Full Length Research Paper

ABSTRACT
Medical documentation, in addition to being a legal and research tool, is vital in providing quality patient care. In Nigeria, hand written documentation without proforma, is the norm. We assessed the quality of doctors’ documentation of children admitted into Emergency Paediatrics Unit (EPU), Usmanu Danfodiyo University Teaching Hospital (UDUTH). A 3-month cross-sectional study of admission records by different cadre of doctors for children admitted into the EPU between March and May 2016. A checklist was used to assess the quality of documentation. Data was analysed with SPSS version 22. Of the 191 patients’ clerking studied, 63 (33%) indicated the doctors’ cadre. The patients’ name written on the first page in 168 (88%), but only 31 (16.2%) indicated name on subsequent pages. Date and time of consultation were written in 183 (95.8%) and 61 (31.9%) respectively. Writing was legible in (174) 91.1%, with counter-signing of cancellations in 19 (9.9%). Examination findings documented included blood pressure in 18 (9.4%), pulse rate in 179 (93.7%), respiratory rate in 179 (93.7%) and temperature in 184 (96.3%). This study demonstrates the need for improvement in quality of paediatrics emergency documentation. Continuing medical education (CME) on this is essential.
Key words: Quality, admission, documentation, emergency, paediatrics, Sokoto.
INTRODUCTION
Clinical documentation in a patient’s hospital record includes all information that relates to the care of the patient during their hospital encounter (Raza, 2012). It is designed to evaluate the current status of the patient, assist in developing a plan of care, evaluate the care given, and provide for continuity of care. It is critical that it should be accurate and complete (Twigg et al., 1993). The admission clerking is one of the most Important documents in the patient’s record because it represents the most frequently referenced evidence of a clinical encounter (Twigg et al., 1993, Raza, 2012). Missing data have medical, financial, managerial and medico-legal implications. Ideally no data should be missing and therefore any data missing is significant (Twigg et al., 1993, Raza, 2012).
Omission of important information on admission can lead to incorrect identification, diagnosis, inadequate assessment of risk, and inadequate management (Royal College of Physicians Health Informatics Unit, Towers, 2013).
According to the Royal College of Physicians Health Informatics Unit (RCP, 2011), (Royal College of Physicians Health Informatics Unit) every entry in the medical record should be dated, timed, legible and signed by the person making the entry. The name and designation of the person making the entry should be legibly printed against their signature. Deletions and alterations should be countersigned, dated and timed and every page in the medical record should include the patient’s name, identification number and location in the hospital (Royal College of Physicians Health Informatics Unit).
Data recorded or communicated on admission, handover and discharge should be recorded using a standardised proforma (Royal College of Physicians Health Informatics Unit). Many individual hospitals have guidelines governing admission documentation in form of clerking proformas which may even be electronic in some climes (Towers, 2013). Electronic recording is capital intensive and requires a lot of training and if not properly used will lead to more deficiencies (Callen et al., 2008). Studies on discharge summaries found that electronic discharge summaries were not necessarily of higher quality than handwritten ones (Callen et al., 2008; Unnewehr et al., 2015). In many developing countries including Nigeria, electronic records are not available, therefore, the quality of existing handwritten records has to be improved upon. There is also no study that has assessed quality of medical documentation in Nigeria. This study was therefore carried out to assess the quality of doctors’ documentation of children admitted into Emergency Paediatrics Unit (EPU), UDUTH, Sokoto. This was with a view to utilize audit findings to ensure targeted interventions based on gaps identified.
METHODOLOGY
The study was conducted at the EPU of the Paediatrics Department of UDUTH, located in Sokoto the capital city of Sokoto State, North-western Nigeria. This hospital serves as a major referral centre for the neighbouring Kebbi and Zamfara States amongst others and border countries like Niger and Benin Republics. Being an accredited tertiary training facility, house officers (interns), resident doctors in training and their supervising consultants are available in the department. The EPU is a 25 bedded facility with an average of 6 admissions daily. Patients are admitted via an emergency room with restricted access to ensure doctors concentrate on the critical cases there before they are stabilized and transferred to the main EPU. The emergency room has a writing desk, chairs, unstandardized hospital clerking sheets, laboratory forms and treatment cards provided at all times for documentation purposes. It was a 3-month descriptive and cross-sectional study conducted from between 1st March and 31st May 2016. The different cadre of doctors admitting children into the EPU ranging from house officers, junior and senior residents to consultants was studied. The sample size was determined using an audit target of 90% (Daly, 2004) with a standard formula ((Araoye, 2004).

Where n = minimum sample size, z = Standard normal deviate set at 1.96, p = Prevalence, q = 1 - p = 1 – 0.9, = 0.1, d = degree of accuracy desired = 0.05.
Allowing for non response/ missing data, the sample size to be selected (ns) was: 139/0.9 = 154.
This was rounded up to 200. Therefore, doctors documentations were consecutively recruited till that number was attained. All documentations written for children admitted into the EPU within the study period were included. While documentations for children who demised before full clerking and documentation was completed, from referral notes and from doctors who were aware of the ongoing research were excluded.
A checklist produced by the authors which was based on standard requirements of admission clerking by the Royal College of Physicians Health Informatics Unit was used to evaluate the admission documentation (Royal College of Physicians Health Informatics Unit). Specific information sought included frequency of recording doctors’ identification including time and date documentation, counter-signatures and frequency of recording in patients’ information. Writing was adjudged to be legible if a health information officer (a university graduate) from another unit in the hospital, could read through without encountering much ambiguity (Ridyard et al., 2015). Each morning, the documentations of the previous days’ admissions was collected and reviewed by a member of the research team. By then, another set of doctors would be in the admission room. The review and entering of data was done in another office so as not to pre-empt other doctors about the study thereby leading to bias as they could be more conscious of their documentation. The identity and cadres of doctors who were on call and wrote the documentations were additionally confirmed from the call duty roster and the nurses on duty. Ethical approval was obtained from the Ethics Committee of Usmanu Danfodiyo University Teaching Hospital, Sokoto. Strict confidentiality was maintained with the records. The data was analyzed with SPSS version 22. The categorical variables were expressed as proportions. Chi-square or where necessary, Fisher’s exact test, was used to test for statistical significance. A p-value of < 0.05 was considered statistically significant.
RESULTS
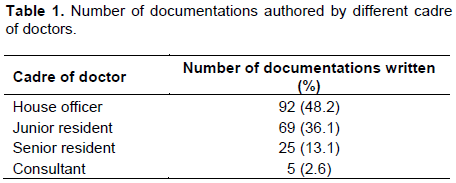
Out of the 200 patients’ clerking assessed, 191 (95.5%) were finally analysed as 9 (4.5%) of them were found to have been entered from unclarified sources/referred patients clerking. All the documentations were handwritten and consisted of more than one page. The clerkings assessed were written by house officers in 92 cases (48.2%), junior residents in 69 cases (36.1%), senior residents in 29 cases (13.1%) and consultants in 5 cases (2.6%). This is shown in Table 1.
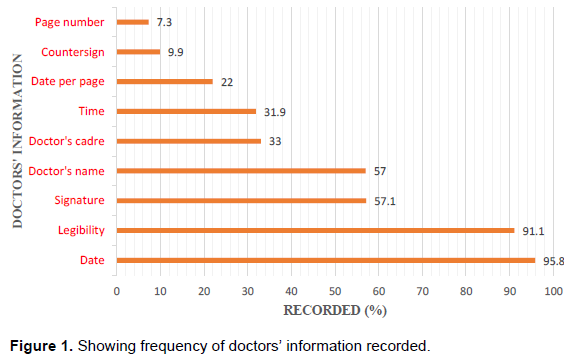
Recording of doctors’ information
Only 108 (57.0%) of the documentations indicated the doctors’ name while 63 (33%) indicated the doctors’ cadre. The clerking was signed by the doctor in 109 cases (57.1%) while counter-signing of corrections, deletions and insertions was done in only 19 cases (9.9%). Date of consultation was written in 183 (95.8%) while the time of consultation was indicated in only 61 (31.9%). However, date or time in the subsequent pages was only indicated in 42 (22%) clerkings. Overall, the writing was adjudged to be legible to the reviewers in (174) 91.1% of the documentations. The details are depicted in Figure 1.
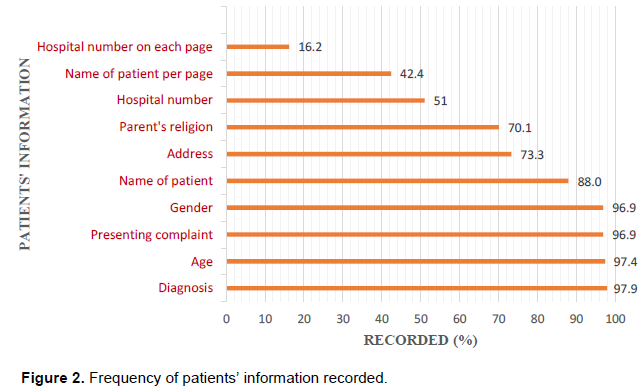
Recording of patients’ information
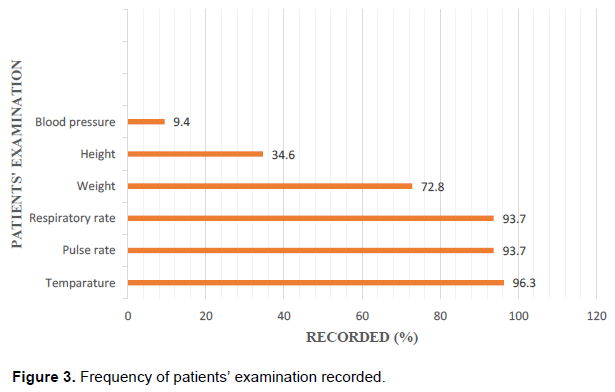
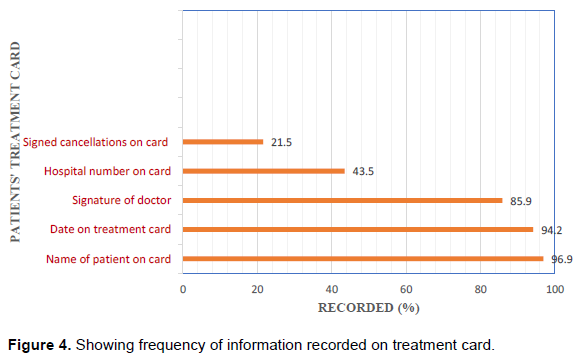
One hundred and sixty-eight (88%) documentations had the patients name written on the first page, but only 81 (42.2%) indicated name on subsequent pages. The hospital number was indicated on the first page in 97 (51%) of cases and on subsequent pages in 31(16.2%). The presenting complaint and diagnosis was written in 185 (96.9%) and (187) 97.9% of clerkings respectively. Review of examination findings showed that the vital signs documented included temperature in 184 (96.3%), pulse rate in 179 (93.7%), respiratory rate in 179 (93.7%) and blood pressure in 18 (9.4%). Anthropometry including weight and height was indicated in 139 (72.8%) and 66 (34.6%) of cases respectively. These details are shown in Figures 2 and 3. On the treatment card, patients name and hospital number were recorded in 96.9% and 43.5% respectively. However, countersigning of cancellations were noted only in 21.5% of those that had corrections as shown in Figure 4.
Relationship of doctors’ cadre to the extent of documentation
Chi square analysis showed that the higher the cadre of the doctor, the more likely that the documentation contained the doctors’ cadre (χ2 = 41.7; p < 0.001), name of doctor (χ2 = 8.7; p = 0.03), time of consultation (χ2 =13.8; p = 0.003) and was legible (χ2 =6.8; p = 0.08), while the lower cadre were more likely to state the informant (χ2 = 12.6; p = 0.006).
DISCUSSION
This study audited the documentation of doctors as they admitted children into a busy emergency paediatric unit. Most other studies on documentation practices have been among adult patients (Chamisa and Zulu, 2007; Attena et al., 2010; Daly, 2008; Ridyard and Street, 2015) with few studies (Pandit, 2014) including the paediatric age group as part of their patient cohort. These studies were also carried out from admission to the point of discharge of patients thereby allowing time for correction of documentation if lapses were noticed. However, this study was carried out shortly after each documentation was completed and could probably reflect a truer picture of the practices of the personnel.
In this study, there was a low rate of proper identification of attending doctors regarding their full name, cadre and signature with figures of 57, 33 and 57.1%, respectively compared to reports by Raza (2012) and Campbell et al. (2017) both from England where rates of documenting these parameters ranged between 82.0 and 99.2%. Daly from Ireland (Daly, 2013) reported low rates of record of doctors’ name and cadre on clerking of 50.0 and 67.0% respectively which could be due to use of hand written records in their centre as practiced in our setting also. These omissions are significant since the names and signature are the only identification available to distinguish the treating physician from others (Raza, 2012). Hence, not documenting such data poses challenges especially if lapses in patient management are later found (Royal College of Physicians Health Informatics Unit).
Documentation in loose sheets even if tagged together in a file is prone to loss, mix-up with other patients’ data and damage. This can be minimised if sheets are properly identified with the patients’ name, hospital number on initial and subsequent pages (Royal College of Physicians Health Informatics Unit). More than 95% of the documentations in our study were dated on the initial pages similar to figures reported by Raza (2012) Daly (2008) and Campbell et al. (2017). However, loosely bound sheets were only dated in 22% of cases. Patient’s name was identified in 88% but was only written in subsequent pages in less than 50%. Other studies reported patient’s name was indicated on the first page in more than 95% (Campbell et al., 2017; Daly and Butler, 2013) and on subsequent pages in 91% (Raza, 2012) and 71% (Royal College of Physicians Health Informatics Unit, Chamisa and Zulu, (2007). The rates of documenting patients name and hospital number which is unique identifiers was lower than the rate of documenting parameters like age and gender. This is possibly because in the study setting, the clerking papers are placed in a file which is already labelled with the patient’s name and hospital number by the records clerk. This notwithstanding, doctors should properly identify patients on their clerking sheets even if bound together (Mann Williams, 2003).
Legibility of documentation in this study was good and comparable to reports by Daly (2008) and Campbell et al. (2017) at > 90% but lower than legibility of 65% reported by Chamisa and Zulu (2007) from South Africa. However, assessment of legibility is subjective compared to the other parameters. Vital sign documentation was better in our study when compared to other studies except for blood pressure which was very low (Campbell et al., 2017; Daly, 2013). Reasons may be due to non-availability of different arm cuff sizes cuff for measurement of blood pressure in children in this study (National High Blood Pressure Education Program et al., 2004). Complaints and diagnosis were better documented compared to the other studies (Royal College of Physicians Health Informatics Unit, Chamisa and Zulu (2007); Daly, 2008) probably because this formed the basis of treatment to be prescribed to the patients.
It was seen that the more senior cadre of doctors were relatively better but not optimal in their documentation. Habit, time restraints, lack of training, and examples being set by others were reasons that were given for poor quality documentation in the study by Raza (2012). However, whatever the reasons, it has been found that audit of clinical notes in different settings, presentation of findings, and redesign of clerking proformas have led to significant increase in quality of documentation.(Campbell et al., 2017; Green and Gauher, 2012; Kentley et al., 2016; Chamisa and Zulu, 2007, Raza, 2012, Towers, 2013)
This study shows that there is need for improvement in admission documentation in the hospital. Further studies are needed to assess the reasons for poor documentation. Designing a clerking proforma preferably electronic adaptable for different specialties and environs is necessary. This should be done in conjunction with the users or trainees, which can be started from medical school, and incorporated in continuing medical education (CME) programmes.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Araoye MO (2004). Sample size calculation. In: Araoye M (Ed): Research Methodology with Statistics for Health and Social Sciences. Nathdex (Publ) Ilorin, pp. 115-121. |
|
|
Attena F, Di Palma MA, Esposito S, Galdo V, Gimigliano A, Parmeggiani C, al e (2010). Original article Quality improvement of medical records in a teaching hospital. Journal of Preventive Medicine and Hygiene 51:53-56. |
|
|
Callen JL, Alderton M, McIntosh J (2008). Evaluation of electronic discharge summaries: a comparison of documentation in electronic and handwritten discharge summaries. International Journal of Medical Informatics 77(9):613-620. |
|
|
Campbell P, Lawrence A, Mahboobani S (2017). Acute Medical Admission Clerking: ticking the boxes but are we missing the point? Watford General Hospital, West Hertfordshire Hospital Trust. |
|
|
Chamisa I, Zulu B (2007). Setting the records straight--a prospective audit of the quality of case notes in a surgical department. South African Journal of Surgery 45(3):92-95. |
|
|
Daly CC, Butler M (2013). Safety Comes First: Are Doctors Attentive Enough to their Initial Clinical Assessment Notes? Irish Medical Journal 106(10):316-318. |
|
|
Daly M (2008). Clinical audit criteria and guidance. Prepared by the Clinical Audit Criteria and Guidance Working group and updated with feedback by Majella Daly. |
|
|
Green E, Gauher S (2012). Improving safety in a District General Coronry care unit- a simple intervention with far reaching consequences. West Middlesex University Hospital NHS Trust. |
|
|
Kentley J, Fox A, Taylor S, Hassan Y, Filipek A (2016).The use of a pro forma to improve quality in clerking vascular surgery patients. British Medical Journal. Quality Improvement Reports; u210642.w4280 |
|
|
Mann R, Williams J (2003). Standards in medical record keeping. Clinical Medicine 3(4):329-332. |
|
|
National High Blood Pressure Education Program, Working Group on High Blood Pressure in Children, Adolescents (2004). The Fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 114:555-576. |
|
|
Pandit U (2014). Study in the Quality of Clinical Documentation Practice in Chitwan Medical College Teaching Hospital, Nepal. Journal of Nepalgunj Medical College 12(2):11-16. |
|
|
Raza M (2012). Good Medical Record Keeping. International Journal of Collaborative Research on Internal Medicine 4(5):535-543. |
|
|
Ridyard E, Street E (2015). Evaluating the Quality of Medical Documentation at a University Teaching Hospital. BMJ Quality Improvement Reports 4(1). |
|
|
Royal College of Physicians Health Informatics Unit Information on the quality of medical note keeping to support appraisal for revalidation. London: RCP, 2011. |
|
|
Towers AL (2013). Clinical Documentation Improvement-A Physician Perspective: Insider Tips for getting Physician Participation in CDI Programs. Journal of AHIMA 84(7):34-41. |
|
|
Twigg J, Briggs T, Parker C, Miller R (1993). Notes: a suitable case for audit. Postgraduate Medical Journal 69:578-580. |
|
|
Unnewehr M, Schaaf B, Marev R, Fitch J, Friederichs H (2015). Optimizing the quality of hospital discharge summaries - a systematic review and practical tools. Postgraduate Medicine 127 (6):630-639. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


