Full Length Research Paper

ABSTRACT
Hepatitis sero-positivity at initiation of haemodialysis may suggest a causal role or arise due to repeated blood transfusions and reduced immunity associated with advanced chronic kidney disease. This study was to determine the sero-prevalence of Hepatitis B and C infection at initiation of haemodialysis, and describe the clinical characteristics and outcome of patients. This is a cross-sectional study of all end stage renal disease (ESRD) patients who had haemodialysis from January 2012 to January 2016 in the study centre. Patients with HIV infection were excluded. Data on the demographic characteristics, health status, aetiology of renal disease, clinical and biochemical parameters were collected. Fifteen (4.9%) out of 341 patients were hepatitis sero-positive; 2.6% were hepatitis B seropositive, while 2.3% were hepatitis C positive. Majority (86.6%) of the patients were males. Hepatitis infection was significantly commoner among patients with sickle cell disease (2 out of 6, p=0.005). Median duration on haemodialysis was 1 month (IQR 0.6, 1.0), while mortality was 20%. Hepatitis B and C infection is commoner among male ESRD patients, the young/middle-aged, and patients with sickle cell disease. Majority of patients are unaware of their hepatitis status and are treatment naive. Haemodialysis treatment drop-out rate and mortality are high.
Key words: Hepatitis, end stage renal disease, haemodialysis, sickle cell disease.
INTRODUCTION
Hepatitis B and C viral infections contribute to the aetiology of chronic kidney disease in many developing countries. The prevalence of hepatitis infection is particularly higher among chronic kidney disease and haemodialysis patient population compared to the general population due to frequent use of blood products, poor infection control practices in haemodialysis centre, lack of effective vaccination, and reduced immunity (Edey et al., 2010).
Hepatitis B infection is more common than HCV infection globally. According to the World Health Organization, in 2015, 257 million people were living with Hepatitis B infection, compared to 71 million living with HCV (World Health Organization, 2017). Africa and West Pacific regions have the highest prevalence of 6.1 and 6.2% respectively for HBV, while prevalence of HCV in Africa is 1% compared to 2.3% in Eastern Mediterranean region (World Health Organization, 2017). Prevalence in haemodialysis patients ranges from 2.6-70% depending mostly on the population studied and the infection control practices in individual haemodialysis units (Luma et al., (2017); Garima et al., 2013; Rinonce et al., 2013. The prevalence of HBV in dialysis centres in Europe, USA and Japan ranges from 0.6-6% (Burdick et al., 2003; Bernieh, 2015), while HCV is generally below 5% in high-income countries (Fabrizi, 2013).
Amira and Lesi (2017) in Nigeria reported a higher prevalence of HBV compared to HCV infection (6.0 vs. 1.2%) among haemodialysis population. Conversely, in Cameroon, the prevalence of HBV and HCV at commencement of haemodialysis was 6.2 and 20.6%, respectively (Halle et al., 2016). A recent study in same country reported a prevalence of 9.3 and 19.2% for HBV and HCV respectively (Luma et al., (2017); suggesting that the HBV prevalence rates in haemodialysis patients mirror that in the general population (8-12%), while HCV infection is much higher in the haemodialysis population. The prevalence rates of hepatitis B infections are said to be decreasing among haemodialysis patients in some countries, due to vaccination, improved infection control, particularly the isolation of sero-positive patients during haemodalysis (Fabrizi et al., 2002). Both HBV and HCV infections are important causes of chronic glomerulonephritis, which is one of the leading causes of chronic kidney disease (CKD) in Sub-Saharan Africa (Ayodele et al., 2006; Bhimma et al., 1998). HBV and HCV are associated with membranous glomerulonephritis (GN), membranoproliferative GN and cryoglobulinaemia. Unfortunately, due to late presentation of patients and poorly equipped laboratories in many developing countries, confirmatory histological diagnosis of hepatitis induced GN is often not made. Diagnosis is often only by suspicion, based on sero-positivity of the patient and clinical, urine examination findings. Treatment of HBV and HCV infection in the general population is low in many African countries due to lack of awareness and high costs of treatment (World Health Organization, 2017). This may explain the high prevalence of these infections as well as its complications, including renal disease and liver cirrhosis in middle and low-income countries.
The aim of this study is to determine the sero-prevalence of Hepatitis B and C infection at initiation of haemodialysis in patients with ESRD, and to describe the clinical characteristics and outcomes of the patients.
MATERIALS AND METHODS
This is a cross-sectional study carried out in Delta State University Teaching Hospital in Southern Nigeria. The centre is equipped with 8 haemodialysis machines, out of which three are set aside for HBV, HCV and HIV sero-positive patients. All patients are routinely screened for these 3 viral infections at presentation and repeated at least every 6 months. Records of all patients who had haemodialysis treatment in the centre from Jan. 2012-Jan. 2016 were obtained from and the dialysis register, including patients who might have had prior haemodialysis in other centres. Patients with acute kidney injury, incomplete or incorrect data were excluded. Ethical clearance was obtained from the Institution’s health research and ethics committee.
Demographic data, health status of patient, aetiology of renal disease, some clinical and biochemical parameters such as systolic and diastolic blood pressures, packed cell volume, were obtained from patients’ dialysis records (Table 1). Hepatitis B surface Antigen and HCV antibodies were detected using the Fisher-Tec rapid kit. Hepatitis B infection was regarded as the presence of HBSAg in serum, while HCV was diagnosed when anti-HCV was present in serum. Data was analyzed using IBM statistical package for social sciences (SPSS) Statistics for windows version 22.0 (IBM Corps., Armonk, N.Y. USA). The main analysis was the determination of the seroprevalence of HBV and HCV infection for the sample. The clinical characteristics of seropositive patients were presented using descriptive statistics and proportions.

RESULTS
Three hundred and forty-one ESRD patients initiated haemodialysis during the 5 year period, 4.9% (n=15) were Hepatitis seropositive. Specific prevalence for HBV and HCV was 2.6 and 2.3% respectively; no patient was sero-positive for both viruses. Thirteen patients (86.6%) were unaware of their hepatitis status prior to presentation. Majority (n=12) of the seropositive patients were males compared to the sero-negative population (80% vs. 40.5%, p=0.126), sex ratio was 4:1. The mean age was 40 ± 16 years compared to 50±16 years among the Hepatitis negative patients (p=0.018), and 93% of sero-positive patients were £60 years compared to 69.6% in the sero-negative population.
The commonest clinical features were weakness (n=13), pallor (n=10), leg swelling (n=9), proteinuria (n=8), nausea and vomiting (n=7) (Table 2). Gastrointestinal bleeding was seen in 3 out of the 15 patients. Mean PCV was 22 ± 4% (Table 3). The commonest causes of ESRD were suspected CGN (40%), Hypertension (20%), Diabetes mellitus (20%), and sickle cell disease (13.3%) (Table 3). A significantly higher proportion of hepatitis seropositive patients had sickle cell disease (13.3%) compared to sero-negative patients (1.2%). Similarly, 40% of sero-positive patients had a diagnosis of CGN, compared to 25% among the sero-negative patients. This was however not statistically significant (OR=1.4, 95%CI=0.49, 4.48). Eight out of the 15 sero-positive patients had previous blood transfusions before presentation. The mode of transmission was not known for the others; however one patient had 3 other first-degree relative who were seropositive for Hepatitis B.


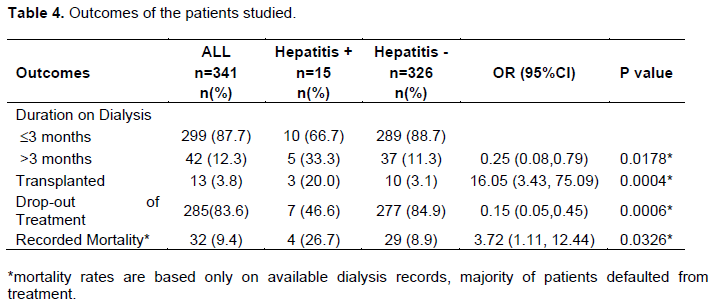
None of the patients had renal biopsy due to late presentation with shrunken kidneys. None of the patients reported taking anti-hepatitis viral medications at diagnosis of ESRD. Median duration on haemodialysis was 1 month (IQR 0.6, 1.0). Significantly higher proportion of hepatitis sero-positive compared to sero-negative patients dialysed for >3months (33.3% vs. 11.3% p=0.0178), and received kidney transplant (20% vs. 3.1%, p=0.0004).
Mortality was higher among the hepatitits sero-positive patients compared to sero-negative patients (26 and 8.9% respectively, OR=3.72 95%CI= 1.11, 12.44) (Table 4).
DISCUSSION
The overall prevalence of Hepatitis infection among haemodialysis patients in this study (4.9%) is comparable with reports from western countries and some parts of Nigeria (Amira and Lesi, 2017), but is lower when compared with reports from Cameroon, Middle East and India. A systematic review by Musa et al. (2015), in Nigeria reported a pooled prevalence rate of 13.6%. The prevalence rates of hepatitis B in the general Nigerian population range from 0.5- 46.8% depending on the population studied and the testing method used. The low rates seen among dialysis patients in this study may be due to the use of a rapid test kit that is not sensitive in the window period and may lead to false negatives. Improved infection control, vaccination, and isolation of Hepatitis infected patients during haemodialysis are other factors contributing to the low rates observed. The World Health Organisation reports that although there are increased deaths from hepatitis B infection, there is a decline in the number of new cases due to improved immunization coverage in children (World Health Organization, 2017). This is not the case for Hepatitis C, as there remains an increasing incidence of infection in some regions. Prevalence of Hepatitis infections in the general population is affected by variations in socio-cultural and religious practices, level of education and immunisation coverage. In CKD patients reduced immunity, repeated exposure to blood products and the haemodialysis procedure are additional risks.
Majority of sero-positive patients in this study were unaware of their status and none was on treatment. The implication of this is that the public is yet to embrace voluntary screening. Many patients are only diagnosed, during hospitalisation or investigation for related or unrelated diseases. The World Health Organisation reports that just 9% of all HBV infections and 20% of all HCV infections were diagnosed in 2015, while 8% of those diagnosed with HBV infection (1.7 million people) were on treatment, and only 7% of those diagnosed with HCV infection (1.1 million people) had started curative treatment during that year (World Health Organization, 2017).
Male predominance among the seropositive patients reflects the gender distribution among the ESRD population as well as in the general population. It may seem that ESRD is commoner among males, or a confirmation that males have better access to health care in many developing countries, particularly in Sub-Saharan Africa. The younger age of infected patients also reflects the distribution of hepatitis infection in the general population, and other authors similarly found that seropositive haemodialysis patients were younger compared to those who are seronegative (Alashek et al., 2012; Daw et al., 2002). Some contributory factors may include risky social behaviour among the young compared to older people, and vertical transmission. Furthermore, CGN, which has been reported as the commonest CKD in seropositive patients, is also a diagnosis more prevalent in the young compared to Diabetes mellitus, and hypertension (Amira and Lesi, 2017). Conversely, Burdick et al. (2003) and Bahri et al. (2016) have also reported that HBV and HCV infection is commoner in older compared to younger haemodialysis patients. The reason ascribed to this pattern was reduced immunity in the older age group (Bahri et al., 2016); although this is scientifically plausible, it wrongly suggests that the patients acquired the infection at older ages.
Majority of the seropositive patients had received prior blood transfusions either as a result of CKD or other comorbidities such as sickle cell disease, suggesting that this may be the source of infection. However vertical transmission and horizontal transmission from sexual relations and other unsafe practices cannot be excluded.
In this study, up to 40% of seropositive patients had a clinical diagnosis of suspected GN. Amira and Lesi (2017) in Lagos similarly reported a higher proportion of patients with CGN testing positive to Hepatitis B, compared to those with other diagnosis. Another study by Akinsola et al., (1984) found 33% of the patients with GN were HBsAg positive compared with 6% in controls. However, like this current study, these were all cross-sectional studies and can only suggest that the viral infections play a causal role in the development of CKD. Although histological diagnosis is essential in patients with suspected Hepatitis related GN, in this study diagnosis was based on clinical criteria alone, mainly due to late presentation evidenced by shrunken kidneys on imaging and/or severe azotaemia. However, proteinuria was found in about 53% of the patients studied, suggesting the presence of glomerular disease. A meta-analysis published in 2015 showed that chronic HCV infection is associated with a 51 and 43% increase in the risk of proteinuria and the incidence of CKD respectively (Fabrizi et al., 2015). A significantly higher proportion of patients with SCD were seropositive compared to patients without SCD. Prevalence of HBV and HCV is particularly high in patients with SCD, due to the repeated exposure to blood and blood products, and other studies corroborate this (Lesi and Kehinde, 2003; Suliman et al., 2013; Jibrin et al., 2014).
This study revealed that the median duration on haemodialysis was 1 month. The average time on dialysis in most of Nigeria is 3 months (Ulasi and Ijoma, 2010), and this is mostly because of financial constraints, mortality, and retraction of consent. Surprisingly, a significantly higher proportion of sero-positive than sero-negative patient dialysed for more than 3 months and had kidney transplant. Longer time on dialysis is notably associated with HCV infection in CKD patients (Assarehzadegan et al., 2009). Some of the seropositive patients had prior haemodialysis in other centres before referral to the study centre suggesting that they might have had longer duration on haemodialysis. Furthermore, a longer time on haemodialysis usually reflects availability of financial resources and patient motivation; this may also explain why a higher proportion of these patients had kidney transplant. Availability of financial resources among the sero-positive patients may be a chance of finding; however it is possible that because of the smaller number of these patients compared to the sero-negative patients, there is more effective doctor/nurse: patient relationship and counselling
Finally, the higher mortality rates in seropositive haemodialysis patients is not surprising, given the added morbidity associated with HBV and HCV infection; in addition none of these patients were on anti-viral treatment prior to CKD diagnosis. Although much progress has been made globally regarding hepatitis treatment in general and in CKD population (Jadoul and Martin, 2017), treatment rates remain low in developing countries (World Health Organization, 2017) possibly due to unawareness/poor patient education, physician inertia, scarce funds, and the overwhelming care burden of ESRD on the patient and family.
This study was a cross-sectional study based on previously recorded data and so some relevant variables were missing. The hepatitis screening method used in this study is not a confirmatory test and can misdiagnose cases (false positives and negatives). Although we studied patients initiating haemodialysis at our centre, some patients who had received haemodialysis treatment in other centre(s) prior to referral were not excluded. Sample size of sero-positive patients was small and limits the power and generalisabilty of study. Sampling was by convenience, as all available records of patients dialysed in the centre were used.
CONCLUSION
Hepatitis B and C infection is commoner among male ESRD patients, the young/middle-aged, and patients with sickle cell disease. Majority of patients are unaware of their hepatitis status and treatment-naive. Haemodialysis treatment drop-out rate and mortality is high. Re-enforcement of public health education on immunization, voluntary screening, and safe health practices will promote prevention and reduce morbidity and mortality associated with advanced hepatitis infection.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Akinsola A, Olusanya O, Iyun AO, Mbanefo CO (1984). Role of hepatitis Bs antigen in chronic glomerulonephritides in Nigerians. Africa Journal of Medicine and Medical Science 13:33‑39. |
|
|
Alashek WA, McIntyre CW, Taal MW (2012). Hepatitis B and C infection in haemodialysis patients in Libya: prevalence, incidence and risk factors. BMC Infect Disease 12:265. |
|
|
Amira CO, Lesi OA (2017). Seroprevalence of hepatitis B and C infection among Nigerian subjects with chronic kidney disease. Journal Clinical Science 14:58-61. |
|
|
Assarehzadegan MA, Shakerinejad G, Noroozkohnejad R, Amini A, Rahim Rezaee SA (2009). Prevalence of hepatitis C and B infection and HCV genotypes among hemodialysis patients in Khuzestan province, southwest Iran. Saudi Journal of Kidney Disease and Transplanting 20:681-684. |
|
|
Ayodele OE, Salako BL, Kadiri S, Arije A, Alebiosu CO (2006). Hepatitis B virus infection: Implications in chronic kidney disease, dialysis and transplantation. Africa Journal of Medicine Medical Science 35:111‑119. |
|
|
Bahri F, Kheirabad AK, Ghasemzadeh I, Shoja S, Gouklani H (2016). Hepatitis Viruses B and D and Human Immunodeficiency Virus Infections in Hemodialysis Patients in the South of Iran: Prevalence and Genotypes. Hepatology Mon. 16(1):e32971 |
|
|
Bernieh B (2015). Viral hepatitis in hemodialysis: an update. Journal of Translational Internal Medicine 3(3):93-105. |
|
|
Bhimma R, Coovadia HM, Adhilari M (1998). Hepatitis B virus‑associated nephropathy membranous nephropathy in black South African children. Pediatrician Nephrology 11:429‑34. |
|
|
Burdick RA, Bragg-Gresham JL, Woods JD, Hedderwick SA, Kurokawa K, Combe C, Saito A, LaBrecque J, Port FK, Young EW (2003). Patterns of hepatitis B prevalence and seroconversion in hemodialysis units from three continents: the DOPPS. Kidney International 63(6):2222-2229. |
|
|
Daw MA, Elkaber MA, Drah AM, Werfalli MM, Mihat AA, Siala IM (2002). Prevalence of hepatitis C virus antibodies among different populations of relative and attributable risk. Saudi Medical Journal 23(11):1356-1360. |
|
|
Edey M, Barraclough K, Johnson DW (2010). Review article: Hepatitis B and dialysis. Nephrology (Carlton) 15:137-45. |
|
|
Fabrizi F, Poordad F, Martin P (2002). Hepatitis C. Infection and the patients with end-stage renal disease. Hepatology 36(1):3-10. |
|
|
Fabrizi F, Verdesca S, Messa P, Martin P (2015). Hepatitis C virus infection increases the risk of developing chronic kidney disease: a systematic review and meta-analysis. Dig Disease Science 60(12):3801-3813. |
|
|
Fabrizi F (2013). Hepatitis C virus infection and dialysis: 2012 update. ISRN nephrology 159760. |
|
|
Garima M, Gupta P, Thakuriaz B, Mukhiyax GK, Mittaly M (2013). Profile of Hepatitis B Virus, Hepatitis C Virus, Hepatitis D Virus and Human Immunodeficiency Virus Infections in Hemodialysis Patients of a Tertiary Care Hospital in Uttarakhand. Journal Clinical Experimental Hepatology 3:24-28 |
|
|
Halle MP, Choukem SP, Kaze FF, Ashuntantang G, Tchamago V (2016). Hepatitis B, Hepatitis C and Human immune deficiency virus seroconversion positivity rates and their potential risk factors among patients on maintenance hemodialysis in Cameroon. Iranian Journal of Kidney Diseases 10(5):304-309. |
|
|
Jadoul M, Martin P (2017). Hepatitis C Treatment in Chronic Kidney Disease Patients: The Kidney Disease Improving Global Outcomes Perspective. Blood Purification 43:206-209. |
|
|
Jibrin B, Jiya NM, Ahmed H (2014). Seroprevalence of hepatitis C virus antibody and its associated risk factors in children with sickle cell anaemia. Sub-Saharan Africa Journal of Medicine 1:20-25. |
|
|
Lesi OA, Kehinde MO (2003). Hepatitis C virus infection in patients with sickle cell anaemia at the Lagos University Hospital. Niger Postgraduate Medical Journal 10:79‑83. |
|
|
Luma HN, Halle MP, Eloumou SAF, Azingala F, Kamdem F, Donfack-Sontsa O, Ashuntantang G (2017). Seroprevalence of human immunodeficiency virus, hepatitis B and C viruses among haemodialysis patients in two newly opened centres in Cameroon. |
|
|
Musa B, Bussell S, Borodo MM, Samaila AA, Femi OL (2015). Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: A systematic review and meta-analysis. Niger Journal Clinical Practice 18:163-167. |
|
|
Rinonce HT, Yano Y, Utsumi T, Heriyanto DS, Anggorowati N, Widasari DI (2013). Hepatitis B and C virus infection among hemodialysis patients in Yogyakarta, Indonesia: Prevalence and molecular evidence for nosocomial transmission. Journal of Medicine and Virology 85:1348‑61. |
|
|
Suliman AM, Busaobiuah J, Al-Baqshi M, Qadiaub K, Bushrah M, Homrany H, Aljassam A, Khan SA (2013). Prevalence of hepatitis B and C in adult sickle cell disease patients in the eastern province of Saudi Arabia. Journal Applied Hematology 4:33-35 |
|
|
Ulasi II, Ijoma CK (2010). The enormity of chronic kidney disease in Nigeria: the situation in a teaching hospital in south-east Nigeria. Journal of Tropical Medicine pp. 1-6. |
|
|
World Health Organization (2017). Hepatitis Global hepatitis report, |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


