Full Length Research Paper

ABSTRACT
Intrauterine devices (IUDs) are among the most widely used contraceptive methods and users discontinue use despite its effectiveness due to different reasons. This study is aimed at determining the reasons for IUD discontinuation. A retrospective survey was conducted at Family Planning Clinic of University College Hospital, Ibadan, Nigeria. Information on socio-demographic characteristics, IUD - duration of use and reason(s) for removal was obtained using a proforma. Data were analyzed using SPSS version 20.0. A total of 1,961 women had IUD removal within the study period. Mean age and duration of use was 37.8 ±8.6 and 6.2±4.6 years, respectively. Their parity ranged from one to six and majority 528(26.9%) were 30-34 years of age. More than one-third 710(36.2%) had secondary level of education and were mainly grandmultipara. Commonest reasons for IUD discontinuation were side-effects 543 (27.6%) and client’s preference 536(27.3%). About a fifth of them had early IUD discontinuation while majority 651(33.2%) used the device for four to ten years. Thus, IUDs are safe and well tolerated with side effects and client’s preference as commonest reasons for its discontinuation. Providers should provide information on the side effects and its management at insertion knowing that the woman’s choice is paramount.
Key words: Intrauterine devices (IUDs), discontinuation, duration, reasons.
INTRODUCTION
The intrauterine devices have been used worldwide for several years and have been proven safe, effective and convenient by many women (Trieman et al., 1995). Globally, the use of Copper Intrauterine Devices (Cu-IUDs) has increased in the past few decades and it remains the most widely used reversible method (Ali et al., 2011; Seiber et al., 2007). China has the largest proportions of IUD users among married women (33%) while its lowest use is reported in sub-Saharan Africa (0.8%) (Staveteig et al., 2015).
The 2013 Nigeria DHS (demographic health survey) reported a contraceptive prevalence use of 15% among 38,949 women of reproductive age group and population of about 173.6 million. Of these women, 8.1% were currently using intrauterine device (NDHS, 2013).
IUD is a long-term reversible contraceptive that is suitable for women of all reproductive ages and act by causing a foreign-body reaction in the endometrium, with increased prostaglandin production and leukocyte infiltration, thus inhibiting sperm transport and viability, thereby preventing fertilization (Deans and Grimes, 2009; Kenny, 2004). Its efficacy in pregnancy prevention far surpasses other daily and scheduled methods such as pills, patches, and contraceptive rings (Mosher and Jones, 2010). The copper IUD is effective for 12 years and represents the most cost-effective reversible method. This device can be inserted at any time of the menstrual cycle provided it has been ascertained by the health worker that the client is not pregnant. If properly inserted, complications such as perforations, expulsions and pain are prevented (Staveteig et al., 2015).
Up to 50% of women stop using IUDs within five years, most often because of unacceptable vaginal bleeding or pain (NICE, 2005). Staveteig et al. (2015) also reported that IUDs, alongside other modern methods have an average of 20% discontinuation rate due to method-related reasons by the end of three years.
According to Dubuisson et al. (2002), women using copper IUDs are most likely to discontinue it because of bleeding and/or pain. The known complications associated with the use of IUD include its displacement, expulsion from the uterus, perforation of uterus, abnormal uterine bleeding, accidental and ectopic pregnancies. The perceived fear of these complications contributes to its discontinuation. In the UK, cumulative discontinuation rates as high as 17% after one year and 28% after two years for the Cu-IUD has been reported while for the LNG-IUD (Levonogestrol IUD), discontinuation rates were as high as 24% after one year and 33% after two years. Discontinuation rates are up to 50% for all types of IUDs by five years (NICE, 2005).
In Nigeria, the reported discontinuation rates ranged from 2.8–55.1% with a major reason for discontinuation as desire for pregnancy (Okunlola et al., 2009; Jimoh, 2004; Igwe, 2016; Enyindah et al., 2012; Igwegbe et al., 2010). Although IUD is effective and commonly used with a wide-range prevalence of 0.7% in 2003 to 56.7% in 2015 shown in different studies, it is not without side effects. Therefore, aside discontinuing use because of desire for pregnancy, users also request for its removal due to the side effects they experience while using it (NDHS, 2013; Nigeria Commitment Maker, 2012; Dinwoke et al., 2015). It is therefore against this background that this study sought to determine the reason(s) for IUD removal or discontinuation so as to provide information which could be used to enhance services for improving the continuation of IUD use among women who had completed their family size or still desire to space their children.
MATERIALS AND METHODS
This was an 8-year retrospective study from 1st January, 2010 – 31st December, 2017 in the Family Planning Clinic of the University College Hospital, a public health tertiary facility in Ibadan, Oyo State, Southwestern, Nigeria. The family planning clinic runs 8 h each day Monday through Friday with an average attendance of 357 clients per month. Services rendered include counseling, contraceptive uptake, follow up, or removal of contraceptives.
In the family planning clinic, women who presented for contraceptive uptake are first registered and a detailed socio-demographic profile, reproductive and medical history, and history of previous experience with any form of contraceptives are usually obtained from clients at presentation. The client’s height, weight and blood pressure are measured and documented. The women discontinuing the use of a contraceptive method were recorded in the removal record. Clients are counseled on the available methods and each individual is provided with any method she opts for if it is not contraindicated and she is confirmed not to be pregnant via a serum or urine pregnancy test or if menstruating at presentation. All contraceptive methods are provided free, however a token of a thousand naira is collected for consumables from clients seeking provider dependent methods. After the uptake of any family planning method that is provider dependent, the women are followed up with initial monthly visit and then yearly visits to the clinic if on long acting contraceptive. They were however advised to return to the clinic any time they experienced any adverse effect with the method or they wanted to discontinue its use. During each follow-up visit, the provider enquires about any side effects and measures the weight and blood pressure. Reason(s) for discontinuation of use is/are obtained if a client wants to discontinue the use of any contraceptive method.
In this study, early discontinuation of IUD is defined as removal of IUD within the first 12 months after insertion while women removing after 12 months were defined as women who did not discontinue IUD early. Client’s preference is defined as the woman’s desire to switch to another method of contraception, abandonment of all contraception or religious tenets and disposition. Method failure is defined as removal of IUD because the woman became pregnant while using the IUD. Duration of use is defined as the interval between the year or month of insertion and removal.
From the family planning unit, IUD removal records were retrieved and reviewed during the period of study. All women who had their IUD removed during the duration of study were included while women still using this method of contraception or other forms of contraceptive and those who presented for treatment of complication or follow-up were excluded. A standardized proforma was developed to obtain information on the clients’ socio-demographic characteristics, duration of IUD use, reason(s) for IUD discontinuation and its reliability was established. Two research assistants with background medical knowledge trained on the objectives of the study and data collection extracted the information from the medical records. Data were entered and analyzed using SPSS version 20. Descriptive statistics such as: mean, standard deviation, frequency and percentages were used to summarize the result. Also, inferential statistics (chi square) was used to investigate the significant association between the patients’ preference and their characteristics at p<0.05.
RESULTS
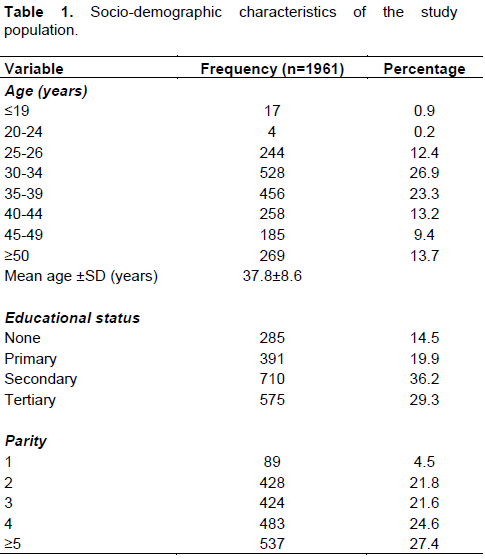
During the period of review, a total of 12,019 women had contraceptive uptake of which 10,189 of them had provider dependent contraceptives. About two-fifth (4085) of them had IUD insertion while 1,961 had removal of IUD. The acceptance and discontinuation rates were 40.1 and 48.0% respectively. The mean age of women who had IUD removal was 37.8 ± 8.6 years and majority 528 (26.9%) were between 30 to 34 years. About two-third 710(65.5%) had at least secondary level of education while 285(14.5%) had no form of education. Only 89(4.5%) of the women who had their IUD removed were primiparous while grand multiparous and para four were 537(27.4%) and 483(21.6%) respectively (Table 1).
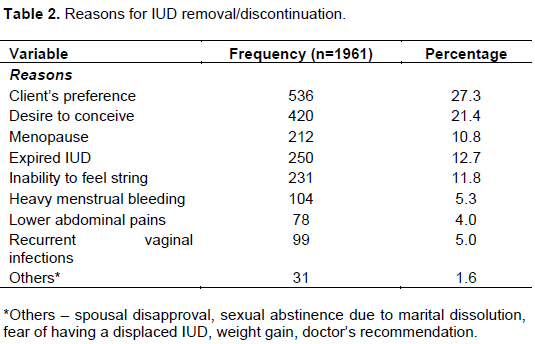
The commonest reason for IUD removal was side effects 543 (27.6%) comprising of heavy menstrual bleeding, lower abdominal pain, recurrent vaginal infections, and inability to feel strings. Other reasons include client’s preference 536(27.3%), desire to conceive 420(21.4%), expired device 250(12.7%), and menopause 212(10.8%) (Table 2).
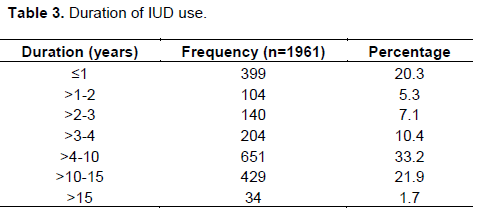
The mean duration of IUD use was 6.2±4.6 years with the shortest duration of use of 1 month and the longest duration of 22 years. About a fifth (399) of the women had early IUD discontinuation while 79.7% of the women did not discontinue the IUD early. The total discontinuation rates were 20.3% at 12 months, 25.6% at 24 months and 32.7% at 36 months. A higher proportion of 651 (33.2%) used the device for four to ten years while 463(23.6%) used it for more than ten years. It was used for >15 years by a few of the women 34(1.7%) (Table 3).
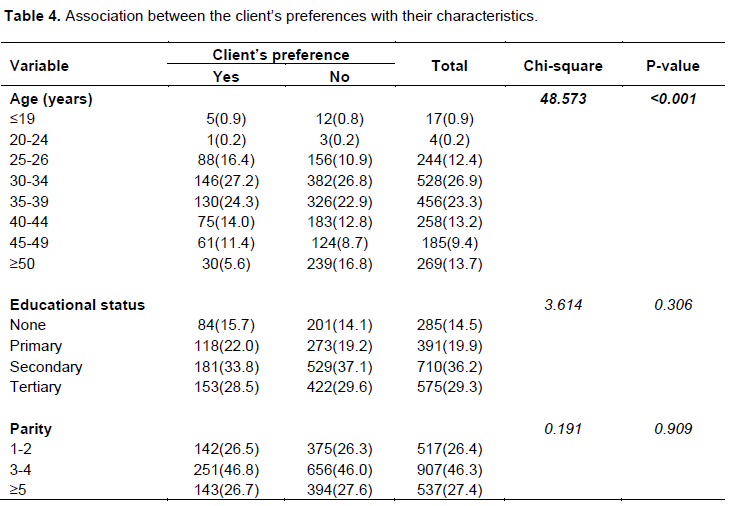
More than a quarter (27.2%) of the women who preferred to discontinue IUD use were in the 30-34 years age group compared with 130(24.3%) and 88(16.4%) in the 35-39 and 25-29 years age groups respectively. A significant relationship exists between client’s preference for discontinuation of IUCD and age (p<0.001) but their educational status and parity were not associated with their preference for discontinuation of IUD at p=0306 and p=0.909 respectively (Table 4).
DISCUSSION
IUDs are effective long acting reversible contraceptive with the health benefit of preventing unwanted pregnancy and its associated consequences though have some side effects. The total discontinuation rate of 48.0% in this present study is higher than the findings in Abakaliki and Jos though lower than that reported in Nnewi (Igwe, 2016; Dinwoke et al., 2015; Anyaka et al., 2016). On the other hand, the discontinuation rates of 20.3% at 12 months, 25.6% at 24 months, 32.7% at 36 months and 42.7% at 48 months is comparable to the findings in a similar study in Nepal with a rate of 21.3% in the first year, 31.3% in the second year, 40.4% in the third year, and 46.5% in the fourth year of insertion (Thapa, 2012).
When compared with the previous study on IUD discontinuation in the same center 15 years earlier, a discontinuation rate of 10.1, 18.4, 22.7 and 26.7% was reported for 12, 24, 36 and 48 months respectively (Okunlola et al., 2009). This shows higher IUD discontinuation rate in our center in recent years but this may be related to the present availability of wider range of contraceptive options. No method failure was reported during the 8 years of reviewing this present study which is similar to a prior 5 years review conducted in our center between 1998 and 2003 (Okunlola et al., 2009).
Majority of the women requesting for IUD removal are within the reproductive age of 30 and 34 years and the mean age at the time of discontinuation was 37.8 ±8.6 years. This observed mean age is higher than the findings of Mutihir et al. (2006) in Jos, North Central Nigeria with a mean age of 32.9 years among the women studied.This might be due to the mean age at marriage which differs in different geopolitical zones in Nigeria. Women in the north central region have a mean age of 18.9 years at marriage while in the southwest it is 21.8 years (NDHS, 2013). Thus, if the device is inserted at an older age, then it will most likely be discontinued at a much older age. Also, Anyaka et al. (2016) study on discontinuation pattern of IUD documented a mean age of 33.6 ± 5.2 years. However, our study supports the report of the Nigeria Demographic Health Survey (NDHS) with the least IUD prevalent rate among women aged 30-34 years while the highest IUD user age group was 40-44 years (NDHS, 2013). Another reason might be possibly because of their desire to conceive since this age group can be regarded as the peak of reproductive age (Ali et al., 2011).
The mean parity of the study population of 3.7±1.4 is at variance with the findings of Anyaka et al. (2016) in Jos with a mean parity of 4.0±2.2 who also reported 0.8% of the population of women discontinued the use of IUD as nulliparous. In this present review, IUD was not inserted or removed for nulliparous women during the study period which is inconsistent with the findings of a study in Nepal (Thapa, 2012). On the other hand, similar to Anyaka et al. (2016) on findings of highest proportion of grand multiparous women requesting for IUD removal, we also observed that majority of women requesting for discontinuation of the IUD during the study period were grandmultiparous (Anyaka et al., 2016). This could be because the grandmultiparous women are close to menopausal age considering the preponderance age of grandmultiparity in our environment from different studies (NDHS, 2013; Anyaka et al., 2016). Moreover, several studies have documented that nulliparous and primiparous women have better IUD continuation rates compared with the multiparous women (Ali et al., 2011; Igwe, 2016; Dickerson et al., 2013).
In this study, discontinuation of IUD was highest among women with secondary education owing to the fact that women with secondary level of education were the highest proportion of the population studied. Interestingly, the opposite was reported in Calabar in that the secondary literates constituted the majority presently using IUD (Iklaki et al., 2015). Conversely, a higher proportion of the women discontinuing IUD use had tertiary level of education in a study in Abakaliki, Nigeria (Igwe, 2016).
Unlike the previous studies in Nigeria - Jos (Muthir et al., 2016; Anyaka et al., 2016), Abakaliki (Igwe, 2016), Ibadan (Okunola et al., 2009) and Calabar (Iklaki et al., 2015), “desire to get pregnant” was commonest reason for discontinuation, but in our study, the main reason for removal or discontinuation was the side effect(s) of IUD which accounted for 27.6% of the total request for removal during the study period. Also, the NDHS in 2013 identified desire to become pregnant as the commonest reason for IUD discontinuation (NDHS, 2013). However, desire to conceive was the reason for IUD discontinuation in about a fifth of the women studied which makes it evident that quite a number of them had used IUD for child spacing. On the other hand, the World Health Organization (WHO), reported side effects of IUD as the commonest reason for its discontinuation in an inter-country study across 14 countries in Latin America, Caribbean, North Africa, West Asia, South-Central and South-East Asia (Ali et al., 2011). Our finding also substantiates the report from Nepal with side effects of IUD as the commonest indication for IUD discontinuation (Thapa, 2012).
In addition, clients’ preference defined in this context as the woman’s desire to switch to another method of contraception, abandonment of all contraception (despite indicating not wishing to become pregnant) or religious tenets and disposition was the second commonest reason for IUD discontinuation. Similarly, some studies have found that majority of women who discontinue IUD use do so without switching to any other methods or switched to either short-term, implants, permanent contraception or traditional methods (Azmat et al., 2013; Ali et al., 2011). Age was found to influence IUD discontinuation due to client’s preference, but their educational status and parity was not statistically significant. This agrees with the previous similar study in our center in which educational status was found not to influence IUD discontinuation though they did not consider the client’s preference (Okunlola et al., 2009).
Furthermore, spousal disapproval was stated as the reason for IUD discontinuation in only five (0.3%) of the women studied compared with 7.0% who reported husband’s view as one of the reasons for discontinuation in a previous study in UCH, Ibadan (Okunlola et al., 2009). This could indicate that men are currently more involved in contraceptive uptake in Nigeria which is one of the key factors that drives increase in family planning uptake (Orji et al., 2007; Wambui et al., 2009).
The mean duration of IUD use was 6.2±4.6 years with the shortest duration of use of 1 month and the longest duration of 22 years. Likewise, 1.9% of women discontinued IUD at 1 month in a Pakistan study (Azmat et al., 2013). About 20.3% of the women had early IUD discontinuation which corroborates the study in Nepal where the same findings was reported but when compared with Ojiyi et al. (2011) and Thapa (2012) findings, about 33.1% of their study population discontinued IUD in less than a year majorly because of its complications. The high proportion of early IUD discontinuation rate in this study will result in a decrease in its prevalence, could discourage its uptake by other clients and increase the unmet need of family planning if clients who discontinue its use do not switch to other forms of family planning methods. However, the average duration of uninterrupted IUD use ranges from two or more years to a little over the three years (37 months) in several studies among women who desire to space their children (NDHS, 2013; Igwe, 2016; AI-Inany, 2007). A higher proportion used the device for four to ten years in our study.
Surprisingly, a significant number of women used IUD for greater than 10 years before its discontinuation despite the counseling they received on duration of IUD effectiveness at insertion though all of them were menopausal. Some studies have also reported prolonged IUD use after menopause, either as a deliberate act or because the woman forgets (Sujatha, 2012; Sinha et al., 2015; Wagner and Gimpelson, 2012). This calls for review of the counseling techniques and instructions given to women receiving IUD by the family planning providers and the need to reemphasize the effects of prolonged IUD use like post-menopausal bleeding and upper genital tract infection to women who are 35 years and above receiving IUD (Sujatha, 2012; Sinha et al., 2015; Wagner and Gimpelson, 2012).
This study is not without limitations considering its retrospective nature and the narrow range of available data. It is recommended that this study be replicated as a prospective study so as to explore in detail what the clients’ preferences are and reason(s) for their change in preference as regards discontinuation of IUD so as to obtain information on their method switch behavior. Also, the report of some side effects like heavy menstrual bleeding, and dysmenorrhea had been subjective and could have been qualified prior to initiation of contraception and followed up to ascertain the quantity of bleeding - light, moderate, moderately heavy, or heavy or severity of dysmenorrhea – mild, moderate or severe.
CONCLUSION
IUDs are the most preferred, widely tolerated modern contraceptive and its discontinuation while still in need of FP could be problematic which leaves the woman at risk of an unwanted pregnancy. Despite this, furthermost reason for discontinuation is client’s preference as compared to the desire to conceive from previous studies. However, discontinuation due to method failure was not recorded during the review period indicating the efficacy of the contraceptive method. In general, family planning (FP) providers should counsel all clients seeking contraceptives on all the available options, their side effects and its management before uptake as well as identify the women at a higher risk of early discontinuation which will promote the continuation of IUD as contraception and reduce the high unmet need of family planning in Nigeria.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ali M, Sadler R, Cleland J, Ngo T, Shah I (2011). Long-term contraceptive protection, discontinuation and switching behaviour. Intrauterine Device (IUD) Use Dynamics in 14 developing Countries. London: World Health Organization and Marie Stopes International. |
|
|
Al-Inany H (2007). Current state of intrauterine contraceptive devices. Middle East Fertility Society Journal 12(1):8-12. |
|
|
Anyaka C, Ocheke A, Shambe I, Kahansim M, Oyebode T, Pam V, Ekwempu C (2016). Discontinuation pattern among intrauterine contraceptive device users at Jos University Teaching Hospital, Jos, Nigeria. Journal of Gynecology and Obstetrics 4(6):53-56. |
|
|
Azmat SK, Hameed W, Mustafa G, Hussain W, Ahmed A, Bilgrami M (2013). IUD discontinuation rates, switching behavior, and user satisfaction: findings from a retrospective analysis of a mobile outreach service program in Pakistan. International Journal of Womens Health 5:19-27. |
|
|
Deans EI, Grimes DA (2009). Intrauterine devices for adolescents: a systematic review. Contraception 79(6):418-423. |
|
|
Dickerson LM, Diaz VA, Jordon J, Davis E, Chirina S, Goddard JA, Carr KB, Carek PJ (2013). Satisfaction, early removal, and side effects associated with long-acting reversible contraception. Family Medicine 45(10):701-707. |
|
|
Dinwoke VO, Okafor CI, Eke A (2015). Intrauterine contraceptive device acceptors in Nnamdi Azikiwe University Teaching Hospital, Nnewi, Southeastern Nigeria - A 5-year review. Tropical Journal of Medical Research 18(2):68-73. |
|
|
Dubuisson JB, Mugnier E, Mirena Study Group (2002). Acceptability of the levonorgestrel-releasing intrauterine system after discontinuation of previous contraception: results of a French clinical study in women aged 35-45 years. Contraception 66(2):121-128. |
|
|
Enyindah CE, Ojule JD, Bassey G (2012). Contraception with intrauterine contraceptive device in Port Harcourt, South-South Nigeria. Journal of Medicine and Biomedical Research 11(1):35-45. |
|
|
Igwe NM (2016). Intrauterine contraceptive device use in Abakaliki, Southeast Nigeria: A 5-year review. Tropical Journal of Medical Research 19(2):138-143. |
|
|
Igwegbe AO, Ugboaja JO, Monago EN (2010). A ten-year clinical experience with intrauterine contraceptive device (IUCD) in a Nigerian tertiary health institution. International Journal of Medicine and Medical Science 2(11):347-353 |
|
|
Iklaki CU, Agbakwuru AU, Udo AE, Abeshi SE (2015). Five-year review of copper T intrauterine device use at the University of Calabar Teaching Hospital, Calabar. Contraception 6:143-147. |
|
|
Jimoh AA (2004). Complications of intrauterine device (IUD) use in University of Ilorin Teaching Hospital Ilorin. Nigeria Journal of Medicine 13(3):244-249. |
|
|
Kenny L (2004). Contraception (Intrauterine contraceptive devices). In: Luesley DM, Baker P, Drife J, editors. Obstetrics and Gynaecology: An Evidence-Based Text for MRCOG. London: Hodder Arnold 520-521. |
|
|
Mosher WD, Jones J (2010). Use of contraception in the United States: 1982-2008. Vital Health and Statistics 23:29:1-44. |
|
|
Mutihir JT, Ujah IA, Uduagbamen PF (2006). Indications for removal of intrauterine contraceptive device in Jos, North Central Nigeria. Nigeria Journal of Clinical practice 9(2):105-180. |
|
|
NICE (National Institute for Health and Clinical Excellence) (2005). Long-acting Reversible Contraception. |
|
|
Nigeria Commitment Maker (2012). Core Indicator Estimates.FP 2020. |
|
|
Nigeria Demographic Health Survey (2013). NDHS Final report. |
|
|
Ojiyi EE, Dike EI, Anolue FC, Okeudo C, Uzoma OI, Uzoma MJ, Agu PO, Anozie UM (2011). Complications of (IUCD) among users in Orlu, Nigeria. Webmed Central Obstetrics and Gynaecology 2(12):WMC002557. |
|
|
Okunlola MA, Owonikoko KM, Robert OA, Morhason-Bello IO (2009). Discontinuation pattern among IUCD users at the family planning clinic University College Hopsital, Ibadan. Journal of Obstetrics and Gynaecology 26(2):152-156. |
|
|
Orji EO, Ojofeitimi EO, Olanrewaju BA (2007). The role of men in family planning decision-making in rural and urban Nigeria. European Journal of Contraceptive and Reproductive Health Care 12(1):70-75. |
|
|
Seiber EE, Bertrand JT, Sullivan TM (2007). Changes in Contraceptive Method Mix in Developing Countries. International Family Planning Perspective 33(3):117-123. |
|
|
Sinha M, Rani R, Gupta R, Chand K, Kaur G (2015). Lippes Loop Inserted 45 Years Back: The Dilemma to Remove It or Leave It in situ. A Case Report with Review of Literature. Journal of Clinical Diagnosis Research 9(4):QE01-QE5. |
|
|
Staveteig S, Mallick L, Winter R (2015). Uptake and Discontinuation of Long-Acting Reversible Contraceptives (LARCs) in Low-Income Countries. DHS Analytical Studies No. 54. USAID. |
|
|
Sujatha VV (2012). Forgotten intrauterine devices presenting with pre- and postmenopausal bleeding: a case series. Tropical Doctor 42(1):56-57 |
|
|
Thapa S (2012). Early discontinuation of intrauterine device in Nepal - a retrospective study. WHO South-East Asia Journal of Public Health 1(3):309-319. |
|
|
Trieman K, Liskin L, Kols A, Rinehart W (1995). IUDa-Update. Population Reports, School of Public Health, Baltimore, series B 6:1-34. |
|
|
Wagner CA, Gimpelson RJ (2012). Postmenopausal bleeding due to a Cu-7 intrauterine device retained for thirty years. Journal of the Society of Laparoendoscopic Surgeons 16(2):329-332. |
|
|
Wambui T, Ek AC, Alehagen S (2009). Perceptions of family planning among low-income men in Western Kenya. International Nursing Review 56(3):340-345. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


