Full Length Research Paper

ABSTRACT
Unskilled Traditional Birth Attendants (TBA) is prevalent in rural Nigeria due to communal culture and traditions, their compassionate attitude, and non-availability of appropriate health facilities within the communities. Yet, there is no clear framework defining their roles, locations and practices. This study aimed to identify the pattern and practices of TBA in Nsukka area of Enugu State, and evaluate their roles in rural maternity services in Enugu state of Nigeria. This was a mixed method cross sectional study involving a questionnaire-based survey and Focus group discussions (FGD). Seventy-eight TBAs, were recruited for this study. Structured interviewer-administered questionnaire was used to collect quantitative data and a semi-structured discussion guide was used for the FGD – one FGD for each development center. SPSS version 25 was used for statistical analysis. Records of FGD sessions were transcribed, condensed into themes, and analyzed. A total of 78 TBAs were interviewed, 26 from each of the three development areas. Majority (66.0%) completed primary education while 9.0% did not have any formal education. Almost two-third (65.4%) uses exclusively traditional methods in their practice, whereas 34.5% combined orthodox method. Three focused group discussions showed almost all the TBAs in the study could neither identify different complications and when to refer nor signs separating different stages of labour. Poorly educated TBA in the Nsukka area of Enugu State combines orthodox medicine with herbs and traditional healing methods. Their appreciation and management of danger pregnancy signs and referral system are lacking.
Key words: Traditional birth attendants, healthcare, Nsukka, informal health, Labor.
INTRODUCTION
Reducing maternal mortality has been a global public health priority in recent years. Various efforts and programs including safe motherhood initiative, millennium development goals and the sustainable development goals (SDG) were conceived to reduce maternal mortality among other aspirations (Starrs, 2006; Theron, 2016).
The sustainable development goal (SDG) 3.1 aims to reduce global maternal mortality ratio (MMR) to less than 70 per 100,000 live births by the year 2030.2It is well known that improving access to antenatal care and availability of skilled attendants at delivery are key approaches for effective reduction in maternal mortality (World Health Organization, 2018; Tunçalp et al., 2015).Due to a combination of reasons including poor physical accessibility to health facilities, economic and cultural factors, poor health-seeking behaviour of the largely uneducated and predominantly rural women and poor understanding of signs of pregnancy complications (Ntoimo et al., 2019; Fagbamigbe et al., 2017),many rural women do not have access to skilled attendants at birth. It has been documented that only about 43% of women in Nigeria have delivery with skilled birth attendants (Ntoimo et al., 2019).
Many of them therefore patronize the readily available and affordable traditional birth attendants (TBA). The TBA initially acquires her skills by delivering babies herself or by working with other TBAs (WHO, 2018). Studies have shown that culture, compassionate attitude of TBAs, non-availability of appropriate health facility and long distance from health facility have made the use of unskilled birth attendants TBA imperative in rural Nigeria (Fagbamigbe et al., 2017; Federal Ministry of Health, 2013; Izugbara and Ukwayi, 2004, 2003). Between 1970 and 1990, WHO promoted and funded training of TBAs as a strategy to reduce maternal and neonatal mortality; however current evidence in support of TBA training is limited but promising for reducing maternal deaths (World Health Organization, 2020). In places where there are unavailability of skilled birth attendants and difficulty in accssing qualitative maternal services, training and re-training of TBAs to incrtease their knowledge of pregnancy and screening capacity for signs of complications during pregnancy can improve referrals and make them more involved positively in maternal health services until the appropriate skilled personnel is available.
The delivery of affordable and quality health interventions especially maternal, newborn and child health depends largely on availability and access to skilled birth attendants. Every day in 2017, about 810 women die globally from causes that could have been prevented during pregnancy (Umeora and Egwuatu, 2010). Of this number, 94% occur in developing countries and the rate is higher in women living in rural areas and poorer communities (Umeora and Egwuatu, 2010; Sibley et al., 2007).More than half of this 94% occur in sub-Saharan Africa (Umeora and Egwuatu, 2010). The maternal, newborn and child health situation in Nigeria is still a public health concern with an estimated annual birth of approximately 6 million (Ntoimo et al., 2019) with infant mortality rate of 69 deaths per 1,000 live births (Ntoimo et al., 2019; World Health Organization, 2010). This rate is a great under estimation of the burden of the problem due to non-availability of epidemiological data from the TBA and other informal healthcare providers that result of complications directly related to pregnancy, labor or puerperium, can be prevented by early recognition, prompt referrals and skilled birth attendance.
Although Nigeria has 43% of deliveries attended to by skilled birth attendants according to the NDHS 2018, the situation in Nsukka Local Government area is still a far cry from normal.15TBA exist within the communities and are patronized by all and sundry, nevertheless, there is no proper documentation of their distribution, organization and practices in Nsukka, Enugu state. Formal recognition and regulation of the activities of TBAs by relevant government authorities have been identified as a possible strategy in addressing the issue of skilled birth attendants since they provide round the clock and emergency services in their strategic locations and can also help to enhance timely referrals (Nbs. Annual Abstract of Statistics, 2010).Although TBA are not the panacea to challenges of skilled birth attendance, when properly guided through capacity building and constant supervision to enable them recognize the limitations in their competencies, they may play crucial roles in bridging the gap in the lack of skilled birth attendants. This study was to identify the pattern and practices of TBAs in Nsukka area of Enugu State and evaluate their role as unavoidable link and participant in the quest for improved rural maternity services in Enugu state of Nigeria.
METHODOLOGY
Study setting
The study area was Nsukka LGA, one of the six LGAs in Enugu North senatorial zone of Enugu State, south-east Nigeria. The LGA comprises thirty-seven communities spread across three development centres created by Enugu State Government. One of these development centres (Nsukka central development center) is largely urban and is home to Nigerian’s first indigenous University, The University of Nigeria, Nsukka and the apex government secondary health facility that serves as the comprehensive emergency obstetric center in the district. The remaining two development centres are of the same socioeconomic level. There are three public secondary health facilities, 23 public primary health facilities, 27 formal private health facilities three of which are owned by faith-based organizations and 24 are owned by private-for-profit organizations. More than 90% of the private health facilities are located in Nsukka central development centre (Federal Ministry of Health of Nigeria, 2009).
Study population and design
This was a mixed-method cross-sectional study of TBAs involving questionnaire survey and Focus Group Discussions (FGD).
Sampling technique
The respondents for the questionnaire were selected using balloting method. Firstly, 13 communities were selected from each of the 3 development centres in Nsukka LGA to make up a total of 39 communities. With the assistance of Chairmen of Ward Development Committees (WDCs), a sample frame of TBAs was generated in the selected 39 communities. The sample frame was used to select 2 TBAs from each of the 39 communities to make up a total of 78 respondents. Among the 78 TBAs selected for questionnaire survey, one per community was nominated by the WDC Chairmen to make up a total of 39 participants for the FGD.
Data collection
Data collection for the survey was carried out using interviewer-administered questionnaire and Focus Group Discussion (FGD) in the months of February 2019 to establish baseline information about the standard of practice, scope of activities, knowledge of maternal and child health and level of training/qualifications of the TBA. The qualitative survey involved three focused group discussion sessions, each comprising 13 participants. The FGD was conducted in Nsukka dialect which is using an FGD guide. The FGD with the TBAs was moderated by members of the research team and centered on the appreciation of maternal deaths and their causes. These discussions were recorded by note-taking and backed-up with audio-recording with an android phone. After each FGD session, the recorded data was immediately transcribed into paper in Central Igbo Language.
Data analysis
Quantitative data was analyzed using SPSS version 25. Qualitative data was analyzed using thematic analysis approach. Firstly, the qualitative data in central Igbo was translated into English Language by an independent trained translator and proof-read by two members of the research team. Preliminary codes were then assigned to the data in order to describe the contents and emerging themes were identified.
Ethical approval was obtained from the Enugu State Primary Health Care Development Agency and the communities were accessed after interactions with, and permission obtained from the various traditional rulers and community leaders. Informed consent was also obtained from each of the participants before they were interviewed.
RESULTS
All 78 questionnaires administered were completed and returned, cleaned and analyzed. Three FGDs were conducted among the respondents who were all TBA; 1 participant per development center, totaling 13 respondents.
Respondents’ profile
Table 1 shows the socio-demographic characteristics of the study participants. All the 78 participants were females. The mean age of the respondents was 48.2 ± 4.3 years while the mean length of practice time is 22.5 ± 3.2 years. Only two of them (who acquired the skills from their late mothers) had never married at the time of the study. The educational qualifications of participants ranged from no formal education (9%), primary school attempt (6%), primary education (66%), Secondary Education (17%), to post-secondary education (2%).
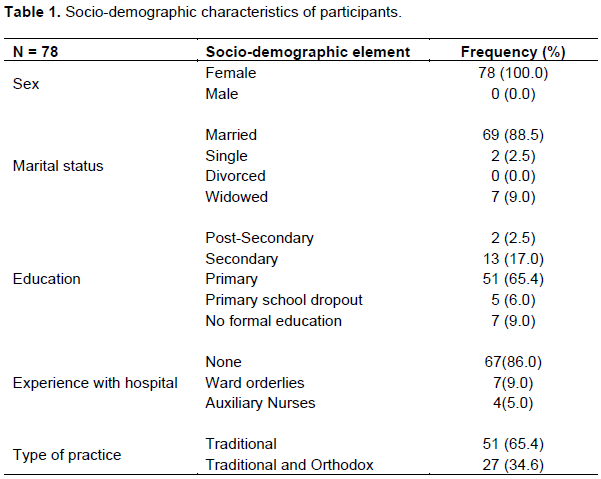
Interestingly, the 78 (100%) TBAs identified themselves as Christians. Their mean length of experience in conducting deliveries was 22.5 ± 3.0 years. Some (9%) of the TBAs had worked as ward orderlies (cleaners, ward officers), while a few (5%) worked as auxiliary nurses in either private health institution or maternity homes before resorting to the use of herbs. These are the ones that combine orthodox and traditional practice.
Formal training
The FGD showed that none of the 39 TBAs involved in the study had received any form of formal training or orientation on basic delivery skills, infection prevention and control practices, management of post-partum hemorrhage, referral and linkages. However, majority of the TBAs were able to identify prolonged labour, retention of placenta and bleeding as complications of labour. About a quarter of them cannot read or write, although they make use of cell phones. This number relies mainly on herbs for conducting delivery and management of labour-related complication. Interestingly, most of the herbs they use come from edible crops, making it highly client friendly. For instance, the leaves of sweet potato are widely used in the management of postpartum hemorrhage.
Pattern of practice
FGD and quantitative data showed that about a third (34.6%) of the TBAs combine both orthodox and traditional methods in their practice. This involved the use of paracetamol, oxytocin and antibiotics in combination with herbal medicine. In addition, a third of the respondents also give mothers herbs during their antenatal care (ANC) visits to reduce the weight of the fetus while more than half of them use herbs to initiate and hasten labour. One of the participants in the FGD had this to say:
“Because we know that when the fetus in the womb is very big it makes delivery more difficult during labour, we give mothers herbs during ANC to reduce the weight of the fetus. We also use herbs to initiate labour when labour fails to starts naturally at nine months”.
While those who had worked in hospital environment administer oxytocin to complement the effect of herbs, majority of the entire respondents give other drugs such as paracetamol. Although they carry out vaginal examination using antiseptic solution, no respondent was able to explain the events or signs separating the different stages of labour. They were also bereft of the knowledge of modern delivery techniques such as squatting or breathing exercise. In addition, although majority of them make use of Sodium hypochlorite, none of them had knowledge of preparation, dilutions and the time required to achieve high level disinfection. Also, mothers are not screened for HIV/AIDS or any other viral disease that can be vertically transmitted.
Referrals and linkages
Furthermore, the FGD showed that there was no coordinated referral system in place, and respondents are not properly aware of referral centres as they would always ask the relatives to carry patient to hospital. Referral was mainly done orally and there was no follow up. There was also no functional transport system to facilitate the referral process. None of the respondents could mention the danger signs of pregnancy. Below is a quote from one of the participants:
“Anytime I am not able to handle a pregnant woman in labour, I ask the relatives to carry her to a hospital”. I usually do this when I observe that it is taking too long for the woman to push out the baby”.
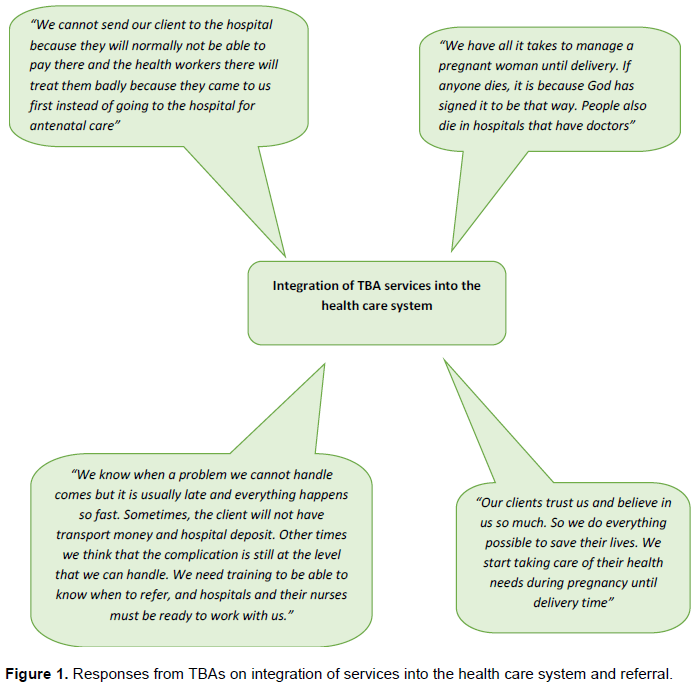
Integration of TBAs into the healthcare system
In an attempt to understand the participants’ scope of practice, only a few (mainly those that have worked in hospitals) understood when there are complications and when to refer. The capacity to understand complications and make the right decision about referral was lacking in most of the TBAs, and even those of them with this ability were limited by lack of a functional integration and referral system with nearby health facilities. While some of the respondents, excitedly showed willingness to be trained to understand delivery-associated complications, and when and how to refer, others were not interested in this level of capacity building; they believed that their practices are exclusively traditional and should not have anything to do with orthodox practice. The TBAs also admitted that the closeness and friendship that exist between them and their clients leaves them trusted by the clients to take care of their health concerns during this time. Most clients believe in them more than they do in health workers. The TBAs also reported poor co-operation with health care workers at the facilities (Figure 1).
DISCUSSION
All participants were females. This was in line with findings in previous studies on TBA in Nigeria in which females predominated (Ofili and Okojie, 2005; Brink et al., 2006) Being all females, they apparently understand the special needs of the woman during antenatal, labour and delivery. None of the TBA involved in the study had received any form of formal training or orientation on basic delivery skills, infection prevention and control practices, management of post-partum hemorrhage or referral linkages which would have made them more useful in preventing maternal mortality by at least noticing early danger signs and referring. This is similar to finding in a study conducted in Edo State, south-south geopolitical zone of Nigeria in which majority of the TBAs (62.2%) acquired their skills through apprenticeship with relation; learning by experience, observation and mentorship from another TBA who they may probably be a related to (Nbs. Annual Abstract of Statistics, 2010). Training for traditional birth attendance is a key intervention for effective maternal care. Training has been found to significantly increase attributes such as knowledge, attitude, behaviour, advice for antenatal care, and pregnancy outcomes (Abeshi et al., 2017).
Majority of the TBAs were able to identify prolonged labour, retention of placenta and bleeding as complications of labour. This is desirous since early identification of these complications are necessary for prompt referral of clients to hospital for skilled birth attendance and management of the complications. However, having this ability, without adequate training on referral and functional system may result in overconfidence in the TBA’s capacity to handle some complications and consequently, lead to loss of lives. Training of TBAs to identify and understand complications and make early referral should be a critical aspect to be considered although, the participants carry out vaginal examination, none of them was able to explain the events or signs separating the different stages of labour. Also, they lacked knowledge of modern delivery techniques such as squatting or breathing exercise. These findings suggest the need to conduct training for the TBAs in order to increase their knowledge and build their capacity for effecting monitoring and identification of the signs of the different stages of labour. This will culminate in good maternal and neonatal outcomes.
Apart from other known reasons why clients choose TBAs such as low cost of service and proximity, the bond and closeness that exist between TBAs and their clients as observed in this study is enormous. Clients have confidence in the TBAs’ ability to handle their health challenges at little or no cost more that they even do the health care professionals at the health centres. The close relationship between TBAs and clients is a programed strength (Glenton et al., 2013), whereas the reported poor co-operation of the health care workers at health facilities is a threat to integrating the unavoidable services of the TBAs.
The changing pattern of practice observed among the TBA in this study in which they combine orthodox medicines with traditional healing methods could be as a result of increasing level of education among TBAs in this setting, especially as 51 (66%) of those sampled completed primary education while 13 (17%) had secondary education. Even though majority of the participants make use of Sodium hypochlorite, none of them has knowledge of preparation, dilutions and the time required to achieve high level disinfection. This may mean that the TBAs know about the need to prevent infections during management of labour but lack detailed knowledge of the standard operating procedures to achieve good results. This also underscores the need for capacity building of the TBA to improve their infection prevention and control practices.
The fact that mothers are not screened for HIV/AIDS or any other viral disease that can be vertically transmitted meant that the TBA do not understand mother to child transmission of HIV and other vertically transmitted diseases or they lack knowledge of referral process for prenatal screening activities at health facilities. This is corroborated by the fact that there was no coordinated referral system in place, and no awareness of referral centres. Referral was mainly done orally and there was no follow up. This is contrary to report about TBAs’ practice in Nepal where almost three-fourths (73%) of them stated that they would refer their clients to a clinic (Ribeiro, 2014). There was no functional transport system to facilitate the referral process. In a study done in Ghana, TBAs did not only arrange means of transport but also accompanied women in labour to health facilities (Adatara et al., 2018).
CONCLUSION
There seems to exist a new trend of poorly educated TBAs who combine orthodox medicine and traditional herbs and healing methods in Nsukka area of Enugu state with all the dangers it portends. There is poor knowledge of the complications of pregnancy, labour and delivery among the respondents and there is poor knowledge of the referral system and the need for early referral. Some level of training and re-orientation, especially focused on early identification of signs of complications of pregnancy, labour and delivery and the earliest time to refer may be necessary to positively influence their practice especially as they are unavoidable links in improving referrals and maternal health in rural areas.
LIMITATION TO THE STUDY
The participants in this study were nominated purposively by the WDC chairmen, since there was lack of availability of TBA registry in the communities studied. Findings from this study therefore may not have adequately represented the true picture of TBA practices in the area.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abeshi SE, Njoku CO, Emechebe CI, Ago BU (2017). Sociodemographic characteristics and handling of life threatening obstetric cases by traditional birth attendants in Cross River State, Nigeria. Tropical Journal of Obstetrics and Gynaecology 34(3):177-181. |
|
|
Adatara P, Agani A, Faya B, Elizabeth A, Salia SM AA (2018). Perspective of Traditional Birth Attendants on Their Experiences and Roles in Maternal Health Care in Rural Areas of Northern Ghana. International Journal of Reproductive Medicine 2018:1-10. |
|
|
Brink E, Dellve L, Hallberg U, Abrahamsson KH, Klingberg GWK (2006). Constructing grounded theory: A practical guide through qualitative analysis. International Journal of Qualitative Studies on Health and Well-being 1(3):188-92. |
|
|
Fagbamigbe AF, Hurricane-Ike EO, Yusuf OB, Idemudia ES (2017). Trends and drivers of skilled birth attendant use in Nigeria (1990-2013): Policy implications for child and maternal health. International Journal of Womens' Health 9:843-53. |
|
|
Federal Ministry of Health (2013). National Demographic Health Survey 2013. Abuja, Nigeria. |
|
|
Federal Ministry of Health of Nigeria (2009). Saving newborn lives in Nigeria: Newborn health in the context of the Integrated Maternal, Newborn and Child Health Strategy [Internet]. Abuja; 2009. |
|
|
Glenton C, Colvin CJ, Carlsen B, Swartz A, Lewin S, Noyes J, Rashidian A (2013). Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: a qualitative evidence synthesis. Cochrane Database of Systematic Reviews 10(58). |
|
|
Izugbara CO, Ukwayi JK (2003). The clientele of traditional birth homes in rural Southeastern Nigeria. Health Care Women International 24(3):177-192. |
|
|
Izugbara CO, Ukwayi JK (2004). An intercept study of persons attending traditional birth homes in rural southeastern Nigeria. Culture, Health and Sexuality 6(2):101-114. |
|
|
Nbs. Annual Abstract of Statistics (2010). Federal Republic of Nigeria. 2010. |
|
|
Ntoimo LFC, Okonofua FE, Igboin B, Ekwo C, Imongan W, Yaya S (2019). Why rural women do not use primary health centres for pregnancy care: Evidence from a qualitative study in Nigeria. BMC Pregnancy Childbirth 19(1):1-13. |
|
|
Ofili AN, Okojie OH (2005). Assessment of the role of traditional birth attendants in maternal health care in Oredo Local Government Area, Edo State, Nigeria. Journal of Community Medicine and Primary Health Care 17(1):55-60. |
|
|
Ribeiro SD (2014). Traditional Birth Attendance in a health system: what are the roles, benefits and challenges: A case study of incorporated TBA in Timor-Leste. Asia Pacific Family Medicine 13(1):12. |
|
|
Sibley LM, Sipe TA, Brown CM, Diallo MM, McNatt KHN (2007). Traditional birth attendant training for improving health behaviours and pregnancy outcomes. Cochrane Cochrane Database of Systematic Reviews. |
|
|
Starrs A (2006). Motherhood initiative: 20 years and counting. The Lancet 368:1130-1132. |
|
|
Theron GB (2016). Sustainable development goals. Vol. 26, Obstetrics and Gynaecology Forum. New York. |
|
|
Tunçalp Î, Were WM, MacLennan C, Oladapo OT, Gülmezoglu AM, Bahl R, Daelmans B, Mathai M, Say L, Kristensen F (2015). Quality of care for pregnant women and newborns - The WHO vision. BJOG: An International Journal of Obstetrics and Gynaecology 122(8):1045-1049. |
|
|
Umeora OUJ, Egwuatu VE (2010). The role of unorthodox and traditional birth care in maternal mortality. Tropical Doctor 40(1):13-17. |
|
|
World Health Organization (WHO) (2018). Definition of skilled health personnel providing care during childbirth: the 2018 joint statement by WHO, UNFPA, UNICEF, ICM, ICN, FIGO and IPA. Geneva, Switzerland; 2018. |
|
|
World Health Organization (WHO) (2018). Recommendations on Antenatal Care for a Positive Pregnancy Experience : Summary Highlights and Key Messages from the World Health Organization's 2016 Global Recommendations for Routine Antenatal Care. Vol. 10. Geneva, Switzerland; 2018. |
|
|
World Health Organization (WHO) (2020). Maternal mortality [Internet]. [cited 2020 Apr 22]. |
|
|
World Health Organization (WHO) (2010). Maternal Health: Investing in the lifeline of healthy societies and economies. Policy Brief. September. 2010. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


