Full Length Research Paper

ABSTRACT
Abruptio placentae remain a major cause of maternal morbidity and mortality and a significant cause of perinatal loss especially in the resource poor countries like Nigeria. The objective of this study was to determine the risk factors, maternal and perinatal outcomes of patients managed for abruptio placentae at the University of Abuja Teaching Hospital, (UATH), during a five-year period. A retrospective 5-year review of all cases of abruptio placentae managed at the University of Abuja Teaching Hospital between 2012 and 2016 was carried out. The patients’ case notes were retrieved from the records department of the hospital and studied for socio-demographic characteristics, parity, gestational age, clinical presentation, risk factors for abruptio placentae, foetal and maternal outcomes. Total number of deliveries during the study period was 10767. Fifty-five (0.51%) women had abruptio placentae. Age significantly affected the incidence of abruptio placenta in this study (p=0.001). Parity was not significantly associated with abruptio placenta (p=0.73). Abruptio placentae occurred more frequently amongst unbooked women (70.9%). Maternal complications were postpartum haemorrhage (16.4%), haemorrhage shock (10.9%), postpartum anaemia (acute) (21.8%), and puerperal sepsis (3.6%). There was one maternal death, giving a case fatality rate of 1.8%. Adverse foetal outcome was noted in severe cases of abruptio placentae. There were seven perinatal deaths giving a perinatal mortality rate of 127 per 1000 births. Abruptio placentae is associated with adverse maternal and foetal outcome. Lack of antenatal care, increasing maternal age and multiparity are independently associated with abruptio placentae and this has significant impact on the fetomaternal outcome from the complications. Early diagnosis and prompt treatment of placental abruption will significantly improve foetal and maternal outcome.
Key words: Abruptio placentae, risk factors, maternal, perinatal outcomes.
INTRODUCTION
Abruptio placentae is the premature separation of a normally implanted placenta from the uterine wall after the age of viability but before the foetal delivery resulting in haemorrhage (Kwawukume and Omo-Aghoja, 2015; Momoh and Ebeigbe, 2015; Wagner, 2013; Abasi et al., 2015). It is one of the major causes of obstetric haemorrhage and a common cause of maternal morbidity and mortality globally, especially in the developing countries like Nigeria (Wagner, 2013; Tikkanen, 2011; Adekanle et al., 2011). It is also a significant cause of perinatal loss (Kwawukume and Omo-Aghoja, 2015; Momoh and Ebeigbe, 2015; Wagner, 2013; Abasi et al., 2015; Tikkanen, 2011; Adekanle et al., 2011). Placental abruption may be total or partial, causing pain and vaginal bleeding-which are the hallmarks of placental abruption.
The global incidence of abruptio placentae ranges from 0.38 to 1% of singleton births, and 1 to 2% among twin pregnancies (Ananth et al., 2006; Bohec and Collet, 2010). Perinatal mortality from abruption placentae has been reported from as low as about 1 in 830 (0.12%), to as high as 65% and a fatality rate of up to 3% (Wagner, 2013; Hossain et al., 2010). In Nigeria, the incidence of abruptio placentae ranges between 0.4 and 0.8%.4, 10 It accounted for 3.6% of maternal death in a recent Nigerian nationwide study (Oladapo et al., 2016). Abruptio placentae accounts for 20 to 25% of antepartum haemorrhages and the bleeding may be revealed in 65 to 80% of cases and concealed in 20 to 35% of cases (Tikkanen, 2011; Coleman et al., 2014).
The exact aetiology of abruptio placentae is unknown but a hypothesis suggests placental or vascular abnormalities due to failure of secondary invasion of trophoblastic villi (Kwawukume and Omo-Aghoja, 2015; Wagner, 2013; Abasi et al., 2015). Abnormal placentation, vascular malformations and increased fragility of vessels predispose to haematoma formation resulting in separation of the placenta (Kwawukume and Omo-Aghoja, 2015; Wagner, 2013; Abasi et al., 2015).
Several risk factors have been associated with abruptio placentae including high parity, young or advanced maternal age (<20 years or ≥35 years), low socioeconomic class, cigarette smoking, abdominal trauma, alcohol usage, crack cocaine use in pregnancy, maternal hypertension, preeclampsia, polyhydramnios, premature rupture of membranes, multiple pregnancy, thrombophilias, previous history of caesarean section and prior history of abruptio placentae (Igwegbe et al., 2013; Oladapo et al., 2016; Coleman et al., 2014). The high maternal morbidity and mortality associated with placental abruption is due to severe haemorrhage that follows this complication while the fetal morbidity and mortality is due to reduced placental surface area for oxygenation (Wagner, 2013).
The clinical hallmarks of abruptio placentae include vaginal bleeding, tetanic uterine contractions, uterine hypertonicity, uterine tenderness, irritability, a non-reassuring fetal heart rate pattern or fetal death.10 The diagnosis of abruptio placentae is essentially clinical and may sometimes be difficult as symptoms and signs vary widely (Wagner, 2013; Abbasi et al., 2008). Only one or several of these clinical features may be present and at times the diagnosis may only be made retrospectively when retro-placental blood clots are observed at the delivery of the placenta (Kwawukume and Omo-Aghoja, 2015; Wagner, 2013; Abbasi et al., 2008).
Abruptio placentae have been found to be the most common cause of consumptive coagulopathy in pregnancy (Wagner, 2013; Coleman et al., 2014). Tissue damage, anoxia and shock activate the coagulation system which in turn activates fibrinolysis (Kwawukume and Omo-Aghoja, 2015; Wagner, 2013; Coleman et al., 2014). This results in consumption of platelets and coagulation factors and continuing bleeding causes further depletion of these haemostatic constituents from the circulation (Kwawukume and Omo-Aghoja, 2015; Wagner, 2013; Coleman et al., 2014). The maternal and fetal survival is therefore dependent on early diagnosis and intervention (Kwawukume and Omo-Aghoja, 2015; Wagner, 2013; Abbasi et al., 2008).
The aim of this study was to determine the risk factors, maternal and perinatal outcomes of patients managed for abruptio placentae at the University of Abuja Teaching Hospital, Abuja. It also sought to provide a baseline data of morbidity and mortality about abruptio placentae in University of Abuja Teaching Hospital, Abuja. This will provide recommendation on the management policies that can best minimize the poor maternal and perinatal outcomes within the limits of peculiar constraints.
MATERIALS AND METHODS
This was a five-year retrospective study of all cases of abruptio placentae managed at the Department of Obstetrics and Gynaecology, University of Abuja Teaching Hospital, Abuja, from 1st January, 2012 to 31st December, 2016. This facility is the only teaching hospital in Federal Capital Territory, Abuja, and it serves as the major referral centre within the Federal Capital Territory and its environs.
The data of all patients managed for abruptio placentae within the study period were collected from the labour ward delivery register, theatre records and maternity ward admission register after obtaining clearance from human research and ethical committee. The patients case notes were obtained from the medical records department and studied for the sociodemographics, parity, clinical presentation, risk factors for abruptio placentae, mode of delivery, gestational age at delivery, complications, perinatal and maternal outcome, using a proforma. The data were analyzed using Statistical Package for Social Science (SPSS), IBM SPSS statistics Version 20. Chi-square (c2) was employed to examine the significant association between variables such as age, parity, occupation, booking status, etc. Statistical significance was set at p<0.05. The results are presented as mean with standard deviations and simple percentages.
RESULTS
During the study period, a total of 55 cases of abruptio placentae were managed out of a total delivery of 10767, giving an incidence of 0.51%. The mean age of the patients was 29.14 ± 5.17 years and all were married. Majority [39 (70%)] of the patients were in the age range of 25 to 34 years. Patients in the age range of 20 to 24 years had the same incidence rate of abruptio placentae with those ≥35 years [7 (12.7%)]. Age significantly affected the outcome of abruptio placentae in this study (p=0.001) as shown in Table 1.
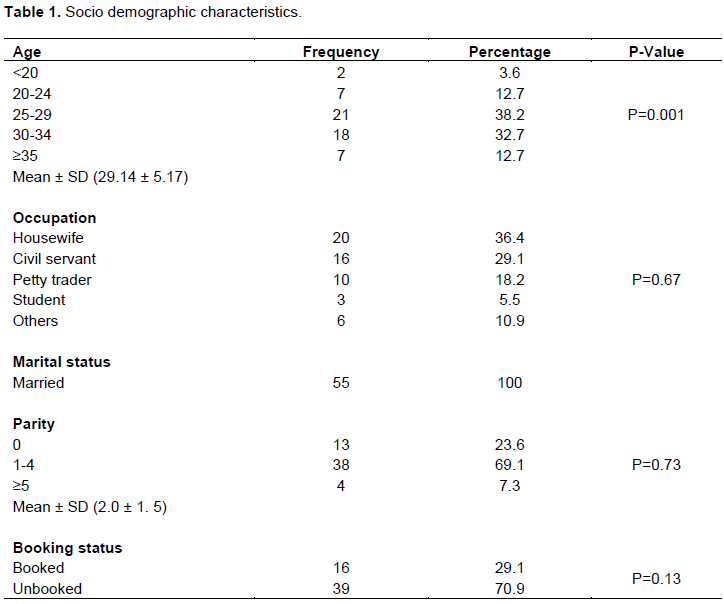
The incidence of abruptio placentae was the highest among housewives 20 (36.4%). Occupation did not significantly affect the incidence of abruptio placentae in this study (p=0.67). The mean parity of the patients was 2.0 ± 1.5. Majority of the women were of parity range 1-4 [38 (69.1%)], nulliparae constituted [13 (23.6%)] and only [4 (7.3%)] were grand multiparae. Abruptio placentae was commoner among unbooked patients [39 (70.9%)], compared to the booked patients [16 (29.1%)] as shown in Table 1.
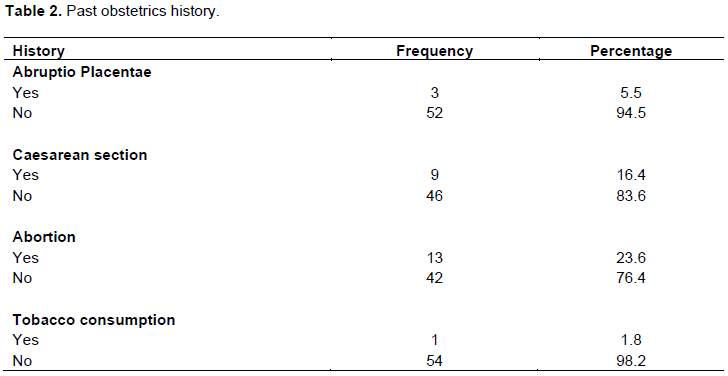
The risk for abruptio placentae was the highest among women with previous history of abortion [13 (23.6%)], followed by those with previous caesarean section [9 (16.4%)]. Prior history of abruptio placentae constituted [3 (5.5%)] risk, while maternal tobacco consumption constituted [1 (1.8%)] risk for placental abruption in this study as shown in Table 2.
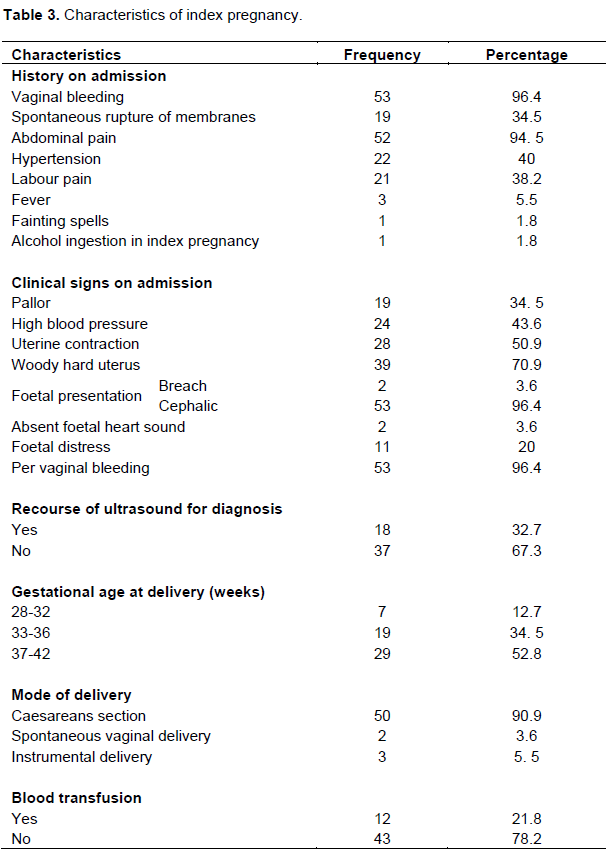
The common presenting complaints were vaginal bleeding [53 (96.4%)], abdominal pain [52 (94.5%)], hypertensive disorder in the index pregnancy [22 (40%)], labour pain [21 (38.2%)] and spontaneous rupture of membranes [19 (34.5%)]. Others were fever 3 (5.5%), fainting spells [1 (1.8%)] and alcohol ingestion in the index pregnancy [1 (1.8%)]. Per vaginal bleeding [53 (96.4%)] was the commonest clinical sign, followed by ‘woody hard’ uterus [39 (70.9%)] and uterine contraction [28 (50.9%)]. Others were raised blood pressure [24 (43.6%)] and pallor [19 (34.5%)]. Fetal presentation was cephalic in 53 (96.4%) of the cases, while 2 (3.6%) presented breech. Fetal distress occurred in 11 (20%) patients, 2 (3.6%) patients had absent fetal heart sounds, while the rest of the patients had normal fetal heart sounds. Majority [48 (86%)] of the patients delivered between 33 and 42 weeks gestation and caesarean section was the commonest mode of delivery [50 (90.9%)]. 2 (3.6%) patients had spontaneous vaginal delivery while 3 (5.5%) had instrumental (vacuum) delivery as shown in Table 3.
The maternal morbidity suffered by patients in this study included postpartum anaemia (acute) [12 (21.8%)], postpartum haemorrhage [9 (16.4%)], haemorrhage shock [6 (10.9%)] and puerperal sepsis [2 (3.6%)]. Six patients (10.9%) were admitted in the intensive care unit. Twenthy patients had no complication. There was one maternal death giving a case fatality rate of 1.8%. The maternal death occurred in an unbooked patient who presented very late to the hospital in irreversible shock having had massive postpartum haemorrhage at home.
The unbooked patients in this study were more compared to booked patients because the hospital serve as a referral centres for the primary health centres and general hospitals in Federal Capital Teritary as shown in Table 4.
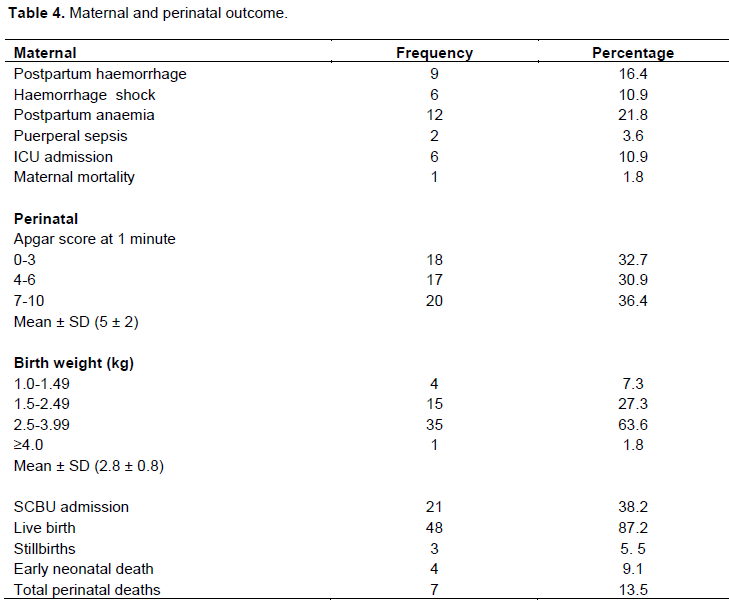
The total birth was 55 and there were 48 (87.2%) live births out of which 18 (32.7%) had severe birth asphyxia while 17 (30.9%) had moderate birth asphyxia. The mean first minute Apgar score was 5 ± 2. Twenty-one (38.2%) babies were admitted in the neonatal intensive care unit. The mean birth weight was 2.8 ± 0.8. Majority 35 (63.6%) of the babies weighed between 2.5 and 3.99 kg. There was one (1.8%) fetal macrosomia. There were seven perinatal deaths (stillbirth + early neonatal death) giving a perinatal mortality rate of 127 per 1000 births. Of the mortalities, three were intrauterine fetal deaths, while four were early neonatal deaths. The causes of death included severe birth asphyxia and prematurity as shown in Table 4.
DISCUSSION
Abruptio placentae is an important cause of maternal and perinatal morbidity and mortality (Wagner, 2013). The severity and duration of abruption are important determinants of the fetal and maternal outcome (Wagner, 2013; Abbasi et al., 2008). The incidence of 0.51% in this study is consistent with both the national and global incidence rates of 0.4 to 0.8% and 0.1 to 0.38%, respectively (Abasi et al., 2015; Ananth et al., 2006; Bohec and Collet, 2010; Igwegbe et al., 2013). It is comparable to reports from Nnewi (0.8%) (Igwegbe et al., 2013) and Bayelsa (1.46%) (Abasi et al., 2015); both in Nigeria, as well as 1.4% reported from Ghana (Igwegbe et al., 2013), but much lower than 3.9 and 4.4% reported from Pakistan and India, respectively (Habibullah and Muhammad, 2010; Mukherjee et al., 2014).
The mean age of patients in this study is comparable to reports of similar studies in Nnewi and Cameroon (Igwegbe et al., 2013; Tebeu et al., 2013). The finding of increased risk of abruptio placentae among women of low income status and those without antenatal care in this study is consistent with reports from previous studies (Abasi et al., 2015; Coleman et al., 2014; Tebeu et al., 2013). Risk of placental abruption in patients with chronic hypertention, prior history of abortion, caesarean section and abruptio placentae, as well as cigarette smoking in the index pregnancy might be increased as shown in this study. This was similar to findings from Nnewi, Ghana, Cameroon and Northern Tanzania (Igwegbe et al., 2013; Coleman et al., 2014; Tebeu et al., 2013; Macheku et al., 2015).
The mean parity of 2.0 ± 1.5 in this study is lower than the finding from Nnewi where a mean parity of 4.1 ± 0.6 was reported (Igwegbe et al., 2013). Parity distribution of 1 to 4 shown in this study is similar to reports from Bayelsa (Nigeria), Ghana and Northern Tanzania (Abasi et al., 2015; Coleman et al., 2015; Abbasi et al., 2008). The mode of presentation is similar to reports from other studies (Abasi et al., 2015; Hossain et al., 2010; Coleman et al., 2014; Tebeu et al., 2013). Although the use of ultrasound shown in this study is lower than 43% reported in Cameroon, it seems quite high as too much reliance on ultrasound for diagnosis of abruption placentae could delay treatment and increase the maternal and foetal complications (Tebeu et al., 2013). Ultrasonographically, abruption may show a variety of appearances depending upon the size, location of bleed and also the time between the abruption and when ultrasonography was performed. Ultrasonographic criteria for diagnosis of placental abruption include preplacental collection under chorionic plate, jello-like movement of chorionic plate with fetal activity, retroplacental collection, marginal haematoma, subchorionic haematoma, increased placental thickiness ˃5 cm and intra-amniotic haematoma.
This study confirmed the findings of previous investigators who reported an increased risk of preterm birth among women with abruptio placentae (Jabeen and Gul, 2011). Emergency Caesarean section rate of 90.9% was higher than the 56, 75.4 and 83%, reported in Bayelsa, Nnewi and Ghana, respectively (Abasi et al., 2015; Igwegbe et al., 2013; Coleman et al., 2014). Caesarean delivery is a better option for women with abruptio placentae with a live fetus as this mode of delivery could reduce the perinatal death rate by 20 to 50% (Bohec and Collet, 2010). Vaginal delivery is the preferred mode of delivery when the fetus is dead and the mother is haemodynamically stable (Kwawukume and Omo-Aghoja, 2015; Momoh and Ebeigbe, 2015; Coleman et al., 2014).
The commonest maternal morbidities noted in this study were postpartum haemorrhage and postpartum anaemia. This is not surprising as both antepartum and postpartum haemorrhages are part of the documented sequelae of abruptio placentae (Kwawukume and Omo-Aghoja, 2015; Momoh and Ebeigbe, 2015; Wagner, 2013; Paterson-Brown, 2012). The frequent occurrence of maternal anaemia in abruptio placentae has been noted in similar studies (Abasi et al., 2015; Tikkanen, 2011; Igwegbe et al., 2013; Coleman et al., 2014; Paterson-Brown, 2012). The case fatality rate of 1.8% found in this study is lower than 2.8, 3.5 and 3.6% reported in Bayelsa, India and Northern Tanzania, respectively, but higher than findings in Europe where case fatality rate was reported to be as low as 0.04% (Abasi et al., 2015; Mukherjee et al., 2014; Macheku et al., 2015; Tikkanen et al., 2009).
The perinatal mortality rate of 127 per 1000 births in this study is lower than reports from Bayelsa (527.7/1000) and Ghana (650/1000).4, 12. In this study, patients with abruptio placentae there were high proportion of babies with low first minute Apgar score, similar to reports from similar studies in Ghana, India, Cameroon and Northern Tanzania (Coleman et al., 2014; Mukherjee et al., 2014; Tebeu et al., 2013; Tikkanen et al., 2009).
CONCLUSION
Abruptio placentae adversely affects foeto-maternal outcome. The risk factors found includes age, parity, previous history of abortion, prior history of caesarean section, previous history of abruption placentae and unbooked patients. There is a need for institutional preparedness, early diagnosis and treatment to prevent foetal and maternal morbidity and mortality.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abasi IJ, Israel J, Ekine AA (2015). Risk factors and pregnancy outcome of placental abruption at the Niger Delta University Teaching Hospital, Okolobiri, South-south Nigeria. British Journal of Medicine and Medical Research 5(8):1000. |
|
|
Abbasi RM, Rizwan N, Mumtaz F, Farooq S (2008). Feto maternal outcome among Abruptio placentae cases at a University hospital of Sindh. JLUMHS 2:106-109. |
|
|
Adekanle DA, Adeyemi AS, Fadero FF (2011). Ante-Partum haemorrhage and pregnancy outcome in LAUTECH teaching hospital, southwestern Nigeria. Journal of Medical Sciences 2(12):1243-1247. |
|
|
Ananth CV, Getahun D, Peltier MR, Smulian JC (2006). Placental abruption in term and preterm gestations: evidence for heterogeneity in clinical pathways. Obstetrics & Gynecology 107(4):785-792. |
|
|
Bohec C, Collet M (2010). May. Abruptio placentae. In Annales francaises d'anesthesie et de reanimation (29 (5):e115-9). |
|
|
Coleman J, Srofenyo EK, Ofori EK, Brakohiapa EK, Antwi WK (2014). Maternal and fetal prognosis in abruptio placentae at Korle-Bu Teaching Hospital, Ghana. African Journal of Reproductive Health 18(4):115-122. |
|
|
Du Toit MM, Smith M, Odendaal HJ (2010). The role of prenatal alcohol exposure in abruptio placentae. South African Medical Journal, 100(12):832-835. |
|
|
Hossain N, Khan N, Sultana SS, Khan N (2010). Abruptio placenta and adverse pregnancy outcome. Hypertension 13:16. |
|
|
Igwegbe AO, Eleje GU, Okpala BC (2013). Management Outcomes of Abruptio Placentae at Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria. Nigerian Journal of Medicine, 22(3):234-238. |
|
|
Jabeen M, Gul F (2011). Abruptio placentae: risk factors and perinatal outcome. Journal of Postgraduate Medical Institute (Peshawar-Pakistan) 18(4). |
|
|
Kwawukume EY, Omo-Aghoja LA (2015). Antepartum Haemorrhage (AP). In: Comprehensive Obstetrics in the Tropics. Kwawukume EY, Ekele BA, Danso KA, Emuveyan EE (Eds) 2nd edition. Ghana: Assemblies of God Literature Centre Ltd. 184-197. |
|
|
Macheku GS, Philemon RN, Oneko O, Mlay PS, Masenga G, Obure J, Mahande MJ (2015). Frequency, risk factors and feto-maternal outcomes of abruptio placentae in Northern Tanzania: a registry-based retrospective cohort study. BMC Pregnancy and Childbirth 15(1):242. |
|
|
Momoh MO, Ebeigbe PN (2015). The Woman with Ante-partum Haemorrhage. In: Foundations of Clinical Obstetrics and Gynaecology in the Tropics. Ebeigbe PN. (Ed). Benin City: Mindex Publishing Company Limited pp. 383-388. |
|
|
Mukherjee S, Bawa AK, Sharma S, Nandanwar YS, Gadam M (2014). Retrospective study of risk factors and maternal and fetal outcome in patients with abruptio placentae. Journal of Natural Science, Biology, and Medicine 5(2):425. |
|
|
Oladapo OT, Adetoro OO, Ekele BA, Chama C, Etuk SJ, Aboyeji AP, Onah HE, Abasiattai AM, Adamu AN, Adegbola O, Adeniran AS (2016). When getting there is not enough: a nationwide crossâ€sectional study of 998 maternal deaths and 1451 nearâ€misses in public tertiary hospitals in a lowâ€income country. BJOG: An International Journal of Obstetrics and Gynaecology 123(6):928-938. |
|
|
Paterson-Brown S (2012).Obstetric Emergencies. In: Dewhurst's Textbook of Obstetrics and Gynaecology for Postgraduate. Edmonds DK. (Ed) 8th edition. London: John Wiley and Sons Ltd. pp. 302-316. |
|
|
Qamarunisa MH, Ali M (2010). Frequency, maternal and fetal outcome of abruptio placenta in a rural Medical College Hospital, Mirpurkhas Sindh. Pakistan Journal of Medical Sciences 26(3):663-666. |
|
|
Tebeu PM, Nnomo JA, Tiyou CK, Obama MTA, Fosso GK, Fomulu JN (2013). The Pattern of Abruption Placenta in Cameroon. Medical Journal of Obstetrics and Gynecology 1(3):1015. |
|
|
Tikkanen M (2011). Placental abruption: epidemiology, risk factors and consequences. Acta obstetricia et gynecologica Scandinavica 90(2):140-149. |
|
|
Tikkanen M, Gissler M, Metsäranta M, Luukkaala T, Hiilesmaa V, Andersson S, Ylikorkala O, Paavonen J, Nuutila M (2009). Maternal deaths in Finland: focus on placental abruption. Acta obstetricia et gynecologica Scandinavica 88(10):1124-1127. |
|
|
Wagner SA (2013). Third trimester vaginal bleeding. Current Obstetrics and Gynaecology Diagnosis and Treatment. 11th ed. USA: Lange Medical Books/McGraw-Hill pp. 310-316. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


