Full Length Research Paper

ABSTRACT
Diabetes mellitus is on the increase worldwide and in Nigeria, with prevalence ranging from 0.65% in rural Mangu to as high as 11.0% in urban Lagos. Its prevention, early diagnosis and adequate treatment to prevent morbidity and mortality are essential. Glycated haemoglobin estimation is a marker of glycaemic control and it reflects average plasma glucose over previous eight to twelve weeks. Reporting estimated average glucose along with glycated haemoglobin values may be useful in the assessment of long term glycaemic control of diabetic patients. This work aims to assess glycaemic control in diabetic patients and determine the association between estimated average glucose and glycated haemoglobin values. This work is a retrospective study. Data of 100 diabetic patients (Type 1 and 2) seen in the endocrine outpatient clinic of the University of Benin Teaching Hospital between March 2017 and October 2017 were analyzed. Glycated haemoglobin (HbA1c) assay was done using high performance liquid chromatography (Bio - Rad). Estimated average glucose was derived using Nathan’s regression formula. Good glycaemic control was established at glycated haemoglobin < 7% according to the American Diabetes Association recommendation. Mean age of the subjects was 61.5 ± 14.8 years. Mean fasting plasma glucose, estimated average glucose, glycated haemoglobin in the subjects were 188.6 ± 100.3, 165.4 ± 24.8 mg/dl, 7.4 ± 2.4% respectively. Estimated average glucose showed a strong positive correlation with glycated haemoglobin, which was statistically significant; r = 1.000, p = 0.000. 46% of the subjects had glycated haemoglobin values < 7%, while 54% had values ≥ 7%. Estimated average glucose correlated strongly and significantly with glycated haemoglobin, therefore reporting estimated average glucose along with glycated haemoglobin values may be useful and beneficial in the assessment of long term glycaemic control of diabetic patients. Glycaemic control is yet to be optimal in the study population.
Key words: Estimated average blood glucose (eAG), glycated haemoglobin (HbA1c), diabetes mellitus.
INTRODUCTION
Diabetes mellitus is a chronic disease, with an increasing prevalence worldwide, Nigeria inclusive (Nyenwe et al., 2003). Prevalence in Nigeria has been reported to range from 0.85% in rural Mangu village, to as high as 11% in urban Lagos (Akinkugbe, 1967). The WHO suggested that Nigeria has the greatest number of people living with diabetes in Africa, with an estimated burden of about 1.7 million, which will increase to 4.6 million by 2030 (Chineye et al., 2012). Diabetes Mellitus leads to both microvascular and macrovascular complications, which include cardiovascular and renal complications if not treated early. Prevention of the disease is of utmost importance. Early diagnosis and treatment, maintaining good glycaemic control helps to reduce co-morbidity and mortality. Glycated haemoglobin is not only a diagnostic tool for diabetes mellitus; it is also a measure of glycaemic control over the past 2-3 months in an individual (Sacks, 2007). In patients with diabetes mellitus, glycated haemoglobin value is used to determine the degree of glycaemic control and make decisions regarding therapy. In addition the concentration of glycated haemoglobin predicts the progression of diabetic microvascular complication (Sacks, 2007; UK Prospective diabetes study (UK PDS, 1998). More recent evidence indicates that glycated haemoglobin also predicts cardiovascular disease in patients with Type 1 diabetes (Sacks, 2007; American Diabetes Association, 2007). Measurement of glycated haemoglobin is thus an important component in the management of patients with diabetes (American Diabetes Association, 2016). The American Diabetes association recommends that HbAIc should be measured at least twice a year (American Diabetes Association, 2018) and Good glycemic control is reported at HbAIc at <7% (American Diabetes Association, 2018).
The relationship between glycated haemoglobin (HbA1c) and Estimated Average glucose (eAG) is described by the formula; eAG - 28.7 × AlC - 46.7 (Cha and Ko, 2016; Raja et al., 2003), which is Nathan’s regression equation recommended by the American Diabetes Association (Raja et al., 2003).
Cha and Ko (2016) have said translating the A1c value into an estimated average glucose (eAG) is more practical and much easier for patients to understand. Riyadh and Abdullah, (2018) and Zhou et al. (2013) have reported glycaemic control findings in their area of study. The need to assess glycaemic control and determine the correlation between glyceated hemoglobin and estimated average glucose has become important due to the increasing prevalence of diabetes milletus in Nigeria.
MATERIALS AND METHODS
Data of l00 diabetic patients (38 males and 62 females) seen consecutively in the endocrinology outpatient clinic between March 2017 and October 2017 were analyzed. They were patients already diagnosed with diabetes mellitus according to WHO criteria and were on blood glucose lowering drugs. Relevant data of both Type 1 and 2 Diabetic patients whose blood samples were sent for glycated haemoglobin assay, were retrospectively analyzed. Other demographic data such as age, gender and biochemical investigations of the patients were retrieved and analyzed. Hospital ethical committee protocol was observed. Glycated haemoglobin (HbA1c) assay was done using high performance liquid chromatography. (D10 – Bio Rad). Estimated average glucose was calculated using Nathan’s regression formula;
eAG = 28.7 × HbAlC – 46.7
Statistical analysis
This was done using Statistical Package of Social Sciences (SPSS) version 21. Difference between means of variables was determined using the student “t” rest. Correlation between variables was examined using Pearson’s correlation. Level of significance was set at P≤ 0.05.
RESULTS
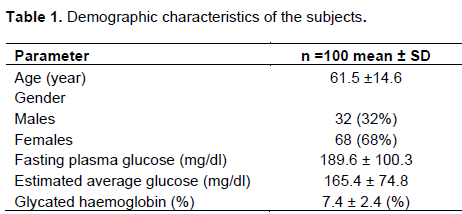
Data of a total of 100 diabetic subjects (38 males, 62 females) were analyzed. Mean age of the subjects was 61.5 ± 14.8 years (Table 1). Mean fasting plasma glucose, estimated average glucose (eAG) and glycated haemoglobin in the diabetic subjects were 189.6 ± 100.3, 165.4 ± 74.8 mg/dl, 7.4 ±2.4% respectively (Table 1). Mean fasting plasma glucose, estimated average glucose and glycated haemogobin were 183.6 ± 93.0. 158.1±85.3 mg/dl, 7.3 ± 2.8%, respectively in the male subjects and 196.1 ± 112.0, 169.9 ± 68.3 mg/dl, 7.5 ±2.2% in the females (Table 2). Difference was not statistically significant (P > 0.05). Estimated average glucose showed a strong positive correlation with glycated haemoglobin r =1.000 P = 0.000. (Table 3 and Figure 1). 46% of the subjects had glycated haemogobin <7% while 39% had levels between ≥ 7 and 10%; 15% had levels > 10% (Table 4).




DISCUSSION
With the increasing prevalence of diabetes mellitus, the social and economic burden on the nation is rising. Adequate prevention strategies and early diagnosis, intervention and treatment to ensure good glycaemic control are of utmost importance. Mean age of the subjects in the study was similar to that reported by Shittu et al. (2017). There were more females in this study than males. Similar findings were reported by Shittu et al. (2017) in their study in Oke Osun Region of Oyo State, Nigeria and the Nigerian National Communicable (The Expert Committee on Non-communicable Disease (1997) diseases. Other studies (Elmandi et al., 1991) also made similar observations. The combined effect of more elderly women than men in most populations is the most likely reason for this observation (Shittu et al., 2017). However, some authors have reported male preponderance (Amooh et al. (2002).
Mean fasting plasma glucose, glycated haemoglobin levels were elevated in both the male and female subjects. Though, there were no statistically significant differences between the values in the male and female subjects. Estimated average glucose showed a positive correlation value of 1 with Glycated haemoglobin in our study. Several authors have reported similar findings. Nepal et al.17 reported a strong correlation value of 1, which was statistically significant, in their study, and concluded that “blood glucose expressed as eAG improves the understanding of blood glucose monitoring”. Nathan 18 et al. recorded a correlation value of 0.8, which was statistically significant and concluded that glycated haemoglobin levels can be expressed as estimated average blood glucose for most patients with type 1 and type 2 diabetes. Sacks (2007) and American Diabetes Association (2016) also reported linear correlation of estimated average glucose and glycated haemoglobin. From these findings, reporting Glycated haemoglobin values along with estimated average glucose levels, will definitely be beneficial in the management of Diabetes Mellitus patients as it plays a dual role of giving the physician a quick overview of average blood glucose over the preceding 2 to 3 months and helps to determine the type of pharmacotherapy and necessary adjustments where applicable. Also, it is an easier and simpler interpretation to the patient on how his/her blood glucose has been controlled over the past 2-3 months. This may also boost compliance, especially if the estimated average blood glucose is still yet to be within the normal range, the patient knows he/she would have to take his/her medications. From the finding in our study, reporting estimated average glucose along with glycated haemoglobin may be beneficial in monitoring and assessment of long term glycaemic control in diabetics in our area of study. The American Diabetes Association and the American Association of Clinical Chemist have determined that the correlation (r=0.92) in the ADAG trial is strong enough to justify reporting both the A1c results and the estimated average glucose result when a clinician orders the A1c test10. However, fasting plasma glucose estimation is still the tool for short term monitoring of glycaemic control and is a relevant part of diabetic management protocol. Reporting the three values together gives a holistic picture of both the past and present glycaemic status of the patient.
There are different schools of thoughts on good glycaemic control. While the American Diabetes Association recommends good glycemic control to be HbA1c > 7%, International Diabetes Federation and American College of Endocrinology recommends values < 6.5% as good glycaemic control. HbA1c < 7% was considered as good glycaemic control in our study. Only 46% of the subjects in this study had glycated haemoglobin < 7 and 54% had glycated haemoglobin values ≥7%, with 15% showing poor glycemic control having values > 10%. Idogun and Olumese recorded 46.8% with poor glycaemic control in 2007, Unadike et al. (2010) reported 46% in 2010, Edo E (Edo and Akhiemokhan, 2012) reported 63% with poor glycaemic control in 2012, also in a previous study by Adewolu, (2014), 59.5% had poor glycaemic control, all in the same area of study. Adebisi et al. (2009) and John et al. (2005) in Nigeria have also reported high prevalence of poor glycaemic control. Achieving good glycaemic control of diabetic patients is still a challenge. Factors ranging from non-compliance to pharmacotherapy, lack of funds to purchase required medications and investigations, payment of hospital bills, socio-cultural beliefs may all be contributory to this development. Economic reasons may take a larger percentage of these factors because of the prevailing high cost of living. Measures such as good patient education, drug subsidization, expansion of scope of health insurance schemes to include diabetes care may be helpful.
In this study, estimated average glucose correlated strongly and significantly with glycated haemoglobin in the diabetic subjects, therefore reporting estimated average glucose along with average haemoglobin will be useful and beneficial in monitoring of long term glycaemic control. 54% of the subjects had poor glycaemic control.
CONCLUSION
Reporting estimated average glucose (eAG) along with glycated haemoglobin may be useful and beneficial in the assessment and monitoring of long term glycaemic control in diabetic patients. Glycaemic control is yet to be optimal in the study population . Socio-economic measures and expanded health insurance coverage may be useful in optimizing glycaemic control.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adebisi SA, Oghagbon EK, Akande TM, Olarionye JK (2009). Glycated haemoglobin and glycaemic of diabetes in Ilorin. Nigerian Journal of Clinical Practice 12:87-91. |
|
|
Adewolu OF (2014) Glycaemic control in patients with Type 2 diabetes mellitus in a secondary school and tertiary health center in Oredo and Egor Local Government areas in Benin city, South-South Nigeria |
|
|
Akinkugbe OO (1967). Final report of National survey on communicable diseases in Nigeria series 1.Federal Ministry of Health & Social services, Lagos. |
|
|
American Diabetes Association (2016). Glycaemic targets. Diabetes care 39 suppl S39-S46. |
|
|
American Diabetes Association (2018). Glycaemic targets: Standards of medical care in Diabetes. Diabetes care 2018 Jan 41(suppl1):S55-S64. |
|
|
American Diabetes Association (2007) . Standard of medical care in diabetes. Diabetes care 30 (suppl 1) S4-S41. |
|
|
Amooh AG, Owusu SK, Adjei S (2002). Diabetes in Ghana: A community based prevalence study in Greater Accra. Diabetes Research and Clinical Practice 56:88-95. |
|
|
Cha SA, Ko SH (2016). Association between estimated blood glucose levels and glycated haemoglobin levels. Korean Journal of Internal Medicine 31(3):457-460. |
|
|
Chineye S, Uloko AE, Ogbera AO, Ofoegbu EN, Fasanmade OA, Fasanmade AA, Osi OO (2012). Profile of Nigerians with diabetes mellitus-Diabcare Nigeria study group (2008): Results of a multicenter study. Indian Journal of Endocrinology and Metabolism 16(4):558. |
|
|
Edo AE, Akhiemokhan K (2012). Relationships between AIC and Spot glucose measurements in Nigerians with type 2 diabetes mellitus. Nigerian Journal of Clinical Practice 15:23-26. |
|
|
Elmandi EM, Kaballo AM, Muktar EA (1991). Features of non-insulin dependent diabetes mellitus (NIDIM) in Sudan. Diabetes Research and Clinical Practice 11:59-63. |
|
|
Idogun ES, Olumese FE (2007). Prevalence of poor Glycaemic control in diabetics seen in a tertiary medical center. Nigerian Postgraduate Medical Journal 14 (1):34-6. |
|
|
John ME, Effiong MU, Essien OE (2005). Compliance and glycaemic control in adult diabetic patients in rural Nigeria. Diabetes Int. 13:17-20. |
|
|
Mahato RM, Nepal KA, Gelal B, Regmi P (2012). Association of estimated average glucose (EAG) with fasting, post prandial serum glucose levels. Journal of Nepal Association for Medical Laboratory Sciences 11(1). |
|
|
Nathan DM, Kuenen J, Borg R, Zeng H (2008). Translating the A/C assay into estimated Average Glucose values. Diabetes care 31: 1473-1478. |
|
|
Nyenwe EA, Ordia OJ, Ihekwahe A, Babtunde S (2003). Type 2 Diabetes in Adult Nigerians: A study of its prevalence and risks factors in Port Harcourt Nigeria. Diabetes Research and Clinical Practice. 62(3):177-189. |
|
|
Raja RP, Reetesh RP, Mhesh V (2003). The association between estimated average glucose levels and fasting plasma glucose levels in a tertiary care centre. |
|
|
Rasaki OS, Fakorede OK, Sikiru AB, Louis OO, Abdullateef GS, Yusuf M (2017). Prevalence of diabetes and prediabates in oke-ogun region of oyo state, Nigeria. Cogent Medicine 4(1):1326211. |
|
|
Riyadh AA, Abdullah HA (2018). The prevalence and determinants of poor glycaemic control among adults with type 2 diabetes mellitus in Saudi Arabia. Diabetes, metalbolic syndrome and obesity: Targets and therapy 11:15-21. |
|
|
Sacks DB (2007). Correlation between haemoglobin ALc (HbA1c) and average blood glucose Can HbAlc be reported as estimated blood glucose concentration. Journal of Diabetes Science and Technology 1(6):801-803. |
|
|
UK Prospective diabetes study (UK PDS) (1998). Group intensive blood glucose control in diabetics with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes. (UKPDS 33) Lancet 3:837-852. |
|
|
Unadike BC, Eresie A, Ohwovoriole AE (2010). Glycaemic control amongst persons with Diabetes mellitus in Benin City. Nigerian Medical Journal 51:164-166. |
|
|
Zhou J, Mo Y, Li H, Ran X, Yang W, Li Q, Peng Y, Li Y, Gao X, Luan X, Wang W, Xie Y, Jia W (2013). Relationship between HbA1c and Continous Glucose Monitoring in Chinese Population: A Multicenter Study. PLoS ONE 8(12):e83827. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


