Full Length Research Paper

ABSTRACT
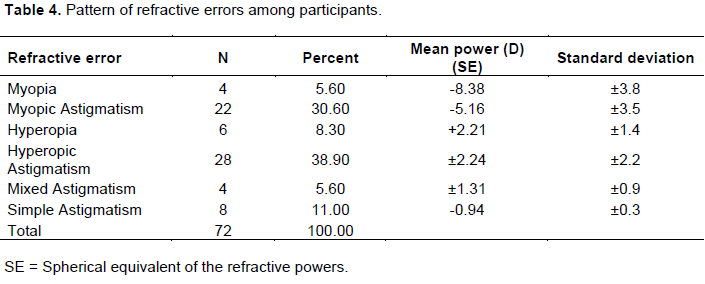
Albinism is a heterogenous group of disorders of melanin synthesis or distribution that is genetically inherited. Refractive errors are common in participants with albinism and high values have been reported. The aim of this study was to determine the pattern of refractive errors in people living with albinism in North-Western Nigeria. This was a prospective hospital-based study, carried out over 12 months from April 2017-March 2018 (12 months) whereby persons with albinism from Kano and Jigawa states were recruited. Ethical approval was obtained from the ethical review board of Aminu Kano Teaching Hospital. A structured proforma was used to record findings of history, examination and subjective and objective refraction were measured for each patient. Data was analysed using the statistical software SPSS version 20.0. A total of 61 participants with 122 eyes were examined. There were 32 males and 29 females (M: F= 1:1.1). Their ages ranged from 19 months to 60 years with a mean age of 16.77 ± 12.82 years. The pattern of refractive errors was hypermetropic astigmatism (38.90%), myopic astigmatism (30.60%), hypermetropia (8.30%) and mixed astigmatism (4%). Refractive errors are common in participants with albinism. In this study hypermetropic astigmatism is the most common refractive error.
Key words: Albinism, pattern, refractive error.
INTRODUCTION
Albinism is a heterogenous group of disorders of melanin synthesis or its distribution that is genetically inherited (Kanski, 2016). The clinical manifestations are associated with decrease or lack of pigmentation in the visual system and/or the skin and hair (Shah et al., 2020; Woertz et al., 2020). The prevalence of albinism ranged from as low as 1 in 15,000 in Nigeria (Enechukwu et al., 2020) to as high as 1 in 1,000 in Zimbabwe (Wright et al., 2015).
Tyrosinase is responsible for melanin synthesis, deficiency of such enzyme results in Albinism (Puzniak et al., 2019). In humans, melanin is the primary determinant of skin and hair color and pigmented tissues in the eyes.6 During development of the ocular structures, melanin deficiency causes clinical manifestations such as nystagmus, strabismus, foveal hypoplasia and refractive errors which explains the low visual acuity (Sayed et al., 2021; Pillay et al., 2021).
Albinism is classified into oculocutaneous albinism (OCA) and ocular albinism (OA). OCA is a group of four autosomal recessive disorders caused by either a complete lack or a reduction of melanin biosynthesis in the melanocytes resulting in hypopigmentation of the hair, skin and eyes. Reduction of melanin in the eyes results in reduced visual acuity caused by foveal hypoplasia and misrouting of the optic nerve fibres. The clinical spectrum of OCA varies, with OCA1A being the most severe type characterized by a complete lack of melanin production throughout life, while the milder forms OCA1B, OCA2, OCA3 and OCA4 show some pigment accumulation over time. The oculocutaneous albinism is inherited as an autosomal recessive genetic condition and there are seven types of OCA (OCA1-7) caused by mutations in seven different genes (Karen et al., 2007; Fukuda et al., 2015).
According to Karen et al (2007), OCA1 has a prevalence of approximately 1 per 40,000 in most populations but is very uncommon among African-Americans. In contrast, OCA2 is the most common type of albinism in African Black OCA patients (Fukuda et al., 2015). The overall prevalence of OCA2 is estimated to be 1:36,000 in the USA, but is about 1:10,000 among African Americans (Juan, 2021). It affects 1 in 3,900 of the population in some parts of the southern part of Africa (Chan et al., 2021). OCA3 or Rufous oculocutaneous albinism has been reported to affect 1:8,500 individuals in Africa, whereas it is very rare in Caucasians and Asiatic populations (Assoumou et al., 2020; Shah et al., 2020; Rooryck et al., 2006). Recently, mutations in a fourth gene were shown to be the cause of albinism, OCA4 (Suzuki et al., 2008; Newton et al., 2001), and were reported to explain the disease in approximately 5 to 8% of German patients with albinism (Sajid et al., 2021; Kubasch and Meurer, 2017) but 18% of Japanese patients (Lee et al., 2021; Inagaki et al., 2004).
Ocular albinism type I (OA1), or X-linked ocular albinism, is the most common form of ocular albinism. Ocular albinism is a genetic disorder characterized by vision abnormalities in affected individuals. Vision deficits are present at birth and do not become more severe over time. Affected individuals have normal skin and hair pigmentation. Ocular albinism is inherited as an X-linked recessive genetic condition and caused by mutations in the G protein-coupled receptor 143 (GPR143) gene (Fukuda et al., 2020).
The OCA and OA are group of congenital heterogeneous disorders of melanin biosynthesis in the melanocytes, OCA is inherited as an autosomal recessive genetic condition and most patients are compound heterozygotes, that is, harbouring two different mutations in one of the genes (Kubasch and Meurer, 2017).
All types of OCA and OA have similar ocular findings, including various degrees of congenital nystagmus, hypopigmentation of iris leading to iris translucency, reduced pigmentation of the retinal pigment epithelium, foveal hypoplasia, reduced visual acuity usually in the range 3/60 to 6/18 and refractive errors, and sometimes a degree of colour vision impairment. The diagnosis of OCA is based on clinical findings of hypopigmentation of the skin and hair, in addition to the characteristic ocular symptoms (McKay, 2019; Rothammer et al., 2017; Patel et al., 2020; Wu et al., 2020; Marçon et al., 2019; Zhong et al., 2019).
However, due to the clinical overlap between the OCA subtypes, molecular diagnosis is necessary in order to establish the gene defect and thus the OCA subtype. Molecular genetic testing of TYR and OCA2 are available on a clinical basis, while at present, analysis of TYRP1 and MATP is on research basis only. Molecular genetic testing is based on mutational analysis of the genes, by standard screening methods such as denaturing high-performance liquid chromatography (DHPLC) or single stranded conformational polymorphism (SSCP), followed by DNA sequencing. The different types of OCA are caused by mutations in different genes but the clinical phenotype is not always distinguishable, making molecular diagnosis a useful tool and essential for genetic counselling (Schidlowski et al., 2020; Dolinska et al., 2017; Chaki et al., 2005).
Refractive errors are common in patients with albinism and high values have been reported (Sayed et al., 2021; Khanal et al., 2016). Studies reported high percentages with the rule astigmatism as well as different incidences of both hypermetropia and myopia among patients with albinism (Sayed et al., 2021; Eballé et al., 2013; Udeh et al., 2014; Christine et al., 2000).
Sayed et al., (2021), reported that astigmatism and hypermetropia were the most common refractive errors, when compared in albino and non-albino children 100 and 62%, respectively, with significant difference between the both groups. Mean total astigmatism (TA), corneal astigmatism (CA) and lenticular astigmatism (LA) were significantly higher in albino group (P<0.05) and all albino eyes were high astigmats (≥1.25 D) (Sayed et al., 2021). Also, Eballé et al. (2013) found out that myopic astigmatism was the most common refractive error (40%) as compared with myopic patients, those with myopic astigmatism and hypermetropic astigmatism were four and ten times less likely to demonstrate significant improvement in distance visual acuity following optical correction among the thirty-five patients (70 eyes) diagnosed with complete oculocutaneous albinism (Khanal et al., 2016).
However, Udeh et al., (2014) assessed the burden and spectrum of refractive and non-refractive ophthalmic disorders in south-eastern Nigerians with oculocutaneous albinism. They found there were high prevalence of refractive, non-refractive and mixed ophthalmic disorders among albinos in south-eastern Nigeria. Refractive disorders comprised astigmatism -73.2% eyes, myopia -23.9% and hypermetropia 2.9%. Spherical refractive errors ranged from -14.00 DS to +8.00 DS while astigmatic errors ranged from -6.00 DC to +6 DC. Non-refractive disorders comprised nystagmus, foveal hypoplasia, hypopigmented fundi and prominent choroidal vessels in 100.0% participants; and strabismus in 16.3% participants. Mixed refractive and non-refractive disorder, that is, presenting visual impairment was present in all the participants. Moreover, the overall refractive profile of oculocutaneous albinos was consistent with emmetropization being impaired in albinism as reported by Christine et al. (2000). The refractive errors of hyperopic albinos also can be explained in terms of meridional emmetropization. The contrasting refractive profiles of myopic albinos may reflect operational constraints of the emmetropization process.
The aim of this study was to determine the pattern of refractive errors in participants with albinism in two states of north-western Nigeria.
METHODOLOGY
This was a prospective hospital based cross sectional study, which was carried out from April 2017 to March 2018. The study adhered to the Tenets of the Helsinki Declaration. Ethical approval was obtained from the Ethical Review Board of Aminu Kano Teaching Hospital and also, informed consents were obtained from each participant before enrolling them in the study. Reduced retinal pigment with visualization of the choroidal blood vessels on ophthalmoscopic examination during the clinical tests and procedures. Persons with albinism were recruited from Jigawa and Kano states in collaboration with the Albino Foundation of the respective states. The inclusion criteria were all albinos with all the clinical phenotypical features such as reduced visual acuity, nystagmus, reduced iris pigment with iris translucency, fundus hypopigmentation, foveal hypoplasia associated with reduction in visual acuity, misrouting of the optic nerves at the chiasm including: alternating strabismus and reduced stereoscopic vision, hypopigmentation of skin and hair of the oculocutaneous albinism from albino foundation of the respective two state chapters during the study period and who agreed to participate in the study. The exclusion criteria were albinos who did not belong to albino foundation, or were not in Jigawa and Kano states as at the time of the study or refused to participate. The albinos selected for this study were received in a defined order of passage and all were provided a full and free ophthalmic consultation carried out by an eyecare team made up of optometrists and ophthalmologists. The variables studied were age, sex, unaided (uncorrected) and aided (corrected) visual acuities, objective refraction, subjective refraction and cycloplegic refraction.
They were evaluated at the Ophthalmology Clinic of Aminu Kano Teaching Hospital Kano. A structured proforma was used for recording findings of ocular history, general and ocular examination, objective and subjective refraction. The visual acuity (VA) both for distance and near of each participant that met the inclusion criteria was determined using the illuminated Snellen’s visual acuity chart and Jaeger’s reading chart, respectively. Illiterate chart was used where indicated and the pictorial projected Snellen chart and the isolated optotype chart were used for children between the ages of one to five years, some adolescents and adults experiencing crowding phenomenon. Each participant’s monocular VA was tested unaided and with a pinhole starting conventionally with the right eye. Participants with VA of ?6/6 that improved with pinhole were determined to have a refractive error. The same procedure was repeated with the left eye and was recorded accordingly. The near VA was also determined at 33 cm with the Jaeger’s reading chart monocularly then binocularly.
The participant’s objective refraction was determined using the streak retinoscopy at two - third meter working distance in a dimly illuminated room followed by the subjective refraction at 6-m distance with the Phoropter (TOPCON companies 2004, Beijing, China). Having determined the best corrected distance visual acuity (BCDVA) of each participant, those who were in the presbyopic age group or those whose near VA indicated need for presbyopic correction were asked to look at the N5 line of the reading chart, and plus spherical lenses were added in +0.25DS steps starting with +1.00DS. The total plus lenses added over the BCDVA was recorded as the final presbyopic correction. Cycloplegic refraction with atropine 1% was carried out on participants between the ages of 1 to 12 years, while cyclopentolate 1% combined with tropicamide 1% were used for subjects between 13 and 20 years.
The drugs were instilled into the conjunctival sac of the subjects, it comprised instillation of one drop of 1% atropine twice daily before and on the day of refraction and instillation of 1% cyclopentolate and 1% tropicamide, respectively. Cyclopentolate (1%) was instilled twice at 5 min intervals followed by tropicamide (1%) also instilled twice at 5 min intervals. Cycloplegic refraction with retinoscope (Keeler, Windsor, SL4 4AA UK) was done 30 min after instillation of the last drop of tropicamide and was done by the same clinician. For both regimens, cycloplegic effect of the drugs was noted when the pupils did not react to light and were fully dilated and when retinoscopic reflex did not fluctuate (Sani et al., 2016).
The refractive errors status after subjective refraction was group into six (6) categories, namely: myopia (those with minus spherical power ranging from -0.50 Diopter Sphere (DS) and above only), myopic astigmatism (those with minus spherical of -0.50DS combined with minus cylindrical powers of ± 0.50 Diopter Cylinder (DC) ≥ 6.00DC), hypermetropia (those with plus spherical power ranging from +0.50DS and above only), hypermetropic astigmatism (those with plus spherical of +0.50DS combined with minus cylindrical powers ± 0.50DC ≥ 6.00DC), mixed astigmatism (those with minus cylindrical and plus cylindrical powers of ± 0.50DC ≥ 6.00DC) and simple astigmatism (those with plano spherical power combined with ± 0.50DC ≥ 6.00DC cylindrical powers). The results of these findings were converted to their various spherical equivalents and recorded using the Microsoft excel spreadsheet database and was analyzed with the Statistical Package for Social Sciences version 20.0 (SPSS Inc., IIIinois, USA).
RESULTS
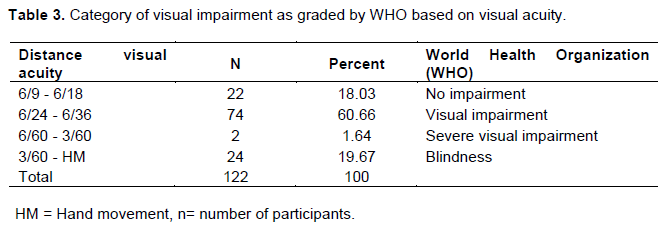
A total of 61 participants with 122 eyes were examined. There were 32 males and 29 females (M: F= 1:1.1) (Figure 1). Their ages ranged from 19 months to 60 years with a mean age of 16.77 ± 12.82 years (Table 1). The mean uncorrected VA of the participants was 0.93±0.25 Log Mar. Table 2 shows the distribution of corrected and uncorrected VA among participants. Table 3 relates the degree of visual impairment with distance VA. Of all the participants, 18.03% had no visual impairment. Out of the 61 participants, 11 had refractive errors in each eye giving a total frequency of 72. Table 4 shows the pattern of refractive errors among participants.



DISCUSSION
Albinism is less common in Nigeria compared to other countries such as Cameroon. (Enechukwu et al., 2020) People with albinism face challenges ranging from cultural taboos to health problems including the eye. They have a shorter life span in sub-Saharan Africa, accompanied with poor quality of life due to associated visual impairment (Sayed et al., 2021). This could be the explanation for the age distribution seen in the study whereby it peaks at adolescence. This is comparable to a study by Eballe et al (2013) and other studies which also showed similar age distribution (Woertz et al., 2020; Saka et al., 2020; Rymer et al., 2007). Although there is paucity of data to explain this, a likely reason could be due to increased risk of skin cancers in the already vulnerable (Sayed et al., 2021; Rymer et al., 2007). This is comparable to a study by Eballe et al., (2013) and other studies which also showed similar age distribution (Woertz et al., 2020; Saka et al., 2020; Rymer et al., 2007). Although there is paucity of data to explain this, a likely reason could be due to increased risk of skin cancers in the already vulnerable (Sayed et al., 2021; Rymer et al., 2007).
This population has visual impairment which directly or indirectly affects their education and in turn their livelihood which is compounded by social discrimination and stigmatization that unfavorably reduces their quality of life. Albinism has no gender predominance, even though this study showed a slight male predominance which is in keeping with previous studies and may be a random finding (Wright et al., 2015; Schulze et al., 2015).
Visual impairment in albinism is caused by either refractive errors or optic system pathology (Pillay et al., 2021; Chan et al., 2021). Some studies have shown that albinism is associated with high refractive errors, just as in this study (Karen et al., 2007; Fukuda et al., 2015; Juan, 2021). All the patients had some form of refractive error with hyperopic astigmatism accounting for most of the cases even though evidence has shown that myopia is the most common refractive error in patients with albinism, some studies had findings similar to that of the present study (Karen et al., 2007; Chan et al., 2021; Suzuki et al., 2008). Refractive errors in albinism have been shown to be as a result of impairment or arrest of emmetropization. Hyperopia is an evidence that there is form of emmetropization which is impaired rather than arrested (Sayed et el., 2021).
Other studies went further to show that tryrosinase negative albinism is associated with myopia while hyperopia is associated with tyrosinase positive albinism (Chan et al., 2021; Esther et al. 2006). This could explain why hyperopic patients were more than myopic patients in this study. It may have been that the majority of the patients were tyrosinase positive which led to hyperopia being more common, however, the hair bulb test was not done to confirm this, which served as a limitation to this study (Karen et al., 2007; Fukuda et al., 2015; Saka et al., 2020; Rymer et al., 2007). Moreover, in support of this, Liqin et al (2018), also found that the retinal tyrosine hydroxylase (TH) pathway was not significantly different between the albino myopic (AM) and the pigmented hyperopic (PH) guinea pigs. Therefore, they hypothesized that the tyrosinase-dependent dopaminergic system is another important regulator of the postnatal refractive error development under normal vision conditions, while the TH-dependent retinal dopaminergic system is involved in form-deprivation myopia (Liqin et al., 2018).
The study also showed that those with pure ametropia were few and most were accompanied with astigmatism, similar with previous studies although some showed that all cases had astigmatism (Sayed et al., 2021; Juan, 2021). These studies additionally showed that with the rule astigmatism is frequently encountered because of nystagmus which molds the cornea, due to rubbing of the eyelid on the corneal surface (Sayed et al., 2021; Karen et al., 2007). One will expect alleviation of astigmatism with lifting of the eyelids but this will not be so because of its chronicity (Karen et al., 2007; Juan, 2021).
Refraction in albinism improves the vision but with subnormal vision persisting as in this study. This is because there are other pathologies such as foveal hypoplasia, abnormal decussation of the optic nerves, light scatter and nystagmus. All these contribute to visual impairment which limits improvement of vision by optical correction. Another contributing factor is amblyopia, depending on the severity and age of correction. However, compliance with spectacle wear has shown improved stereopsis and ocular alignment (Juan, 2021; Fukuda et al., 2015).
CONCLUSION
This study has shown that albinism is associated with visual morbidity caused by refractive errors mainly hypermetropic astigmatism. For this reason, refraction at an early age is vital for improving visual outcome, quality of life and preventing amblyopia.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Assoumou PA, Aki TM, Oussavou O, Mengome EM (2020). Clinical Characteristics of Nystagmus in Albinos Living in Libreville. Open Journal of Ophthalmology 10(1):69-76. |
|
|
Chaki M, Mukhopadhyay A, Ray K (2005). Determination of variants in the 3'-region of the tyrosinase gene requires locus specific amplification. Human Mutation 26(1):53-58. |
|
|
Chan HW, Schiff ER, Tailor VK, Malka S, Neveu MM, Theodorou M, Moosajee M (2021). Prospective Study of the Phenotypic and Mutational Spectrum of Ocular Albinism and Oculocutaneous Albinism. Genes 12(4):508 |
|
|
Christine FW, Peter JO, Simon C (2000). Albinism: Its Implications for Refractive Development. Investigative Ophthalmology and Visual Science 41(1):1-7. |
|
|
Dolinska MB, Kus NJ, Farney SK, Wingfield PT, Brooks BP, Sergeev YV (2017). Oculocutaneous albinism type 1: link between mutations, tyrosinase conformational stability, and enzymatic activity. Pigment Cell and Melanoma Research 30(1):41-52. |
|
|
Eballé AO, Mvogo CE, Noche C, Zoua ME, Dohvoma AV (2013). Refractive errors in Cameroonians diagnosed with complete oculocutaneous albinism. Clinical Ophthalmology 7:1491-1500 |
|
|
Enechukwu NA, Ogun GO, Ezejiofor OI, Chukwuanukwu TO, Yaria J, George AO, Ogunbiyi AO (2020). Histopathologic patterns of cutaneous malignancies in individuals with oculocutaneous albinism in Anambra state, Nigeria: a paradigm swing? Ecancermedicalscience 14:1013. |
|
|
Esther SH, Hajo Z, Michael HR (2006). Albinism in Africa as a Public health issue. BMC Public Health 6(1):212. |
|
|
Fukuda N, Naito S, Masukawa D, Kaneda M, Miyamoto H, Abe T, Yamashita Y, Endo I, Nakamura F, Goshima Y (2015). Expression of ocular albinism 1 (OA1), 3, 4- dihydroxy- L phenylalanine (DOPA) receptor, in both neuronal and non-neuronal organs. Brain Research 1602:62-74. |
|
|
Inagaki K, Suzuki T, Shimizu H, Ishii N, Umezawa Y, Tada J, Kikuchi N, Takata M, Takamori K, Kishibe M, Tanaka M, Miyamura Y, Ito S, Tomita Y (2004). Oculocutaneous albinism type 4 is one of the most common types of albinism in Japan. American Journal of Human Genetics 74:466-471. |
|
|
Juan AG (2021). Comparative transcriptomics of albino and warningly-coloured caterpillars. Ecology and Evolution 11(12):7507-7517. |
|
|
Kanski JJ (2016). Clinical ophthalmology. 8th edition. Butterworth Heinemann, Oxford 668 p. |
|
|
Karen G, Jakob Ek, Karen BN (2007). Oculocutaneous albinism. Orphanet Journal of Rare Diseases 2(1):1-8. |
|
|
Khanal S, Pokharel A, Kandel H (2016). Visual deficits in Nepalese patients with oculocutaneous albinism. Journal of Optometry 9(2):102-9. |
|
|
Kubasch AS, Meurer M (2017). Oculocutaneous and ocular albinism. Hautarzt 68(11):867-875. |
|
|
Lee SY, Lee EJ, Byun JC, Jang KM, Kim SY, Hwang SK (2021). A new type of oculocutaneous albinism with a novel OCA2 mutation. Yeungnam University Journal of Medicine 8(2):160-164. |
|
|
Liqin J, Sen Z, Rongfang C, Li M, Xiaojun W, Yingying W, Jia Q, Xiangtian Z (2018). Effects of the Tyrosinase-Dependent Dopaminergic System on Refractive Error Development in Guinea Pigs. Investigative Ophthalmology and Visual Science 59:4631-4638. |
|
|
Marçon CR, Maia M (2019). Albinism: epidemiology, genetics, cutaneous characterization, psychosocial factors. Anais Brasileiros de Dermatologia 94(5):503-520. |
|
|
McKay BS (2019). Pigmentation and vision: Is GPR143 in control? Journal of Neuroscience Research 97(1):77-87. |
|
|
Newton JM, Cohen-Barak O, Hagiwara N, Gardner JM, Davisson MT, King RA, Brilliant MH (2001). Mutations in the human orthologue of the mouse underwhite gene (uw) underlie a new form of oculocutaneous albinism, OCA4. American Journal of Human Genetics 69:981-988. |
|
|
Patel N, Bhadarka HK, Vaniawala S, Patel A (2020). A Successful Case for Deselection of Albino Embryo and Live Birth of Albinism-Free Healthy Baby Followed by PGT-M. Journal of Human Reproductive Sciences 13(3):245-248. |
|
|
Pillay E, Naidoo T, Asmal K, Maliwa L, Mchunua S, van Staden DB, Rampersad N (2021). Characterization of Retinal Thickness in Individuals with Albinism: Baseline Data for a Black South African Population. Clinical Optometry 13:15-22. |
|
|
Puzniak RJ, Ahmadi K, Kaufmann J, Gouws A, Morland AB, Pestilli F, Hoffmann MB (2019). Quantifying nerve decussation abnormalities in the optic chiasm. Neuroimage Clinical 24:102055. |
|
|
Rooryck C, Roudaut C, Robine E, Müsebeck J, Arveiler B (2006). Oculocutaneous albinism with TYRP1 gene mutations in a Caucasian patient. Pigment Cell and Melanoma Research 19:239-240. |
|
|
Rothammer S, Kunz E, Seichter D, Krebs S, Wassertheurer M, Fries R, Brem G, Medugorac I (2017). Detection of two non-synonymous SNPs in SLC45A2 on BTA20 as candidate causal mutations for oculocutaneous albinism in Braunvieh cattle. Genetics Selection Evolution 49(1):73. |
|
|
Rymer J, Choh V, Bharadwaj S, Padmanabhan V, Modilevsky L, Jovanovich E, Yeh B, Zhang Z, Guan H, Payne W, Wildsoet CF (2007). The albino chick as a model for studying ocular developmental anomalies, including refractive errors, associated with albinism. Experimental Eye Research 85(4):431-442. |
|
|
Sajid Z, Yousaf S, Waryah YM, Mughal TA, Kausar T, Shahzad M, Rao AR, Abbasi AA, Shaikh RS, Waryah AM, Riazuddin S, Ahmed ZM (2021). Genetic Causes of Oculocutaneous Albinism in Pakistani Population. Genes 12(4):492. |
|
|
Saka B, Teclessou JN, Akakpo SA, Gnossike P, Doh K, Adam S, Mouhari-Toure A, Mahamadou G, Kassang P, Elegbede Moise Y, Darre T, Kombate K, Pitché P (2020). A Histopathological Study of Skin Lesions in Individuals with Oculocutaneous Albinism in Togo in 2019. Journal of Skin Cancer 2361957. |
|
|
Sani RY, Hassan S, Habib SG, Ifeanyichukwu EP (2016). Cycloplegic effect of atropine compared with cyclopentolate-tropicamide combination in children with hypermetropia. Niger Medical Journal, 57:173-7. |
|
|
Sayed KM, Mahmoud AM, Gad KA (2021). Analysis of the Refractive Profile of Children with Oculocutaneous Albinism versus an Age-Matched Non-Albino Group. Clinical Ophthalmology 15:73-78. |
|
|
Schidlowski L, Liebert F, Iankilevich PG, Rebellato PRO, Rocha RA, Almeida NAP, Jain A, Wu Y, Itan Y, Rosati R, Prando C (2020). Non-syndromic Oculocutaneous Albinism: Novel Genetic Variants and Clinical Follow Up of a Brazilian Pediatric Cohort. Frontiers in Genetics 11:397. |
|
|
Schulze SM, Kumar N, Bohrmann D, Msukwa G, Kalua K, Kayange P, Spitzer MS (2015). Refractive errors, visual impairment, and the use of low-vision devices in albinism in Malawi. Graefe's Archive for Clinical and Experimental Ophthalmology 253(4):655-661. |
|
|
Shah M, Khan MT, Saeed N (2020). Visual rehabilitation of people with oculocutaneous albinism in a tertiary clinical setting in Pakistan. Saudi Journal of Ophthalmology 34(2):111-115. |
|
|
Suzuki T, Tomita Y (2008). Recent advances in genetic analyses of oculocutaneous albinism types 2 and 4. Journal of Dermatological Science 51:1-9. |
|
|
Udeh NN, Eze BI, Onwubiko SN, Arinze OC, Onwasigwe EN, Umeh RE (2014). Prevalence and profile of ophthalmic disorders in oculocutaneous albinism: a field report from South-Eastern Nigeria. Journal of Community Health 39(6):1193-1199. |
|
|
Woertz EN, Omoba BS, Dunn TM, Chiu SJ, Farsiu S, Strul S, Summers CG, Drack AV, Carroll J (2020). Assessing Ganglion Cell Layer Topography in Human Albinism Using Optical Coherence Tomography. Investigative Ophthalmology and Visual Science 61(3):36. |
|
|
Wright CY, Norval M, Hertle RW (2015). Oculocutaneous albinism in sub-Saharan Africa: adverse sun-associated health effects and photoprotection. Photochem Photobiol 91(1):27-32. |
|
|
Wu KC, Lv JN, Yang H, Yang FM, Lin R, Lin Q, Shen RJ, Wang JB, Duan WH, Hu M, Zhang J, He ZL, Jin ZB (2020). Nonhuman Primate Model of Oculocutaneous Albinism with TYR and OCA2 Mutations. Research Washinton DC. 2020:1658678. |
|
|
Zhong Z, Gu L, Zheng X, Ma N, Wu Z, Duan J, Zhang J, Chen J (2019). Comprehensive analysis of spectral distribution of a large cohort of Chinese patients with non-syndromic oculocutaneous albinism facilitates genetic diagnosis. Pigment Cell and Melanoma Research 32(5):672-686. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


