Full Length Research Paper

ABSTRACT
There are very few reports focusing on a role of vitamin D in falls and the related factors in the non-elderly (18-64 years). A cross-sectional survey was addressed to investigate associations between falls, the related factors, and 25[OH]D3 status in 256 non-elderly adults that regularly work indoors at latitude 40° north region. The mean value of the serum 25[OH]D3 was 15.6 ± 7.0 ng/ml. We divided the serum 25[OH]D3 levels into 3 groups. The deficient, inadequate, and adequate group was at a level of <12.0, 12.0 to < 20, and ≧ 20 ng/ml. Percentage of each group was 35, 38, and 27%. Therefore, 73% of the 256 non-elderly adults working indoors did not have adequate serum 25[OH] D3. Falls prevalence of the past 12 months was 8.9, 5.1 and 11.8%, respectively. The mean age of the 3 groups was 37.2 ± 12.5, 39.7 ± 13.2, and 42.0 ± 13.4 years, and it was significantly older in the adequate group (p<0.01). No associations were found in the prevalence of falls, spinal alignment, bone, muscle status, laboratory data among the 3 groups. Therefore, assessment of Vitamin D status in the non-elderly adults may be less valuable as far as falls and the related factors were concerned.
Key words: 25[OH]D3, falls prevalence, non-elderly indoor workers, 40° north latitude.
INTRODUCTION
Vitamin D or cholecalciferol is a collective structure related to metabolites obtained from dietary foods, supplements and sunlight. It regulates calcium and phosphorus levels in the blood by promoting their absorption from the intestine, and also stimulates bone formation and mineralization. The importance of Vitamin D is well recognized in the skeleton. 25-hydroxyvitamin D (25[OH]D) is a stable form of Vitamin D metabolized in the liver, and it sharply reflects the nutritional status of Vitamin D. Lack of 25[OH]D easily leads to osteopenia or osteoporosis because of secondary hyperparathyroidism which induces increasing flow-out of calcium from the bone tissue. Recently, lots of new functional aspects of 25[OH]D in the human body are being investigated. Moreover, several potential links between lack of 25[OH]D and general health problems are also proposed, though they are not conclusive. Vitamin D also works as a kind of essential hormone to maintain normal muscle function in vitro. Vitamin D receptors (VDR) are expressed in the muscle tissue of the entire human body. The action of vitamin D is affected by allelic variance of the VDR. The main action is directly mediated through 1,25(OH)2D3 binding VDR in skeletal muscle tissue. Hamilton has summarized both the genomic and non-genomic function of vitamin D in a review article. 1,25(OH)2D3 binding VDR rapidly regulates membrane calcium channels in the skeletal muscle cells as a non-genetic function. Meanwhile, the binding of 1,25(OH)2D3 to VDR results in enhanced protein transcription in the skeletal muscle cells as a genomic function (Hamilton, 2010).
In clinical cases, lack of 25[OH]D has a possibility to result in myopathy, sarcopenia, neurological impairment, and secondarily limits physical performance (Kulie et al., 2009; Hamilton 2010). It has already been demonstrated that 25[OH]D plays a key role to prevent falls directly or indirectly in the elderly(≧65 years old), but the mechanism is still controversial. Falls are serious events in elderly populations, and even minor falls lead to hip, vertebral fracture, and spinal cord injury which finally lead to dysused syndrome or mortality. The proportion of elderly cases has been increasing in our globe. Out of all the advanced countries, Japan, in terms of the aging society phenomenon, is at the center of this problem. The number of people over 65 years is rapidly increasing and estimated to rise to 32.8% by 2035; even though the total population of Japan is going to naturally decrease (Yoshimura et al., 2009; Cabinet Office Government of Japan, 2019). This is an unsurprising data, and one must be confronted. Undoubtedly, the current situation of Japan is bound to develop in other countries including Africa, where the numbers of young populations are still increasing nowadays, in the near future. Therefore, prevention of falls is considerably crucial to establish well-being and lessen medical costs in aging societies (Brainsky et al., 1997; Krueger et al., 2013). Influence of low serum 25[OH]D on individual health is a serious concern in developed western countries. In the United States, NIH, World Health Organization, Institute of Medicine, Centre for Disease Control and other organizations have suggested variable kinds of risks caused by lack of Vitamin D. Especially, NIH has clearly proposed a guideline for the serum 25[OH] for bone and overall health, but it is still debatable (National Institute of Health, 2019).
Some epidemiological reports have already shown the significance of Vitamin D to maintain physical performances and prevent falls in the elderly population. Pfeifer et al. (2001) demonstrated that serum 25[OH]D had a negative correlation with trunk sway and fall incidence in 237 postmenopausal women. Bischoff-Ferrari et al. (2004a) demonstrated that lower 25[OH]D concentration (< 40 nml/L) are associated with weaker lower-extremity functions in both active and inactive persons aged 60 years and above. Menant et al. (2012) also disclosed that the lower serum 25[OH]D was associated with an increased risk of falls in elderly men (aged 70-90 years). Shimizu et al. (2015) also concluded that the lower serum 25[OH] D, cut-off level < 20 ng/mL, was associated with an increased risk of falls among 1,393 community-dwelling elderly women aged 75 years or older. But, there still remains a question whether it plays the same function in the non-elderly (18-64 years) who are normally not associated with spinal deformity, osteoporosis, and/or sarcopenia. If 25[OH]D has the same function for falls and the related factors in the non-elderly, it is very beneficial to keep serum 25[OH]D concentrations in their normal range before they turn 65 years old or more. To our knowledge, very few systemic studies have been done to investigate relationships between falls, global spinal alignment, bone, muscle, and 25[OH]D status in the non-elderly. To address this question, the current study was introduced in the same sunlight exposure setting. The aim of the current survey is to investigate whether there are associations between falls, the related factors, and 25[OH]D status in non-elderly populations who regularly work indoors at a latitude of 40° North in Japan.
SUBJECTS AND METHODS
Workers employed in an indoor medical equipment factory in Odate were considered candidates. Odate is geographically located at approximately 40° north latitude, and 140° East longitude in Japan, and is one of the cities that annually has the shortest time of solar exposure in Japan. It has been estimated at approximately 1526.0 h per year (1981-2010) (Japan Meteorological Agency, 2019). The total number of workers in the medical equipment factory was 1,489. A questionnaire was delivered, and was collected from 1,452 out of 1,489 workers (collection rate: 97.5%). Age, gender, body height, and weight were ascertained in the questionnaire. Experience of falls in the past 12 months was ascertained as well. Definition of falls was ‘an unintentional change in position resulting in coming to rest at a lower level or on the ground’ (Shimizu et al., 2015). The forty-eight individuals who had not completed the full items in the questionnaire were excluded. Therefore, 1,404 employees were considered participants. Out of the 1,404 workers, 310 were randomly selected for further assessment. The past history of 310 participants was taken by direct interview. Physical conditions including the lumbar spine, hips, knees, and ankle joints were checked by 3 independent orthopedic doctors after the initial interview. A cross sectional study about falls, spinal alignment, bone, skeletal muscle status, and laboratory data including serum concentration of 25 [OH]D was carried out. Twenty-five participants taking drugs that might negatively affect the nerve system were excluded. No one had supplementation of Vitamin D and/or calcium. Twenty-three participants with past histories of cranial, spinal diseases, major joint disorders of the lower extremities, and diabetes mellitus were also excluded.
Three individuals who had not accurately completed items about falls and their past history were also excluded at this point. Three participants who could not complete the following test were also excluded. Finally, 256 of 310 participants were enrolled in the final analysis (Figure1).

Assessment of spinal alignment, bone, and muscle
To evaluate spinal coronal and sagittal balance of the spine, C7-central sacral ventral line (C7-CSVL) and C7 sagittal vertical axis (C7-SVA) were measured on the radiograms of the total spine (Thawrani et al., 2013; Schwab et al., 2012). The radiograms were taken in neutrally standing position with the arms resting on the chest. Measurement of C7-CSVL and C7-SVA were done by 3 radiographers, and the mean value was used for the evaluation. Body mass index (BMI, kg/m2) was calculated by dividing their weight in kilograms by the square of their height in metres. Bone mineral density of the whole body (BMD, g/cm2), and skeletal muscle index (SMI: [arm muscle mass + leg muscle mass] / body height squared, kg/m2) were simultaneously measured using Dual Energy X-ray Absorptiometry (Hologic DISCOVERY A, Bedford, MA).
Biochemical assessment
Blood samples were collected in a non-fasting state and in a sitting position. Serum calcium, phosphorus, albumin were analysed by a fully automated biochemistry analyser (TBA 120FR®, Canon, Tokyo) using commercially available kits. HgA1C was analysed by high performance liquid chromatography. To evaluate metabolic status of the bone, type I procollagen N-terminal propeptide, (total P1NP), and type I collagen cross-linked N-telopeptide (NTx) were measured with electro chemiluminescent immunoassay and enzyme immunoassay, respectively. Blood samples for 25[OH]D (25[OH]D2, 25[OH]D3) were temporarily stored at –20°C, and measured by liquid chromatography-mass spectrometry/mass spectrometry method with an RIT 2 kit® (Dia Sorin, Stillwater, MN, USA). The RIT 2 method is based on an antibody specific to 25[OH] D (the CV was <1%).
Statistical analysis
Associations between 25[OH]D3 concentrations and all investigated items were statistically analysed (cut off , P<0.05). The one-way ANOVA test for ordinal data, and the chi-square test for nominal data were used. All analysis was performed by the Statistical Package for Bioscience (SPBSware Ver 9.6®) (Murata and Yano, 2002).
RESULTS
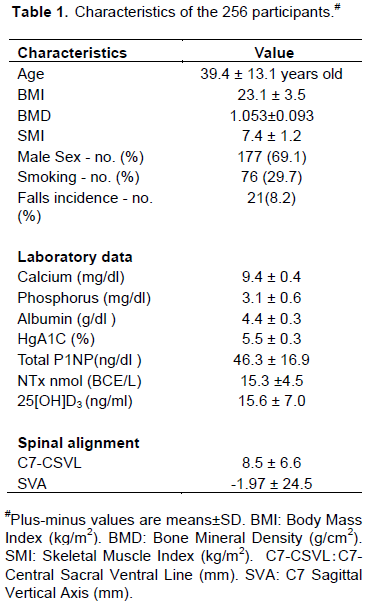
The basic characteristics of the 256 participants are shown in Table 1. In fall incidence, 8.2% of participants (21/ 256) experienced it at least once over the previous year.
Subgroup analysis according to serum 25[OH]D3
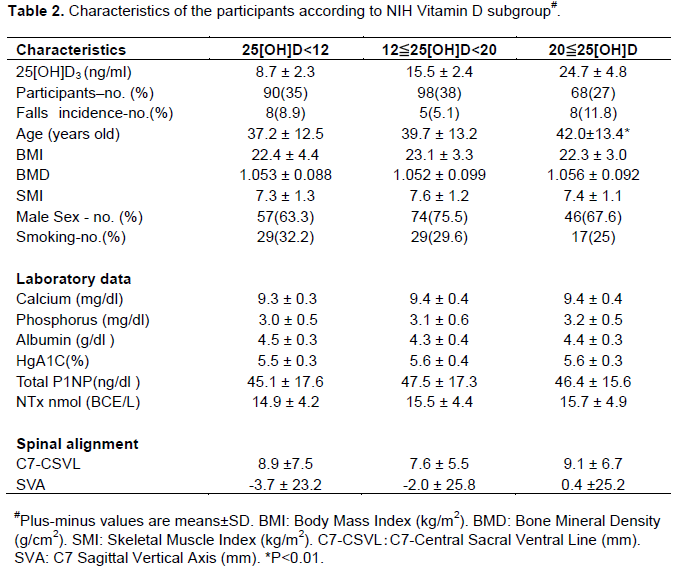
We summarized the serum 25[OH]D3 levels of these subjects into 3 groups according to NIH proposal (National Institute of Health, 2019). The deficient group was defined as a level of <12.0 ng/ml (30 nmol/L). The inadequate group was defined as a level of 12.0 ng/ml (30 nmol/L) to < 20 ng/ml (50 nmo/Ll). The adequate group was defined as a level of ≧20 ng/ml (50 nmo/Ll). The mean 25[OH]D3 of each group was 8.7 ± 2.3, 15.5 ± 2.4, and 24.7 ± 4.8 ng/ml. Percentages of the participants categorized as deficient, inadequate, and adequate groups were 35% (90/256), 38% (98/256), and 27% (68/256), respectively. The mean age in the adequate group was significantly older than the deficient and inadequate groups (p<0.01). As a total result, there were no statistical differences found in the prevalence of falls, all evaluated items of spinal alignment, bone, muscle status, and biochemical assessment among the 3 groups (Table 2).
DISCUSSION
Falls are regulated by various intrinsic and extrinsic factors. As for the intrinsic factors, central and peripheral nerve system, visual, vestibular organs, skeletal tissues, global spinal alignment (Imagama et al., 2013) and so forth are interacting in a complex form to prevent falls in the human body. Skeletal muscle function is considered as one of the important intrinsic factors that affect falls. Miyakoshi et al. (2010) has demonstrated that a vitamin D analog (alfacalcidal) had an effect of strengthening muscle tonus as well as bone mineral density in glucocorticoid-treated rat. Furthermore, Endo et al. (2003) have demonstrated that normal differentiation of the myocytes was not observed in VDR knockout mice, and as a result, a formation of the small myocytes was observed. When the function of Vitamin D in the experimental models in vitro is positively supported, it is presumed that the influence of Vitamin D would be very crucial to prevent falls and keep the physical performance well in vivo. It is generally recognized that muscle volume and strength is negatively associated with aging. It is reported that muscle strength declined from people with ages <40 years to those >40 years between 16.6 and 40.9% in participants with healthy legs (Keller and Engelhardt, 2013). Moreover, aging was significantly associated with decreased VDR expression, independent of biopsy location and serum 25[OH]D levels in human body (Bischoff-Ferrari et al., 2004b).
The current study was performed in non-elderly adults (18-64 years.) with the mean age of 39.4 ± 13.1 years., and has demonstrated that no significant difference was found in fall prevalence, SMI, and other parameters among deficient serum 25[OH]D3 [<12.0 ng/ml (30 nmol/L)], inadequate serum 25[OH]D3 [ 12.0 ng/ml (30 nmol/L) to < 20 ng/ml (50 nmo/Ll)] and adequate serum 25[OH]D3 [≧ 20 ng/ml (50 nmo/Ll)] groups. The current results are completely opposed to the established conclusions of elderly populations. It is speculated that the participants with deficient and inadequate serum 25[OH]D3 still have enough muscle volume and balanced spinal alignment to compensate for a low level of serum 25[OH]D status, and as a result, the participants do not easily fall down as the elderly do. Does the status of low serum 25[OH]D (<20 ng/ml (50 nmo/Ll) still remain in subclinical or insignificant conditions in the non-elderly? The current result is pretty controversial. Body gravity sway velocity is negatively associated with the level of serum 25[OH]D in the elderly (Pfeifer et al., 2001). If body gravity sway is analysed in all participants, similar findings with the elderly might be disclosed. Further biomechanical research is very crucial. The quality of muscle fibers is remarkably different between the non-elderly and the elderly, and it was suggested that age-related reductions in specific strength and power indicated that muscle mass volume alone could not account for the loss of strength and power in the elderly (McNeil et al., 2007). Decrease of muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size, and is unlikely accompanied by substantial muscle fiber loss as well (Nilwik et al., 2013). Also, it could not be denied that rich VDR expression in the muscle tissue still compensates for low serum 25[OH]D status in the non-elderly. It was demonstrated that pathologic mineralization defects of iliac bone occurred in 675 individuals (with 401 males (mean age 58.72 ± 16.99 years), and 274 females (mean age: 68.26 ± 17.27 years)) with a serum 25[OH]D below 75 nmol/L (Priemel et al., 2010). The results have suggested a lower 25[OH]D have some subclinical influence for skeletal health. There is no data whether the participants with low serum 25[OH]D3 below 20 ng/ml (50 nmo/Ll) are destined to fall down easily and become frail several decades later, but there is a possibility that a similar pathologic change is already present in the muscle tissue of the participants of which a serum 25[OH]D is less than 12 or 20 ng/ml despite the normal spinal alignment, BMD and/or SMI. Further discussion and consensus based on the non-biased epidemiological and scientific research are very important.
The current survey was performed in a non-elderly population with the mean age of 39.4 ± 13.1 years in a city at 40° north latitude. The mean value of the serum 25[OH] D3 was 15.6 ± 7.0 ng/ml. It is defined as being ‘inadequate’ according to the NIH proposal. If a cutoff value of 20 ng/mL (50 nmol/L) is adopted, 73% of the participants (188/256) are categorized into the insufficient status of serum 25[OH]D. The mean age of the participants (42.0 ± 13.4 years) in the adequate 25[OH]D3 group was significantly older than of those (37.0 ± 12.5, 39.7 ± 13.2 years) in the deficient and the inadequate 25[OH]D3 group (p<0.01). The result of this current survey does not match previous reports which demonstrated that Vitamin D status was negatively correlated with aging, but it is very similar to the result of a cross sectional study of 77 young, healthy women, aged 19 - 66 years in Japan. According to the report, the mean serum 25(OH)D in women younger than 30 years old was 34.0 ± 11.0 nmol/L and significantly lower than that in women 30 years old and older (50.0 ± 14.4 nmol/L), and the proportion of subjects younger than 30 years old who had serum 25(OH)D less than 30 nmol/L was 42.1%, and was significantly higher than the proportion of those 30 years old and older (10.3%) (p < 0.001). The author has speculated that low fish intake, peculiar dieting, and less outdoor activity are the main reasons of lower serum 25(OH)D in young, healthy Japanese women (Nakamura et al., 2001). Another cross-sectional study showed a high prevalence of Vitamin D insufficiency and deficiency in Rossian adults and adolescent population and an association of low serum 25[OH]D level with female gender, obesity and a low fish diet (Karonova et al., 2016). In a study of health black African adults in Nairobi, the proportion of participants who had a 25(OH) D level of < 20 ng/ml was 17.4% (95% C.I 12.73–22.07), and sunshine exposure for ≥3 h per day reduced the odds of being Vitamin D deficient though this was not statistically significant after multivariate regression analysis (Kagotho et al., 2018). In a survey of African immigrants in Austria, a total of 36% of adults were Vitamin D deficient (35% of men, 37% of women), and the prevalence ratio (PR) of vitamin D deficiency decreased by 2% per year of age (PR 0.98; 95% CI (0.97, 0.99); p = 0.004) and was 1.6 times higher in those with low/sedentary, compared to moderate/high, physical activity levels (PR 1.64; 95% CI (1.12, 2.39); p = 0.011) (Horton-French et al., 2019). The Japan Meteorological Agency reported that Odate has the shortest sunlight duration in Japan (1526.0 h per year in 2010) (Japan Meteorological Agency, 2019). The less sunlight exposure in the indoor working field might negatively affect production of 25[OH]D3 in the non-elderly.
It has been have reported that 90% of Japanese and Korean populations have serum 25[OH]D concentrations below 30 ng/mL (75 nmol/L) of which this level is defined as a threshold level for falls (Dawson-Hughes et al., 2010). If a cutoff value of 30 ng/mL (75 nmol/L) is adapted for fall risk in the non-elderly as well, 98ï¼… of the participants (251/256) in the current survey would be categorized into the high risk group for falls. In the current survey, totally, 8.2 % of participants (21/256) have experienced falls over the previous year. Asian populations easily fall down in comparison to Caucasians. Aoyagi et al. (1998) reported that the proportion of falls in the previous year after age standardization for Japanese (65 years and over) was about twice as high for Caucasians. But it is pretty controversial that the 25[OH]D guideline for falls mentioned above are also pragmatic for the non-eldery population without osteoporosis and/or sarcopenia. There is a possibility of ethnic and age-related difference in Vitamin D status. It is more beneficial that a racial and age-related difference of serum 25[OH]D status should be reconsidered to establish the consensus for fall prevention in whole–spectrum populations (Norris and Williams, 2013; Powe et al., 2013). In regards to the supplementation of Vitamin D, the validity is much more controversial. Broe et al. (2007) reported that a dose of vitamin D (800 IU/day) supplementation dramatically reduced the risk of falls of nursing home residents. Pfeifer et al. (2001) strongly argued that in conjunction with a sufficient calcium intake, the dose of vitamin D supplementation should ensure that circulating levels of 25[OH]D reach this minimum threshold (75 or 30 ng/mL) to maintain skeletal health. Whereas, there is a report that proves no efficacy of the vitamin D supplementation, a high-dose bolus vitamin D supplementation of 100,000 IU colecalciferol monthly over 2.5 - 4.2 years did not prevent falls or fractures in this healthy, ambulatory, adult population (Khaw et al., 2017). As far as fall risk is concerned, is it really necessary for non-elderly, healthy individuals to mandatorily check Vitamin D status and take the Vitamin D supplementation when they have low serum 25[OH]D below 30 ng/mL (75 nmol/L)? Further research is also needed to ascertain the effects of daily Vitamin D dosing with or without calcium for fall prevention.
LIMITATIONS
First, the survey was done for a duration of 1 year due to limited capacity of our institute to evaluate 256 participants. Therefore, it could not be denied that a seasonal change of 25[OH]D3 concentrations affect fall incidence and the related factors (Cinar et al., 2014). Second, bias or inaccuracy about recall of falls in the previous year of the participants, could not be completely excluded through the current interview technique although the interviewers had had no information of the 25[OH]D3 status of the participants before the interview (Coughlin, 1990). Uncertainty of the definition about falls should also be acknowledged. Third, the survey is absolutely cross-sectional. There is no data in regard to the period of the deficient, inadequate serum 25[OH]D3 or adequate serum 25[OH]D3 status of the participants in the past and future. A longitudinal influence of lower serum 25[OH]D3 could not be discussed from the viewpoint of the current results.
ETHICS
This survey was approved by the Ethics Committee of our institute on 7 August, 2015 according to the 1964 Helsinki Declaration. The approval number was 32 in our institute. All patients were asked to give their consent to participate in the current survey. On completion, the survey team will submit the current results for publication in a peer-reviewed scientific journal.
FUNDING
This survey was financially supported as a dissemination project related to the occupational injuries and illness by the Japanese Labour, Health and Welfare Organization in 2015-2017.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate the invaluable contributions made by the staff related to the current survey.
REFERENCES
|
Aoyagi K, Ross PD, Davis JW, Hayashi T, Wasnich RD, Hayashi T, Takemoto T (1998). Falls among community-dwelling elderly in Japan. Journal of Bone and Mineral Research 13(9):1468-1474. |
|
|
Bischoff-Ferrari HA, Borchers M, Gudat F, Dürmüller U, Stähelin HB, Dick W (2004a). Vitamin D receptor expression in human muscle tissue decreases with age. Journal of Bone and Mineral Research 19(2):265-269. |
|
|
Bischoff-Ferrari HA, Dietrich T, Orav EJ, Hu FB, Zhang Y, Karlson EW, Dawson-Hughes B (2004b). Higher 25-hydroxyvitamin D concentration are associated with better lower-extremity function in both active and inactive persons aged>or = 60 y. The American Journal of Clinical Nutrition 80(3):752-758. |
|
|
Brainsky A, Glick H, Lydick E, Epstein R, Fox KM, Hawkes W, Kashner TM, Zimmerman SI, Magaziner J (1997). The economic cost of hip fractures in community-dwelling older adults: a prospective study. Journal of American Geriatric Society 45(3):281-287. |
|
|
Broe EK, Chen TC, Weinberg J, Bischoff-Ferrari HA, Holick MF, Kiel DP (2007). A higher dose of vitamin D reduces the risk of falls in nursing home residents: a randomized, multipleâ€dose study. Journal of American Geriatric Society 55(2):234-239. |
|
|
Cinar N, Harmanci A, Yildiz BO, Bayraktar M (2014). Vitamin D status and seasonal changes in plasma concentrations of 25-hydroxyvitamin D in office workers in Ankara, Turkey. European Journal of Internal Medicine 25(2):197-201. |
|
|
Japan Meteorological Agency (2019). Climate of Japan. Tokyo: Japan Meteorological Agency, (http://www.jma-net.go.jp/akita/Q&A/qanda2-1.htm) accessed November 29th 2019. |
|
|
Coughlin SS (1990). Recall bias in epidemiologic studies. Journal of Clinical Epidemiology 43(1):87-91. |
|
|
Dawson-Hughes B, Mithal A, Bonjour JP, Boonen S, Burckhardt P, Fuleihan GE, Josse RG, Lips P, Morales-Torres J, Yoshimura N (2010). Vitamin D recommended for older adults. Osteoporosis International 21(7):1151-1154. |
|
|
Endo I, Inoue D, Mitsui T, Akaike M, Yoshizawa T, Kato S, Matsumoto T (2003). Deletion of vitamin D receptor gene in mice results in abnormal skeletal muscle development with deregulated expression of myoregulatory transcription factors. Endocrinology 144(12):5138-5144. |
|
|
Hamilton B (2010). Vitamin D and human skeletal muscle. Scandinavian Journal of Medicine & Science in Sports 20(2):182-190. |
|
|
Horton-French K, Dunlop E, Lucas RM, Pereira G, Black LJ (2019). Prevalence and Predictors of Vitamin D Deficiency among African Immigrants Living in Australia. International Journal of Environmental Research Public Health 16(16):2855. |
|
|
Imagama S, Ito Z, Wakao N, Seki T, Hirano K, Muramoto A, Sakai Y, Matsuyama Y, Hamajima N, Ishiguro N, Hasegawa Y (2013). Influence of spinal sagittal alignment, body balance, muscle strength, and physical ability on falling of middle-aged and elderly males. European Spine Journal 22(6):1346-1356. |
|
|
Kagotho E, Omuse G, Okinda N, Ojwang P (2018). Vitamin D status in healthy black African adults at a tertiary hospital in Nairobi, Kenya: a cross sectional study. BMC Endocrine Disorders 18:70. |
|
|
Karonova T, Andreeva A, Nikitina I, Belyaeva O, Mokhova E, Galkina O, Vasilyeva E, Grineva E (2016). Prevalence of vitamin D deficiency in the north-west region of Russia: a cross-sectional study. The Journal of Steroid Biochemistry and Molecular Biology 164:230-234. |
|
|
Keller K, Engelhardt M (2013). Strength and muscle mass loss with aging process. age and strength loss. Muscle, Ligaments and Tendons Journal 3(4):346-350. |
|
|
Khaw KT, Stewart AW, Waayer D, Lawes CMM, Toop L, Camargo CA Jr, Scragg R (2017). Effect of monthly high-dose vitamin D supplementation on falls and non-vertebral fractures: secondary and post-hoc outcomes from the randomised, double-blind, placebo-controlled ViDA trial. The Lancet Diabetes and Endocrinology 5(6):438-456. |
|
|
Krueger H, Noonan VK, Trenaman LM, Joshi P, Rivers CS (2013). The economic burden of traumatic spinal cord injury in Canada. Chronic Diseases and Injuries in Canada 33(3):113-122. |
|
|
Kulie T, Groff A, Redmer J, Hounshell J, Schrager S (2009). Vitamin D. an evidence-based review. Journal of the American Board of Family Medicine 22(6):698-706. |
|
|
McNeil CJ, Vandervoort AA, Rice CL (2007). Peripheral impairments cause a progressive age-related loss of strength and velocity-dependent power in the dorsiflexors. Journal of Applied Physiology 102(5):1962-1968. |
|
|
Menant JC, Close JC, Delbaere K, Sturnieks DL, Trollor J, Sachdev PS, Brodaty H, Lord SR (2012). Relationships between serum vitamin D levels, neuromuscular and neuropsychological function and falls in older men and women. Osteoporosis International 23(3):981-989. |
|
|
Miyakoshi N, Sasaki H, Kasukawa Y, Kamo K, Shimada Y (2010). Effect of a vitamin D analog, alfacalcidol, on bone and skeletal muscle in glucocorticoid-treated rats. Biomedical Research 31(6):329-336. |
|
|
Murata K, Yano E (2002). Medical statistics for evidence-based medicine with SPBS user's guide. Nankodo Publisher, Tokyo. |
|
|
Nakamura K, Nashimoto M, Matsuyama S, Yamamoto M (2001). Low serum 25-hydroxyvitamin D in young adult Japanese women: a cross sectional study. Nutrition 17(11-12):921-925. |
|
|
Nilwik R,  Snijders T, Leenders M, Groen BB, van Kranenburg J, Verdijk LB, van Loon LJ (2013). The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. Experimental Gerontology 48(5):492-498. |
|
|
Norris KC, Williams SF (2013). Race/ethnicity, serum 25-hydroxyvitamin D, and heart disease. Journal of the American Medical Association 310(2):153-155. |
|
|
Pfeifer M, Begerow B, Minne HW, Schlotthauer, T, Pospeschill, M, Scholz M, Lazarescu AD, Pollähne W (2001). Vitamin D status, trunk muscle strength, body sway, falls, and fractures among 237 postmenopausal women with osteoporosis. Experimental and Clinical Endocrinology and Diabetes 109(2):87-97. |
|
|
Powe CE, Evans MK. Wenger J, Zonderman AB, Berg AH, Nalls M, Tamez H, Zhang D, Bhan I, Karumanchi SA, Powe NR, Thadhani R (2013). Vitamin D-binding protein and vitamin D status of black Americans and white Americans. The New England Journal of Medicine 369(21):1991-2000. |
|
|
Priemel M, von Domarus C, Klatte TO, Kessler S, Schlie J, Meier S, Proksch N, Pastor F, Netter C, Streichert T, Püschel K, Amling M (2010). Bone mineralization defects and vitamin D deficiency: histomorphometric analysis of iliac crest bone biopsies and circulating 25â€hydroxyvitamin D in 675 patients. Journal of Bone and Mineral Research 25(2):305-312. |
|
|
Cabinet Office Government of Japan (2019). Situation of aging. Tokyo: Cabinet Office Government of Japan. |
|
|
Schwab F, Ungar B, Blondel B, Buchowski J, Coe J, Deinlein D, DeWald C, Mehdian H, Shaffrey C, Tribus C, Lafage V (2012). Scoliosis research society-Schwab adult spinal deformity classification: a validation study. Spine 37(12):1077-1082. |
|
|
Shimizu Y, Kim H, Yoshida H, Shimada H, Suzuki T (2015). Serum 25-hydroxyvitamin D level and risk of falls in Japanese community-dwelling elderly women: a 1-year follow-up study. Osteoporosis International 26(8):2185-2192. |
|
|
Thawrani D, Agabegi SS, Eismann E, Martin R, Sturm PF (2013). Accuracy and reliability of drawing central sacral vertical line on scoliosis radiographs in clinical practice. Spine Deformity 1(1):16-20. |
|
|
Yoshimura N, Muraki S, Oka H, Mabuchi A, Kinoshita H, Yosihda M, Kawaguchi H, Nakamura K, Akune T (2009). Epidemiology of lumbar osteoporosis and osteoarthritis and their causal relationship - is osteoarthritis a predictor for osteoporosis or vice-versa? : the Miyama study. Osteoporosis International 20(6):999-1008. |
|
|
National institute of Health (2019). Vitamin D - Fact Sheet for Health Professionals. Bethesda: National institute of Health, (https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional) accessed November 29, 2019. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


