Full Length Research Paper

ABSTRACT
The severity of sickle cell anaemia (SCA) often causes painful episodes of vaso-occlussive crises and affects quality of life. Poor health-related quality of life (HRQoL) associated with sickle cell disease has been established. The study aim was to determine the relationship between pain index and HRQoL in Nigerian patients with SCA. The study was a cross-sectional survey of SCA individuals. Data collection was done using socio-demographics and clinical characteristics questionnaire, Wong-Baker FACES pain rating scale, and WHOQoL-Bref. Descriptive, cross-tab and multinomial logistic regression analyses were used to analyze the data in SPSS® version 20 IBM, USA. A total of 226 SCA individuals (males = 111 (49.1%) and females = 115 (50.9%)) with mean age 28.9±8.5 years participated in this study. Greater than 80% of the SCA individuals with pain had poor HRQoL score. Overall, with the range of statistically significant Chi-square value 49.715-94.474 (Cramer’s V = 0.469-0.647), strong association was observed between pain index and all HRQoL domains. Logistic regression analysis also revealed pain rating (pain relative to no pain) significantly predicted increased odds of affecting physical health (OR = 5.030; 95% CI = 1.094-23.118; P value = 0.038) as well as social and relationship status (OR = 9.443; 95% CI = 3.228-27.618; P value < 0.001) among SCA individuals. In conclusion, individuals with SCA largely have poor HRQoL. However, pain affects domains of HRQoL, particularly the physical health and social and relationship status domains of health.
Key words: Sickle cell anaemia (SCA), pain, health-related quality of life (HRQoL), World Health Organization Quality of Life-Bref (WHOQoL-Bref).
INTRODUCTION
Sickle cell anaemia (SCA) affects about 20 million people globally including about 2 to 3% of Nigerian population (Nasimuzzaman and Malik, 2019; Adewoyin, 2015). With Nigeria contributing disproportionately to the burden, nearly 90% of children with sickle cell disease born in sub-Saharan Africa die mostly before age 5 (Wonkam et 2020; Nasimuzzaman and Malik, 2019; Oshikoya et al., 2015). This mortality burden in sub-Saharan Africa is reportedly compounded by secondary challenges including poor healthcare system, malaria, infectious diseases and poverty (Wonkam et al., 2020). Nigeria is also among the three countries that account for over half of the 305,000-312,000 total annual births with SCA globally (Williams, 2016). These epidemiological data suggest the extent of SCA burden in Nigeria and sub-Saharan Africa as compared to other regions of the world.
Sickle cell anaemia is the most severe genetic variant of sickle cell disease (SCD) that is an inherited autosomal recessive disorder (Driss et al., 2009). It is characterized by homozygosity for hemoglobin S (HbSS) (Isoa, 2009). The formation of haemoglobin S (HbS) is due to point mutation in the β-globin gene that substitutes an amino acid residue, glutamate for a valine residue at position 6 (Gladwin and Sachdev, 2012). This mutation structurally affects HbS conformation, causes HbS polymerization with consequent impact on the erythrocytes, and sickling phenomenon ensues (Quinn, 2016; Gladwin and Sachdev, 2012). These events are underlying causes of devastating complications of SCA including painful episodes of vaso-occlusive crises (Quinn, 2016). Sickle cell anaemia results in many devastating sequelae or sickle cell crises including chronic hemolytic anaemia, painful vaso-occlusive crises and inflammation, priapism, infections, and multisystem or multi-organ damage with manifestations of inflammation, vasculopathy, thrombosis, stroke, acute chest syndrome, pulmonary hypertension, avascular necrosis, renal damage and nephropathy (Piccin et al., 2019).
Episodes of these painful crises have been reported to be triggered by environmental and psychological factors (Oshikoya et al., 2015). Acute and chronic pains are both eventful among SCA patients; however, chronic pain has been reported to be mostly experienced than acute pain which is associated with vaso-occlusive crises. Less active social lifestyle, low appetite, sedentary lifestyle, decreased mobility, and undesirable feeling of fear, anxiety, stigmatization, depression, hatred, inability to complete education, sleep disturbance, and tendency of drug abuse have all been correlated with sickle cell diseases and associated chronic pain (Rizio et al., 2020; Williams and Tanabe, 2016; Adewoyin, 2015). Hence, the burden of SCA has sociological, physiological and psychological impacts (Jenerette and Brewer, 2010); and could bear negative impact on quality of life (Locke et al., 2015).
Although previous studies from different parts of the world described health-related quality of life in SCD-associated pain and different measurement instruments were used (Rizio et al., 2020; Britto da Cunha et al., 2020; Nwagha and Omotowo, 2020; Esham et al., 2020; Boulassel et al., 2019; Constantinou et al., 2015; Beverung et al., 2015; Al Jaouni et al., 2013; Dale et al., 2011). Rizio et al. (2020) stated that painful vaso-occlusive crises is one of the most debilitating sequelae experienced by SCD patients, and minimal research has yet been done on this aspect in relation to impact on patients’ quality of life. Perhaps there are gaps in researches, as touching relationships between SCD-related pain and quality of life, which are emanating from different parts of the world, particularly from Africa where SCD is endemic. Nevertheless, researches done in Nigeria involving SCD and quality of life adjusted for demographics effect on health-related quality of life, but no data was revealed on pain index effect on health-related quality of life (Nwagha and Omotowo, 2020; Nwogoh et al., 2016; Anie et al., 2010). This calls for continuous research, principally in the aspect of pain and quality of life in SCD. Hence, this present study was aimed at studying the impact of pain on health-related quality of life of a Nigerian population with sickle cell anaemia. The relationship between pain index and health-related quality of life of Nigerian population with sickle cell anaemia was the major highlight of this study.
METHODOLOGY
Ethics and participants
A cross-sectional survey approach was used for this study. The study was carried out in 2019 at the Adult Haematology Clinic of the Lagos University Teaching Hospital (LUTH), Lagos, Nigeria. The method of convenient sampling was used to recruit participants during the study period. According to data on the proportion of a specific group of Nigerian SCA individuals with poor quality of life as reported by Nwagha and Omotowo (2020), sample size was determined using cross-sectional study sample size formula for qualitative variable as described by Charan and Biswas (2013). With Z1-α/2 (Z score at 95.0% confidence limit) = 1.96, P (the previous study reported proportion of SCA individuals with poor quality of life in Nigeria) = 18.2%, and d (absolute precision at 5%) = 0.05, the calculated sample size was 229. The SCA status of participants was validated through medical records made available at the clinic before they were recruited into the study. Additionally, only participants who gave informed consent participated in the study. Moreover, prior to the commencement of this study, ethical approval was obtained from the LUTH Health Research Ethics Committee. Individuals with already established cognitive or behavioural dysfunction, stroke, congenital diseases, diabetes, or cancer were excluded from the study. Totally, 226 SCA individuals including 111 males and 115 females participated in this study.
Measures
A structured questionnaire covering some demographics and clinical aspects of SCA with few pain-related questions, Wong-Baker Pain Rating Scale, and World Health Organization Quality of Life-Bref (WHOQoL-Bref) measurement instruments were used in this study. The questionnaire was self-administered, and support was provided when required. Age, gender, marital status, religion, educational level, academic performance, and employment status were socio-demographic factors of focus in this study.
Pain
Degree of pain was assessed through Wong-Baker FACES pain rating scale instrument described by Garra et al. (2010). The range of the pain rating scale scoring was from 0 to 5. Scores 0 (no hurt) and 1 (hurts little bit) were interpreted as “no pain,” while scores 2 (hurts a bit more), 3 (hurts even more), 4 (hurts whole lot) and 5 (hurts worst) were interpreted as “pain.” The categorization of the pain rating scale score as “no pain” or “pain” was based on a subjective evaluation of the Wong-Baker FACES pain rating chart interpretation in linkage with possibility of pain severity, daily activity interference or bodily function impairment. The frequencies of “no pain” and “pain” were analyzed, and used for logistic regression analysis for prediction of pain index effect on HRQoL. The level of knowledge about pain, pain interference with social life activities, and short-term severity of pain experienced in previous 4 weeks before participation in the survey were also assessed using the pain-related questions in the general questionnaire. Likert scale scoring ranges of 1-4 was used, respectively. The level of knowledge about pain was graded as poor = 1, fair = 2, good = 3, and very good = 4. Pain interference with social life activities variable grading was as follows: not at all = 1, a little bit = 2, moderately = 3, and extremely = 4. Additionally, the scale used for short-term severity of pain experienced in previous 4 weeks measurement was none = 1, mild = 2, moderate = 3, and severe = 4.
Health-related quality of life
The World Health Organization Quality of Life-Bref (WHOQoL-Bref) instrument was used to assess HRQoL (WHO, 1996). The WHOQoL-Bref has four main domains and general health section including a total of 26 questions. “Domain 1” is for physical health, “Domain 2” stands for psychological health, “Domain 3” represents social and relationship, while “Domain 4” encodes environment status. According to standard protocol, the order of options or responses to 3 questions (questions 3, 4 and 26) that have negative impact on the total HRQoL scoring outcome were reversed such that score 5=1, 4=2, 3=3, 2=4 and 1=5. The scale scoring range was from 1 to 5. The transformed scores of each domain were computed by calculating the mean of the questions in the domain and multiplying by 4. The maximum score for each domain is 20. Score <12 that was equivalent to <50 on the transformed score scale as given by the WHO manual was classified as “poor” quality of life, while scores ≥12 that was equivalent to ≥50 on the transformed score scale was classified as “good” quality of life (WHO, 1996). Additionally, the reliability of the WHOQoL-Bref questionnaire with the participants’ responses was computed by determination of Cronbach’s alpha value that was found to be 0.836. The frequency of the responses of the participants was analyzed.
Statistical analysis
The data collected were collated and managed on Microsoft Excel Spreadsheet (v2013). The data were then analyzed using Statistical Package for Social Sciences (SPSS®) version 20 IBM, USA. Data were cleaned of inconsistencies and checked for completeness, and descriptive statistics of variables were presented as frequencies. Association of HRQoL with pain rating was determined by Chi Square test through cross-tab analysis. Adjusting for pain index, the relationship or effect of pain rating on HRQoL outcome was analyzed using multinomial logistic regression. Confidence interval was set at 95%.
RESULTS
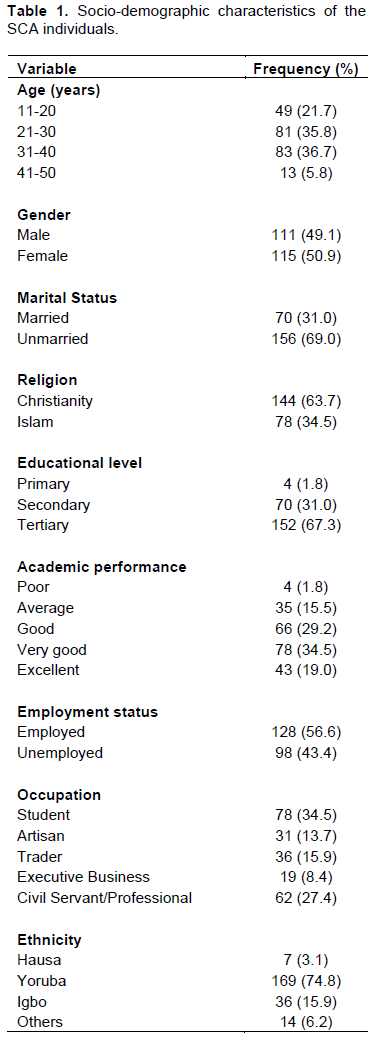
A total of 226 SCA individuals with age range 11-50 years and mean age 28.9±8.5 years participated in this study. These included 111 males (49.1%) and 115 females (50.9%). The respondents were predominantly 11-40 years of age whereas 5.8% were 41 years and older. The respondents were predominantly unmarried (69.0%), practicing Christianity (63.7%), and educated with, at least, secondary level of education (secondary (31.0%) and tertiary level (67.3%)) and over average academic performance combined (good (29.2%), very good (34.5%) and excellent (19.0%)). In addition, 56.6% were employed and 43.4% unemployed, 34.5% and 27.4% were students and civil servants/professionals, respectively, and 74.8% belonged to Yoruba ethnic group (Table 1).
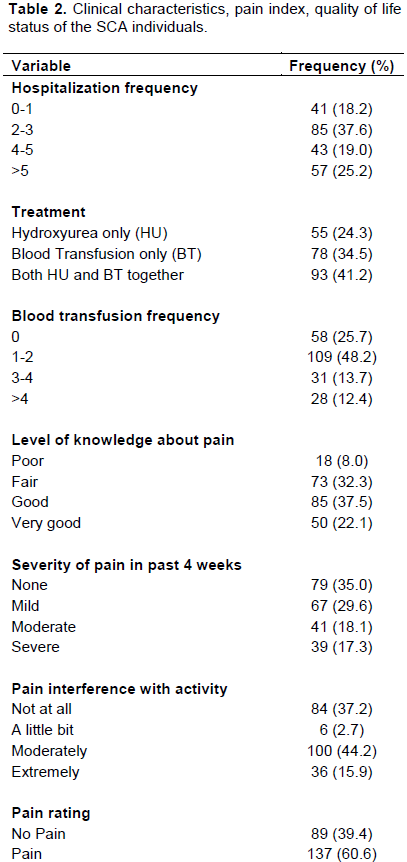
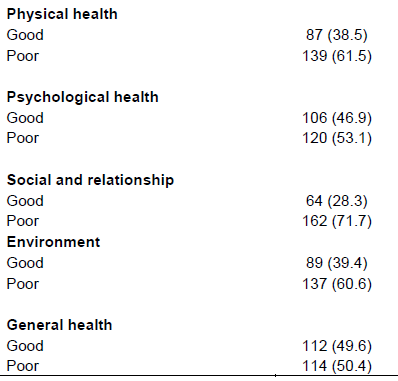
The frequency distribution of clinical characteristics assessed revealed about 81% of respondents had ≥2 hospital admission while about three-quarter of the respondents had received blood transfusion ≥1 time. Majority used both hydroxyurea and blood transfusion (41.2%) treatment modalities together. Meanwhile, a lower proportion of the respondents used hydroxyurea only (24.3%) as well as blood transfusion only (34.5%). Only 18% had poor knowledge about pain. A higher proportion of the respondents had mild to severe degree of pain within 4 weeks before survey. Additionally, moderate and extreme levels of pain interference with activity were indicated by majority of the respondents. The FACES pain rating revealed 60.4% had some degree of pain. About 61.5, 53.1, 71.7, 60.6 and 50.4% of the respondents had poor physical health, psychological health, social and relationship, environment and general health score, respectively (Table 2). Although data was not shown, the mean score for physical health was 9.6±2.1 (range = 4.0-14.0) and 10.0±2.5 (range = 6.22-26.7) for psychological health. Social and relationship was 7.1±1.7 (range = 2.7-10.0), environment was 9.6±2.2 (range = 5.09-14.55), and general health was 10.522±3.626 (range = 0.00-16.00).
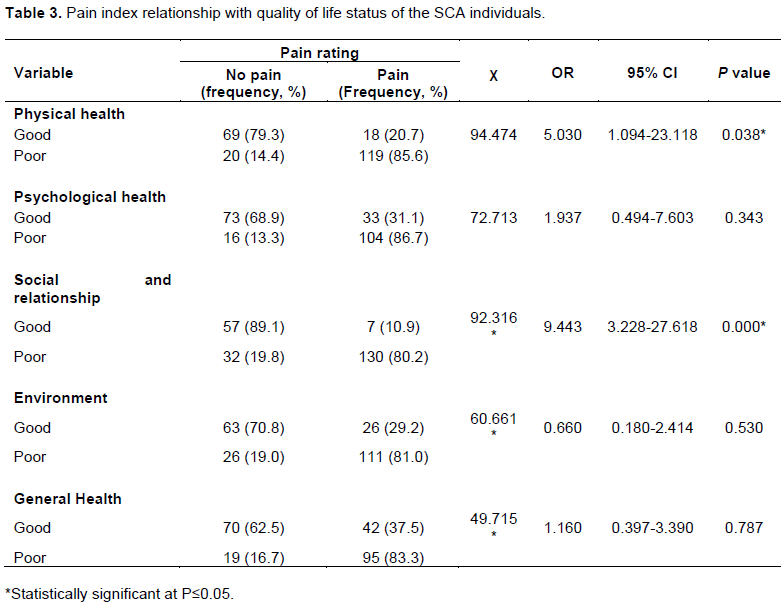
Furthermore, 85.6, 86.7, 80.2, 81.0 and 83.3% of the SCA individuals with pain had poor quality of life score in each of the HRQoL domains (physical health, psychological health, social and relationship, environment status) and general health (Table 3). Overall, statistically significant strong association was observed between pain index and each of the quality of life domains including physical health (c2 = 94.474; Cramer’s V = 0.647; P value < 0.001), psychological health (c2 = 72.713; Cramer’s V = 0.567; P value < 0.001), social and relationship (c2 = 92.316; Cramer’s V = 0.639; P value < 0.001), environment status (c2 = 60.661; Cramer’s V = 0.518; P value < 0.001) and general health (c2 = 49.715; Cramer’s V = 0.469; P value < 0.001). Moreover, relative risk assessment in the crosstab analysis further revealed that it is generally more likely for SCA individuals with no pain to have good quality of life (from physical to general health) relative to individuals with pain. Logistic regression analysis revealed the odds of pain rating (pain relative to no pain) impacting quality of life status. Pain rating significantly predicted the increased odds of affecting physical health (OR = 5.030; 95% CI = 1.094-23.118; P value = 0.038) and status of social and relationship (OR = 9.443; 95% CI = 3.228-27.618; P value = 0.000) among SCA individuals (Table 3).
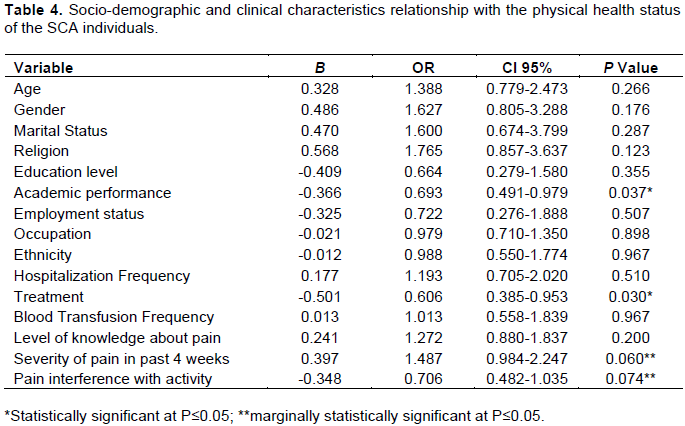
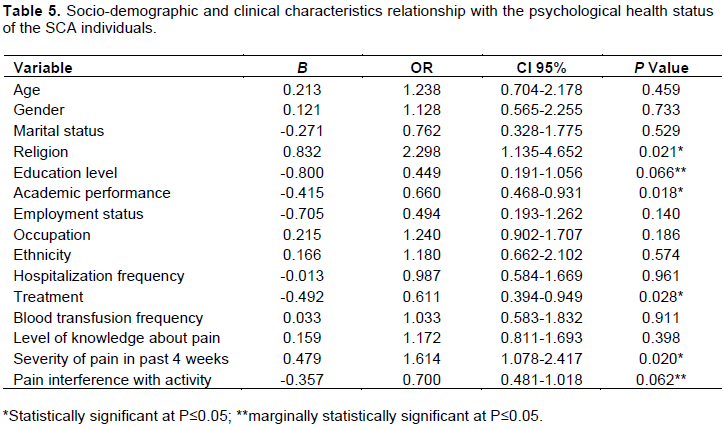
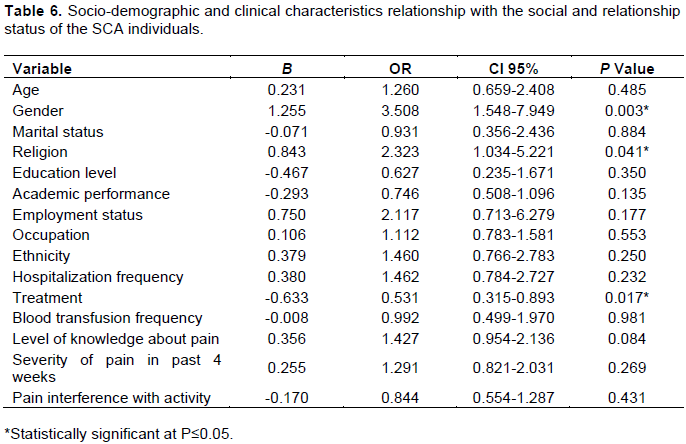
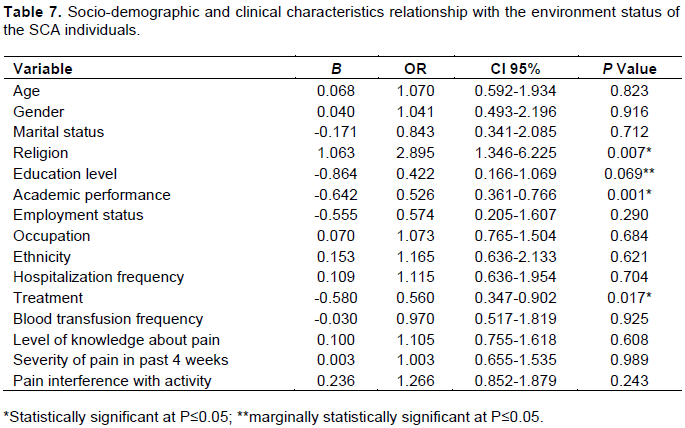
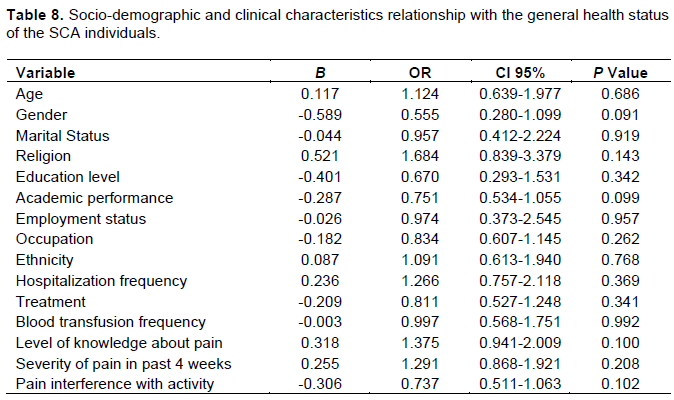
Multinomial logistic regression was used to predict the odds of SCA individuals having poor quality of life score (relative to good score) under the effect of a specific demographical factor evaluated when other factors are held constant. Academic performance, treatment modality, religion, gender, degree of pain severity within 4 weeks before survey, level of interference of activity by pain, and level of education significantly or marginally significantly predicted the odds of having poor physical health, psychological health, social and relationship, environment status score relative to good score among SCA individuals (Tables 4 to 8).
DISCUSSION
Sickle cell anaemia is the most severe form of sickle cell disease that leads to painful episodes of vaso-occlusive crises and affects quality of life. Health-related quality of life is a commonly characterized assessment of human health, even in diseased state. Poor health-related quality of life associated with sickle cell disease has been established by several studies (Dale et al., 2011; Nwogoh et al., 2016; Ojelabi et al., 2019). However, we studied the relationship between pain index and health-related quality of life among Nigerian SCA population. The slightly higher proportion of female than male in this study is corroborated by previous studies that revealed gender imbalance in SCD distribution with females higher than males, even in terms of risk of complications (Jaffer et al., 2009; Nwogoh et al., 2016; Ojelabi et al., 2019). However, there were some contradictory reports where male frequency distribution was higher than female (Faremi and Oyeninhun, 2020; Fernandes et al., 2015; Amr et al., 2011). These discrepancies could be associated with the age groups sampled. Some studies that targeted adolescents reported higher male to female ratio (Faremi and Oyeninhun, 2020; Fernandes et al., 2015; Amr et al., 2011) while those that included adults reported higher female to male ratio (Ojelabi et al., 2019; Nwogoh et al., 2016; Jaffer et al., 2009). With mean age of study participants at 28.9±8.5 years (range 11-50 years) and more than half the total participants employed (56.6%), we may well have had good representation among adults with SCA.
The observed good knowledge about pain by over 80% of the total participants suggests validation of responses to pain index related questions. With the aid of Wong-Baker FACES pain rating, the predominance of pain (60.4%) was observed among the Nigerian SCA cohort. Although there is no general consensus in the measures used for pain assessment in similar previous studies, outcomes reported corroborated our findings on high prevalence of pain in sickle cell disease (Valrie et al., 2020; Sil et al., 2016; Ezenwa et al., 2016). The finding of severity of pain experienced and pain interference with activities among SCA individuals were also widely supported by previous studies (Valrie et al., 2020; Sil et al., 2016; Ezenwa et al, 2016).
Health-related quality of life is a subjective or perceptive assessment of several components of wellbeing including physical health, psychological health, social and relationship status, environment, and general health (Nwogoh et al., 2016). Generally, the high prevalence of poor physical health (61.5%), psychological health (53.1%), social and relationship (71.7%), environment (60.6%) and general health (50.4%) among the Nigerian SCA cohort showed poor HRQoL among this population under investigation. In support of our observation, Britto da Cunha et al. (2020) reported poor HRQoL in 48.08% of children with SCA in Brazil. In addition, Faremi and Oyeninhun (2020) revealed over 85% of SCD individuals with low quality of life. Academic performance, treatment modality, religion, gender, degree of pain severity, level of interference of activity by pain, and level of education were major predictors of having poor HRQoL among SCA individuals. Moreover, previous studies highlighted age, educational level, health quality, anxiety, depression and conducive environment as predictors of quality of life (Nwagha and Omotowo, 2020; Ojelabi et al., 2019; Adzika et al., 2017).
In accordance with the present observation, Britto da Cunha et al. (2020) also revealed a higher proportion of SCA individuals (>56%) with poor HRQoL had pain.
With over 80% of SCA individuals with pain having poor quality of life score, we found statistically significant strong association between pain index and HRQoL domains. This suggests that the experience of pain among SCA individuals have relative effect on HRQoL domains. This finding is supported by Esham et al. (2020), who revealed that pain intensity is linked with impairments of many domains of HRQoL. Moreover, Rizio et al. (2020), who reported significant impact of pain measured by frequency of vaso-occlusive crisis on HRQoL in SCD, revealed that physical, social and emotional domains of HRQoL were largely affected. This observation supports our multinomial logistic regression analysis that showed pain significantly predicted the increased odds of affecting physical health and status of social and relationship among SCA individuals. Cooper et al. (2019) also found significant interactions between pain and physical component of HRQoL.
Several HRQoL assessment instruments have been utilized in different studies. The WHOQoL-BREF (Al Jaouni et al., 2013), generic children’s QoL measure (GCQ) (Constantinou et al., 2015), PedQL™ (Boulassel et al., 2019; Dale et al., 2011), PROMIS (patient-reported outcomes measurement information system) Global Health, and adult sickle cell quality of life measurement system (ASCQ-Me) (Esham et al., 2020; Cooper et al., 2019) are some examples among others. These assessment or measurement tools have been found to be HRQoL in SCD, revealed that physical, social and emotional domains of HRQoL were largely affected. This reliable, but may skew research findings and sometimes make comparative analysis or systematic review almost impossible. It recommends harmonization of HRQoL assessment tool for clinical research and practice across the world. Apparently, this study has presented findings related to relationship between pain index and HRQoL. However, it is quite important to highlight some gaps. Firstly, this study was carried out in a single tertiary health facility in Lagos State, which is just a state out of the 36 states of Nigeria. Thus, our findings might not be a generalized representation of what is obtainable across Nigeria. Perhaps, a systematic review of similar studies across the country may give a meta-analyses of this study interest. But in order to achieve this systematic review, more original research articles within this research scope across Nigeria are quite needed. Secondly, we also felt that economic status might provide a cushion effect that may enhance HRQoL. Thus, comparative analysis of the relationship between pain index and HRQoL among SCA individuals from poor and rich background might be noteworthy. Lastly, the logistic regression approach utilized was multinomial. The use of the covariates approach helped us to simplify the generalized effect of the socio-demographics and clinical characteristics. There were many of them (socio-demographics and clinical characteristics). As such, reference group for each of the factors could not be indicated. So there is need to use a simplified approach to aid the results. Adzika et al. (2017) used similar generalized approach for regression analysis.
CONCLUSION
This study concludes from the data with literature comparisons that pain affects domains of health-related quality of life, particularly the physical health and social and relationship status domains of health. Additionally, high prevalence of poor physical health (61.5%), psychological health (53.1%), social and relationship (71.7%), environment (60.6%) and general health (50.4%) was found among the Nigerian SCA cohort.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adewoyin AS (2015). Management of sickle cell disease: a review for physician education in Nigeria (sub-saharan Africa). Anemia 2015, 791498. |
|
|
Adzika VA, Glozah FN, Ayim-Aboagye D, Ahorlu CSK (2017). Socio-demographic characteristics and psychosocial consequences of sickle cell disease: the case of patients in a public hospital in Ghana. Journal of Health, Population and Nutrition 36(1):4-4. |
|
|
Al Jaouni SK, Al Muhayawi MS, Halawa TF, Al Mehayawi MS (2013). Treatment adherence and quality of life outcomes in patients with sickle cell disease. Saudi Medical Journal 34(3):261-265. |
|
|
Amr MA, Amin TT, Al-Omair OA (2011). Health related quality of life among adolescents with sickle cell disease in Saudi Arabia. Pan African Medical Journal 8:1. |
|
|
Anie KA, Egunjobi FE, Akinyanju OO (2010). Psychosocial impact of sickle cell disorder: perspectives from a Nigerian setting. Global Health 6(2):1-6. |
|
|
Beverung LM, Strouse JJ, Hulbert ML, Neville K, Liem RI, Inusa B, Fuh B, King A, Meier ER, Casella J, DeBaun MR, Panepinto JA (2015). Health-related quality of life in children with sickle cell anemia: impact of blood transfusion therapy. American Journal of Hematology 90(2):139-143. |
|
|
Boulassel MR, Al-Badi A, Elshinawy M, Al-Hinai J, Al-Saadoon M, Al-Qarni Z, Khan H, Qureshi RN, Wali Y (2019). Hemoglobin F as a predictor of health-related quality of life in children with sickle cell anemia. Quality of Life Research 28(2):473-479. |
|
|
Britto da Cunha V, Freitas de Andrade Rodrigues C, Alves Rodrigues T, Silva Gomes de Oliveira EJ, Santos Garcia JB (2020). Self-Report for Assessment of Pain and Quality of Life in Children with Sickle Cell Anemia in a Developing Country. Journal of Pain Research 13:3171-3180. |
|
|
Charan J, Biswas T (2013). How to calculate sample size for different study designs in medical research? Indian Journal of Psychological Medicine 35(2):121-126. |
|
|
Constantinou C, Payne N, Inusa B (2015). Assessing the quality of life of children with sickle cell anaemia using self-, parent-proxy, and health care professional-proxy reports. British Journal of Health Psychology 20(2):290-304. |
|
|
Cooper O, McBain H, Tangayi S, Telfer P, Tsitsikas D, Yardumian A, Mulligan K (2019). Psychometric analysis of the adult sickle cell quality of life measurement information system (ACSQ-Me) in a UK population. Health and quality of life outcomes 17(1):1-11. |
|
|
Dale JC, Cochran CJ, Roy L, Jernigan E, Buchanan GR (2011). Health-related quality of life in children and adolescents with sickle cell disease. Journal of Pediatric Health Care 25(4):208-215. |
|
|
Driss A, Asare KO, Hibbert JM, Gee BE, Adamkiewicz TV, Stiles JK (2009). Sickle Cell Disease in the Post Genomic Era: A Monogenic Disease with a Polygenic Phenotype. Genomics Insights 2:23-48. |
|
|
Esham KS, RoddayAM, SmithHP, NoubaryF, Weidner RA, Buchsbaum RJ, Parsons SK (2020). Assessment of health-related quality of life among adults hospitalized with sickle cell disease vaso-occlusive crisis. Blood Advances 4(1):19-27. |
|
|
Ezenwa M, Yao Y, Molokie R, Wang Z, Suarez M, Zhao Z, Carasco J, Angulo V, Shuey D, Roach K, Oraifo G, Wilke D (2016). The association of sickle cell-related stigma with physical and emotional symptoms in patients with sickle cell pain. Journal of Pain 17(S15). |
|
|
Faremi FA, Oyeninhun AO (2020). Quality of life of adolescents living with sickle cell anaemia in Ondo State, Nigeria. Pan African Medical Journal 35:124. |
|
|
Fernandes TA, Medeiros TM, Alves JJ, Bezerra CM, Fernandes JV, Serafim ÉS, Fernandes MZ, Sonati M (2015). Socioeconomic and demographic characteristics of sickle cell disease patients from a low-income region of northeastern Brazil. Revista Brasileira de Hematologia E Hemoterapia 37(3):172-177. |
|
|
Garra G, Singer AJ, Taira BR, Chohan J, Cardoz H, Chisena E, ThodeJr HC (2010). Validation of the Wong-Baker FACES Pain Rating Scale in Pediatric Emergency Department Patients. Academic Emergency Medicine 17(1):50-54. |
|
|
Gladwin MT, Sachdev V (2012). Cardiovascular abnormalities in sickle cell disease. Journal of the American College of Cardiology 59(13):1123-1133. |
|
|
Isoa EM (2009). Current trends in the management of sickle cell disease: an overview. Benin Journal of Postgraduate Medicine 11(1):50-64. |
|
|
Jaffer DE, Amrallah FK, Ali KM, Mohammed NA, Hasan RA, Humood ZM (2009). Adult sickle cell diseased patients' knowledge and attitude toward the preventive measures of sickle cell disease crisis. International Journal of Nursing and midwifery 1(2):010-018. |
|
|
Jenerette CM, Brewer C (2010). Health-related stigma in young adults with sickle cell disease. Journal of the National Medical Association 102(11):1050-1055. |
|
|
Locke AB, Kirst N, Shultz CG (2015). Diagnosis and management of generalized anxiety disorder and panic disorder in adults. American Family Physician 91(9):617-624. |
|
|
Nasimuzzaman M, Malik P (2019). Role of the coagulation system in the pathogenesis of sickle cell disease. Blood Advances 3(20): 3170-3180. |
|
|
Nwagha T, Omotowo BI (2020). Determinants of Psychosocial Health-related Quality of Life of Adults with Sickle Cell Disease in a Nigerian Setting. Nigerian Medical Journal: Journal of the Nigeria Medical Association 61(3):114. |
|
|
Nwogoh B, Ofovwe C, Omoti C (2016). Health-related quality of life in sickle cell disease subjects in Benin City, Nigeria. African Journal of Medical and Health Sciences 15(2):80. |
|
|
Ojelabi AO, Bamgboye AE, Ling J (2019). Preference-based measure of health-related quality of life and its determinants in sickle cell disease in Nigeria. PLoS ONE 14(11):e0223043. |
|
|
Oshikoya KA, Edun B, Oreagba IA (2015). Acute pain management in children with sickle cell anaemia during emergency admission to a teaching hospital in Lagos, Nigeria. South African Journal of Child Health 9(4):119-123. |
|
|
Piccin A, Murphy C, Eakins E, Rondinelli MB, Daves M, Vecchiato C, Wolf D, Mc Mahon C, Smith OP (2019). Insight into the complex pathophysiology of sickle cell anaemia and possible treatment. European Journal of Haematology 102(4):319-330. |
|
|
Quinn CT (2016). Minireview: Clinical severity in sickle cell disease: the challenges of definition and prognostication. Experimental Biology and Medicine 241(7):679-688. |
|
|
Rizio AA, Bhor M, Lin X, McCausland KL, White MK, Paulose J, Nandal S, Halloway RI, Bronte-Hall L (2020). The relationship between frequency and severity of vaso-occlusive crises and health-related quality of life and work productivity in adults with sickle cell disease. Quality of Life Research 29(6):1533-1547. |
|
|
Sil S, Cohen LL, Dampier C (2016). Psychosocial and functional outcomes in youth with chronic sickle cell pain. Clinical Journal of Pain 32(6):527-533. |
|
|
Valrie C, Floyd A, Sisler I, Redding-Lallinger R, Fuh B (2020). Depression and Anxiety as Moderators of the Pain-Social Functioning Relationship in Youth with Sickle Cell Disease. Journal of Pain Research 13:729-736. |
|
|
Williams H, Tanabe P (2016). Sickle Cell Disease: A Review of Nonpharmacological Approaches for Pain. Journal of Pain Symptom Management 51:163-177. |
|
|
Williams TN (2016). Sickle Cell Disease in Sub-Saharan Africa. Hematology/Oncology Clinics 30(2):343-358. |
|
|
Wonkam A, Chimusa ER, Mnika K, Pule GD, Ngo Bitoungui VJ, Mulder N, Shriner D, RotimiCN, Adeyemo A (2020). Genetic modifiers of long-term survival in sickle cell anemia. Clinical and Translational medicine 10(4):e152. |
|
|
World Health Organization (WHO) Quality of Life Group (1996). WHOQOL-BREF introduction, administration, scoring and generic version of assessment. Field Trial Version, pp. 1-18. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


