacteria is becoming an increasingly worrying clinical problem. It has been caused by the widespread use, and sometimes abuse of antibiotics not only in medical practice but also in animal husbandry where the antibiotics are frequently used as prophylactics and chemotherapeutics (Zhang et al., 2010). Inappropriate antibacterial treatment and abuse of the antibiotics in our area have also contributed to the emergence of antibacterial-resistant bacteria. Self-prescription of antibacterials is an example of antibiotic abuse. High resistance against these commonly used antibacterials is certainly worrisome. Therefore these drugs should no longer be prescribed as initial empirical therapy but unfortunately these antibiotics are yet being prescribed as first line drugs in the developing countries.
Other drugs that appeared to be clinically useful were the first-generation cephalosporin (cephradine), nalidixic acid, gentamycin and nitrofurantoin. The presence of multidrug resistance may be related to the dissemination of antibiotic resistance among hospital isolates of E. coli. The rate of ESBL production by E. coli in our study may be due to the selective pressure imposed by extensive use of antimicrobials. The indiscriminate use of cephalosporins is responsible for the high rate of selection of ESBL producing microorganisms ((Boschi-Pinto et al, 2008).
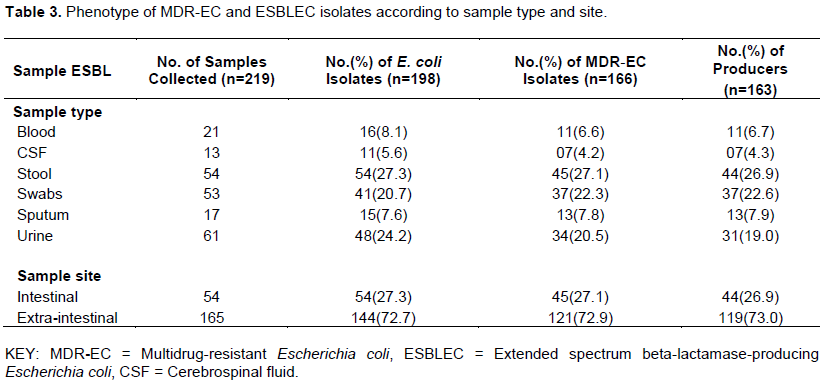
In our study, out of the 198 E. coli isolates, 54(27.3%) were recovered from stool specimens with MDR and ESBL prevalence of (27.1%) and (26.9%) respectively (Table 3). This is followed by 48 (24.2%) from the urine specimens of patients with various urinary tract infections (UTIs), with CSF as the least 11(5.6%). A 72.7% of the isolates are from exraintestinal sites (mainly genitourinary tract), with MDR and ESBL prevalence of 72.9 and 73.0% respectively. This indicates a strong relationship between multidrug resistance and ESBL production. The rate of ESBL production by E. coli may be due to the selective pressure imposed by extensive use of antimicrobials. The indiscriminate use of cephalosporins is responsible for the high rate of selection of ESBL producing microorganisms ((Boschi-Pinto et al, 2008; Fakruddin et al., 2013).
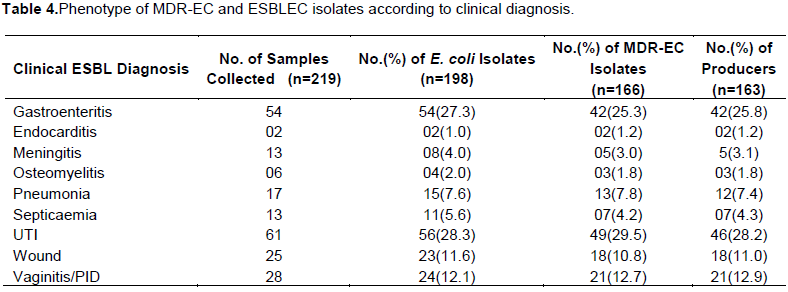
In the present study, prevalence of Multidrug resistance (29.5%) and extended spectrum beta-lactamase production (28.2%) was found among cases of Urinary tract infection, followed by Gastroenteritis (25.3%) and (25.8) respectively (Table 4). This study found that the two infections are mainly caused by pathogenic E. coli, as the organisms is commonly acquired through oral faecal route and is a commensal bacteria human gut, that can be virulent. According to Mohajeri et al. (2014), UPEC are a major cause of UTIs and may be responsible for approximately 90% of UTIs.
E. coli are the principal bacterial pathogen in childhood diarrhoea and constitute an important public health problem, especially in developing countries. Diarrhoeagenic E. coli strains often display resistance to beta-lactams due to the production of extended-spectrum beta-lactamases (ESBLs). Enterovirulent E. coli are among the most important causes of acute diarrhoea in developing as well as in developed countries (Kukanur et al., 2015). E. coli is an emerging agent among pathogens that cause diarrhoea (Nguyen et al., 2005). Most of ESBL producers are from male (37.4%) out-patient (32.1%) suffering from gastroenteritis. This is followed by female (31.9%) out-patient (29.1%) with diagnosis of UTIs.
Other important ESBLEC isolates observed are those associated with Vaginitis/PID (29.2%) and wound infections (16.4%) in the patients. Women are especially prone to UTIs for anatomical reasons with the life time risk of having a UTI is greater than 50% (Annapurna et al., 2014). UTIs in men are not as common as in women but can be serious when they occur. The main causal agent in upper and lower urinary tract infection is E. coli. UTI is predominantly a disease of the females, because of the anatomy of the female urethra. The incidence of bacteriuria increases during pregnancy, due to the anatomical and the hormonal changes. In most of the hospitalized patients, nearly all the UTIs are preceded by the instrumentation of the urinary tract, mainly urinary catheterization and it is a frequent cause of significant morbidity, sepsis and death (Shruthi et al., 2012).
CONCLUSION
The findings of this study indicate a strong association between multidrug resistance and ESBL production in E. coli pathotypes, as well as age and gender of patients due to drugs usage. Emergence of multidrug resistant (MDR) E. coli has an increasing trend and is a significant clinical challenge, because of limited therapeutic option for this pathogen. Therefore early detection of MDR and Extended spectrum beta lactamase producing E. coli is important to restrict their spread in community. There is need for continuous monitoring of antibiotic susceptibility in E. coli isolates and the resistant isolates to be routinely screened for different kinds of easily detectable virulence factors and beta lactamases to update the characteristics and new types of resistance mechanisms emerging in E. coli. It is essential to report ESBL production along with the routine sensitivity reporting, which will help the clinicians in prescribing proper antibiotics.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Aibinu IE, Ohaegbulam VC, Adenipekun EA, Ogunsola FT, Odugbemi TO, Mee BJ (2003). Extended-Spectrum β-Lactamase Enzymes in Clinical Isolates of Enterobacter Species from Lagos, Nigeria, Journal of Clinical Microbiology 41(5):2197-2200. |
|
|
Al-Mayahie SM, Al-Jafary AE, Al-Kafajy AM, Al-Maliky ZA, Al Swadi HA and Al-Qurbawi JS (2011). Detection of Extraintestinal Pathogenic Escherichia coli among Normal Stool Flora of Young, Healthy, Unmarried Males and Females as Predisposing Factor to Extraintestinal Infections: A Comparative Study. Baghdad Science Journal 8(1):81-90. |
|
|
Annapurna YV, Swapna BR, Lakshmi VV (2014). Multidrug Resistance and Virulence Phenotypes Among Uropathogenic Escherichia coli. International Journal of Current Microbiology and Applied Sciences 3(6):222-229. |
|
|
Baker KR, Sigurdardottir HH, Jana B, Guardabassi L (2017). Cephem potentiation by inactivation of nonessential genes involved in cell wall biogenesis of β-lactamase-producing Escherichia coli. Antimicrobial Agents and Chemother 6(1):66 -71 . |
|
|
Boschi-Pinto C, Velebit L, Shibuya K (2008). Estimating child mortality due to diarrhoea in developing countries, Bull World Health Organization 86:710-717. |
|
|
Chakraborty A, Adhikari P, Shenoy S, Baliga S, Rao S, Dhanashree B (2012). Extra-intestinal β-lactamase Producing Escherichia coli Infection-an Emerging Infection in a South Indian Tertiary Care Hospital. Journal of Clinical and Diagnostic Research 6(7):1210-1214. |
|
|
Cheesbrough M (2012). District Laboratory Practice in Tropical Countries. Part two (2), Cambridge University Press, Cambridge, UK. |
|
|
Clinical Laboratory Standards Institute (2012). Performance Standards for Antimicrobial Susceptibility Testing: 22nd international supplement. (M100-S22). CLSI, Wayne, PA, USA. |
|
|
Drawz SM, Papp –Wallace KM, Bonomo RA (2014). New beta-lactamase inhibitors: a therapeutic renaissance in an MDR world. Antimicrobial Agents and Chemotherapy 58:1835-1846. |
|
|
Enwuru NV, Enwuru CA, Ogbonnia SO, Adepoju-Bello AA (2011). Metallo-Β-Lactamase Production by Escherichia Coli and Klebsiella Species Isolated from Hospital and Community Subjects in Lagos, Nigeria. Nature and Science 9(11):1-5. |
|
|
Ejikeugwu PC, Ikegbunam NM, Ugwu, CM, Iroha, IR, Esimone CO (2012). Extended-Spectrum β-Lactamase-Producing Escherichia coli isolates from Suspected Community Acquired Urinary Tract Infections. European Journal of Scientific Research 84(4):565-571. |
|
|
Fakruddin MD, Mohammad R, Mazumdar A, Chowdhury I, Shahnewaj K (2013). A preliminary study on virulence factors & antimicrobial resistance in extra intestinal pathogenic Escherichia coli (ExPEC) in Bangladesh. Indian Journal of Medical Research 137:988-990. |
|
|
Hassan AS, Jamal AS, Kamal M (2013). Occurrence of Multidrug Resistant and ESBL Producing E.coli Causing Urinary Tract Infections, Journal of Basic and Applied Sciences 7(1):39-43. |
|
|
Hawkey PM (2008). Prevalence and clonality of extended-spectrum beta-lactamases in Asia, Clinical Microbiology and Infection 14:159-165. |
|
|
Hansen KH, Bortolaia V, Nielsen CA, Nielsen JB, Schonning K, Agerso Y and Guardabassi L (2016). Host-specific patterns of genetic diversity among IncI1-I and IncK plasmids encoding CMY-2 Beta-lactamase in Escherichia coli isolates from humans, poultry meat, poultry and dogs in Denmark. Applied and Environmental Microbiology 82:4705-4714. |
|
|
Iroha IR, Amadi SE, Adikwu MU, Esimone CO (2008). Detection of Plasmid Borne Extended spectrum Beta – Lactamase enzymes in clinical isolates of Escherichia coli from a community General Hospital. International Journal of Molecular Medicine and Advance Sciences 4(2):46-49. |
|
|
Kai M, Park T, Choi BY, Foxman B (2004). The epidemiology of acute pyelonephritis in South Korea, 1997-1999. American Journal of Epidemiology 160(10):985-993. |
|
|
Kukanur S, Meundi M, Bajaj A, Kotigadde S (2015). Co-Relation between Virulence Factors and Antibiotic Resistance of E. coli, With Special Reference to Uropathogenic E. coli. IOSR Journal of Dental and Medical Sciences 14(3):15-21. |
|
|
Li S, Qu Y, Hu D, Shi Y (2012). Comparison of extended spectrum beta-lactamases producing Escherichia coli with non-ESBLs producing E.coli: drug-resistance and virulence. World Journal of Emergency Medicine 3(3):208-212. |
|
|
Mohajeri P, Khademi H, Ebrahimi R, Farahani A, Razeai M (2014). Frequency distribution of Virulence factors in Uropathogenic E. coli Isolated from Kermanshah in 2011- 2012, International Journal of Applied and Basic Medical Research 4(2):123-131. |
|
|
Motayo BO, Ogiogwa IJ, Okerentugba PO, Innocent-Adiele HC, Nwanze JC, Onoh CC, Okonko IO (2012). Antimicrobial Resistance Profile of Extra-intestinal Escherichia coli Infections in a South Western Nigerian City. Journal of Microbiology Research 2(5):141-144. |
|
|
Mackenzie FM (2004). Scottish Trends and Routine Diagnostic Detection of ESBL in: Scottish Centre for infection and environmental health (SCIEH) Weekly Report 38(50):1357-4493. |
|
|
Mahon C, Manuselis G, Lehman D (2007). Textbook of Diagnostic Microbiology, 3rd Edition, W B Saunders, Philadephia. |
|
|
Nagdeo NV, Kaore NM, Thombare VR (2012). Phenotypic Methods for detection of various Beta-lactamases in Gram-negative clinical isolates: Need of the hour Journal of Antimicrobial Chemotherapy 3(4):293-297. |
|
|
Nguyen T, Le van P, Le Huy C, Nguyen K (2005). Detection and Characterization of diarrhoeagenic Escherichia coli from young children in Hanoi, Vietnam. Journal of Medical Microbiology 23:755-760. |
|
|
Okeke NL, Laminkanra A, Hartmut S, Kaper JB (2005). Characterization of Escherichia coli strains from cases of childhood diarrhoea in provincial south-Western Nigeria. Journal of Medical Microbiology 55:1163-1163. |
|
|
Olowe OA, Aboderin BW (2010). Detection of Extended Spectrum β-Lactamase Producing Strains of (Escherichia coli) and (Klebsiella sp.) in a Tertiary Health Centre in Ogun State. International Journal of Tropical Medicine 5:62-64. |
|
|
Olusolabomi JI, Onipede OA, Orimolade AE, Akinyoola LA, Babalola GO (2011). Extended-spectrum Beta-lactamase Orthopedic Wound Infections in Nigeria. Journal of Global Infectious Diseases 3(3):211-215. |
|
|
Ochoa JT, Ruiz J, Molina M, Martha DV (2009). High frequency of antimicrobial drug resistance of diarrhoeagenic Escherichia coli in infants in Peru Journal of Medical Microbiology 65:231-237. |
|
|
Pitout JD (2010). Infections with extended-spectrum beta-lactamase-producing Enterobacteriaceae: changing epidemiology and drug treatment choices. Drugs 70:313-333. |
|
|
Pitout JD, Laupland KB (2008). Extended-spectrum beta-lactamase-producing Enterobacteriaceae: an emerging public-health concern. Lancet Infectious Diseases 8:159-166. |
|
|
Rajan S, Prabavathy JV (2012). Antibiotic Sensitivity and Phenotypic Detection of ESBL producing E. coli Strains Causing Urinary Tract Infection In a Community Hospital, Chennai, Tamil Nadu, India Indian Journal of Medical Microbiology 22(3):172 -174. |
|
|
Rono SJ, Kaikai R, Esamai F, Mibei E, Odundo E (2015). Pathotypes and Virulence Markers in Escherichia coli Associated with Diarrhoea among HIV Seropositive and Sero- negative Children below five years in Western Kenya European Scientific Journal 10(27):2341-2350. |
|
|
Saeidi S, Ghamgosha M, Ali TR, Shiri Y, Solouki M, Hassanpour K, Farnoosh G (2014). Phenotypic and genotypic detection of extended-spectrum β-lactamase (ESBL) producing Escherichia coli isolated from urinary tract infections in Zabol, Iran. Journal of Coastal Life Medicine 2(9):732-737. |
|
|
Shahid HI, Abdel Messih IA, Klena JD (2012). Phenotypic and genotypic analysis of enterotoxigenic Escherichia coli in samples obtained from Egyptian children presenting to referral hospitals, Journal of Clinical Microbiology 47:189-197. |
|
|
Shruthi N, Ranvikumar R (2012). Phenotypic detection of virulence factors in Escherichia coli isolated from antenatal cases, catheterized patients and faecal flora, Journal of Clinical and Diagnostic Research 6(10):1699-1703. |
|
|
Umadevi S, Kandhakumari G, Joseph NM, Kumar S, Easow JM, Stephen S, Singh UK (2011). Prevalence and antimicrobial susceptibility pattern of ESBL producing Gram Negative Bacilli, Journal of Clinical and Diagnostic Research 5(2):236-239. |
|
|
Vandepitte J, Verhaegen J, Engbaek K, Rohner P, Piot P, Henck C (2003). Basic Laboratory Procedures in Clinical Bacteriology (2nd ed.). WHO, Geneva. |
|
|
World Health Organization (WHO) (2012). Infectious diseases: The global report, Geneva. pp. 12-17. |
|
|
Wright GD (2016). Antibiotic adjuvants: rescuing antibiotics from resistance. Trends in Microbiology 24:862-871. |
|
|
Yasmin T (2012). Prevalence of ESBL among Esch. coli and Klebsiella spp. in a tertiary care hospital and molecular detection of important ESBL producing genes by multiplex PCR. An M.Sc. Thesis (Unpublished) Department of Microbiology, Mymensingh Medical College, Mymensingh, Bangladesh. |
|
|
Yazdi M, Nazemi A, Mirinargasi M, Jafarpour M, Sharifi SH (2012). Genotypic versus Phenotypic methods to detect Extended-Spectrum Beta-Lactamases (ESBLs) in Uropathogenic Escherichia coli. Annals of Biological Research 3(5):2454-2458. |
|
|
Yusha'u MM, Kumurya AS, Suleiman L (2010). Prevalence of Extended spectrum Beta-lactamases among Enterobacteriaceae in Murtala Mohammed specialist hospital, Kano, Nigeria. Global Journal of Pure and Applied Sciences 3(1):169 - 172. |
|
|
Yusuf I, Haruna M (2013). Detection of AmpC and ESBL Producers among Enterobacteriaceae in a Tertiary Health Care in, Kano - Nigeria. International Journal of Science and Technology 3(4):220-225. |
|
|
Yusha'u M, Aliyu HM, Kumurya AS, Suleiman K (2010). Prevalence of Extended Spectrum Βeta-Lactamases (ESBL) among Enterobacteriaceae in Murtala Mohammed Specialist Hospital, Kano, Nigeria, Bayero Journal of Pure and Applied Sciences 3(1):169 -172. |
|
|
Zasowski EJ, Rybak JM, Rybak MJ (2015). The beta-lactams strike back: ceftazidime-avibactam. The Journal of Human Pharmacology and Drug Therapy 35:755-770. |
|
|
Zhang C, Liu Y, Wang J (2010). Detection of ESBLs and Antimicrobial Susceptibility of Escherichia coli isolated in Henan, China. Journal of Animal and Veterinary Advances 9(15):2030-2034. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


