Full Length Research Paper

ABSTRACT
Long-acting reversible contraception (LARC) methods, including intrauterine contraceptives and subdermal implants, are some of the most effective contraceptive methods available. They are known to be convenience, cost effective and suitable for many women. The study aims to determine the trends and uptake of long acting reversible contraception in University of Maiduguri Teaching Hospital, Maiduguri, assess the characteristics of the acceptors and identify the reason for discontinuation of the methods. A 5 years retrospective study was conducted at the family planning clinic of University of Maiduguri Teaching Hospital from 1st January 2015 to 31st December 2019. Case notes for all acceptors of LARC were retrieved. Data extracted include socio demographic characteristics of acceptors, previous contraceptive use and reason for discontinuation after one year of use; statistical significance was tested using chi-square. The results showed that 4064 new clients accepted the available family planning methods in University of Maiduguri Teaching Hospital, during the study period. Out of this, 43.1% accepted sub dermal implant, and only 9.0% uses intra uterine contraceptive device (IUCD). Findings further revealed that there is a significant relationship (P<0.05) between uptake of LARCs and related socio demographic characteristics in this study. This means that adolescent are less likely to use LARC so also those of low parity. Reason for discontinuation include desire for more children, irregular menses, and contraceptive faire; husband refusal, weigh gain, infection and missing string of IUCD. The rising uptake of subdermal implant in this study is encouraging, however there is a low uptake of IUCD and adolescent are less likely to use LARC. Some clients discontinue the methods within one year of use. Therefore appropriate counseling, follow up care and management of side effects and clients inconveniences, involving men in reproductive health are important in reducing the rate of discontinuation and improved the uptake of LARC.
Key words: Long-acting reversible contraception (LARC), reason for discontinuation, Nigeria.
INTRODUCTION
The state of Nigeria today is a matter of great concern, Nigeria is one of the most densely populated countries in Africa, with approximately 200 million people in an area of 923,768 km2 (356,669 sq. mi), (National Population Commission and ORC/Macro. National Population Commission/Federal Ministry of Health, 2018) and is also the country with the largest population in Africa (National Population Commission and ORC/Macro. National Population Commission/Federal Ministry of Health 2018) and the seventh largest population in the world. (National Population Commission and ORC/Macro. National Population Commission/Federal Ministry of Health, 2018) and (National Population Commission, 2018) Population growth (annual %) in Nigeria was reported at 2.5648% in 2018, this will have enormous implications for diverse socio-economic ills and health challenges, including poor maternal and neonatal health, (National Population Commission, 2018) One major reason for the persistent high fertility level and high maternal and child mortality rate across the country is the low level of contraceptive uptake. For example, modern contraceptive prevalence rate was estimated at 11% among Nigerian women. (World Health Organization, 2019)
Although the annual number of global maternal mortality has decreased between 2000 and 2017, the maternal mortality ratio (MMR, number of maternal deaths per 100,000 live births) dropped by about 38% worldwide. However it is still remains very high in Nigeria (917 death per 100.000 live birth), as the region accounts for 14% of the whole maternal deaths (World Health Organization, 2019). Family planning has been reported to be the key in the increased female productivity by reducing their fertility and ensuring child survival and improved maternal health (Usman et al., 2019).
A variety of contraception options are available, these can be grouped into two categories. These are long-acting reversible and permanent contraceptive methods (like intrauterine devices, implants, and sterilization) and short-acting (like pills, condoms, spermicides, injectable, and other modern methods, and all traditional methods) (Mukamuyango et al., 2014).
Newer long-acting reversible contraceptive (LARC) methods such as intrauterine devices and sub dermal implants are preferred because they do not depend on patient conformity (Mukamuyango et al., 2014). They are highly effective and appropriate for most women and have the additional advantages of being long-lasting, convenient, well-liked by users and cost effective. LARC methods are 'forgettable'; they are not dependent on compliance with a pill-taking regimen, or coming back to the clinician for an injection (Bhandari et al., 2019) LARC method failure rates rival that of tubal sterilization at <1% for IUDs and the sub dermal implant (Mukamuyango et al., 2014; Bhandari et al., 2019).
Despite the improvement in availability and utilization of long acting reversible contraception, early discontinuation is becoming a major problem. Significant proportion of women discontinues the methods within one year even without any side effect (Staveteig et al., 2015). According to a report based in Nigeria, 13% of IUD users and 2% of Implanon users discontinue the methods during the first 12 months (Aruna et al., 2015).
Higher discontinuation rate of long acting reversible contraception is a public health concern; long acting reversible contraceptives which are designed to be used for 3 to 12 years are coast effective only when they serve for the intended period of time.
Against this background, this study aimed to document the trends and uptake of LARC methods among women in our setting, assess the characteristics of the acceptors, and identify the reason for discontinuation so that strategies can be put in place to maximize their benefits.
MATERIALS AND METHODS
The study setting was a tertiary hospital located in Maiduguri, northeast Nigeria and catering for the metropolis and its environs. The family planning clinic of University of Maiduguri Teaching Hospital (UMTH), Maiduguri provides family planning services from Monday to Friday between 8.0 am to 4.0 pm. A consultant obstetrician and gynecologist, and four trained nurses direct activities in the clinic. Medical and nursing students and resident doctors in Obstetrics and Gynecology are posted to the clinic for clinical experiences. The services provided in the clinic include family planning counseling, same day provision of chosen methods to clients, teaching, research, training of students, and medical record documentations. Group family planning counseling is undertaken at regular intervals in the antenatal clinics. Approval for this study was obtained from the Ethics and Research Committee of the University of Maiduguri Teaching Hospital.
A retrospective study design to evaluate uptake of LARC (intrauterine contraceptive devises and implant) was conducted. All available client records from the family planning clinic from January 1st, 2015 to December 31st, 2019 were retrieved. Information was collected on socio-demographic characteristics, previous contraceptive use, method of contraception chosen at the first visit and reason for discontinuation within one year of insertion.
Data analysis
Data was analyzed using the statistical package for social sciences (SPSS) version 15. Missing responses were stated as such and excluded from analysis. Descriptive analysis was done using frequencies and percentages. Chi square was used as a test of association between methods of contraception used and demographic characteristics (other relevant factors such as reason for discontinuation). Significance level was established at P value of 0.05.
RESULTS
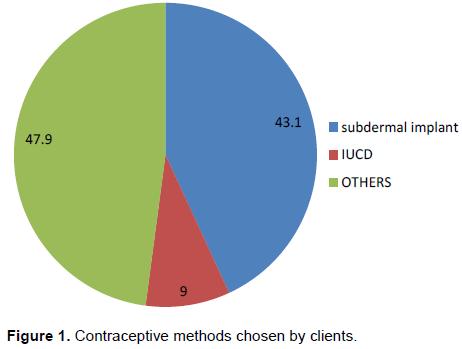
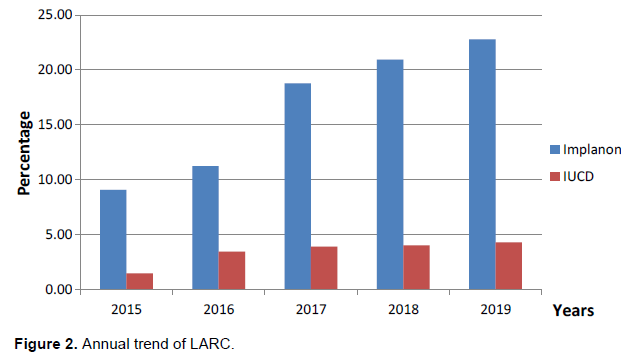
Four thousand and sixty four (4064) new clients accepted the available family planning methods in University of Maiduguri Teaching Hospital, Maiduguri, Borno State Nigeria during the study period. A total of 1752(43.1%) accepted sub dermal implant, 363(9.0%) accepted IUCD and 1947(47.9%) accepted others form of contraception. This is shown in Figure 1. There has been a general upward trend showing that LARC uptake has overtime continued to gain some increase among users in this study (as shown in Figure 2). Sub dermal implant uptake increased from 9.08% in 2015 to 22.79% in 2019 and IUCD uptake steadily increased from 1.47% in 2015 to 4.30% in 2019.
Majority of the clients using LARC were mostly aged 21-39 years 1823(86.1%), only 142(6.7%) were less than 20 years. Nine hundred and thirty one (44.0%) of the new acceptors had secondary education, 485(22.9%) had tertiary education, and 637(30.1%) had no formal education; unemployed were 889 (42.0%), and civil servant were 662(31.3%), and self-employed were 566(28.8%). Acceptance of the contraceptive methods increased as parity increased with a peak at Para 5 and above 764 (36.1%). Parity 0 acceptors were 0.2% only. Most of them had 1 to 4 living children.
Table 1 presents results from bivariate analysis which explored the relationship between the use of LARC method and selected demographic characteristics. As shown in the table, some of the characteristics are significantly associated with LARC uses. For instance, those who are aged less than 20 years and more than 40 years had lower proportion of use of LARC (7.0 and 8.65%) compared to those age 21-30 and 31- 40 (43.73 and 42.41%) respectively. With regard to parity, respondent who does not have a child (0.2%) are less likely to use LARC compare to those of high parity (35.6%).
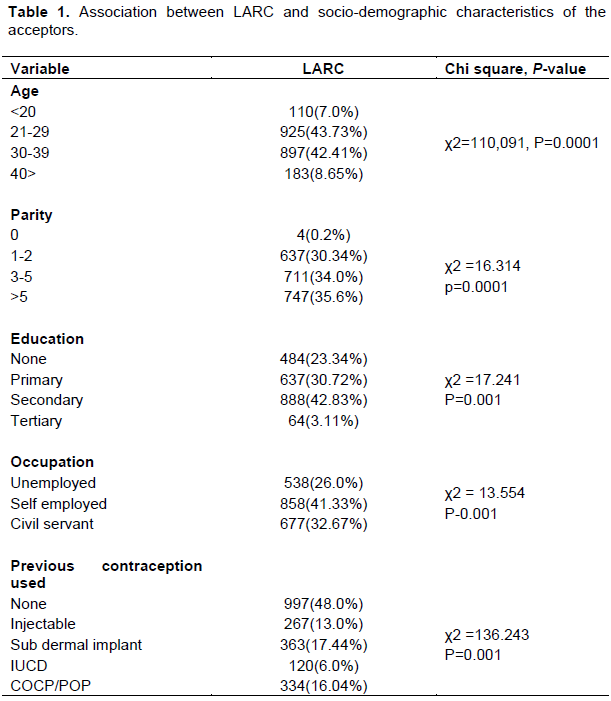
Level of education is associated with the use of LARC; those who had secondary level of education are more likely to use LARC (42.83%) compared to those who had primary (30.72%) and no formal education (23.34%). Respondents who are self-employed were most likely to use LARC contraceptives (41.33%), followed by civil servant (32.67%) and those who are not employed being the least (26.0%).
Acceptance of LARC were more likely from those who had never used contraception before (48.0%), and those choosing LARC were most likely to have used sub dermal implant in the past.
Majority of the clients discontinued the methods because they want to get pregnant 739(34.9%), some because the duration had elapsed 512 (24.1%), and menstrual irregularity was about 493(23.3%), others reason such as husband refusal, missing string of IUCD, pelvic infection and weigh gain constituted about 262(12.4%). Only 111(5.2%) of them was due to contraceptive failure.
Table 2 shows the association between socio-demographic characteristic of the clients and the reason for discontinuation of LARC to be significantly different (p value <0.05). Younger age groups are more likely to discontinue due to desire for more children (43.3%) compare with those with ages ≥40 (27.6%). Menstrual irregularity is the commonest reason for discontinuation in those aged < 20 (25.5%) than those aged > 40 (15.8%). Older clients are more likely to carry the contraception up to the duration elapsed (34.2%) than those less than 20 years (16.3%).
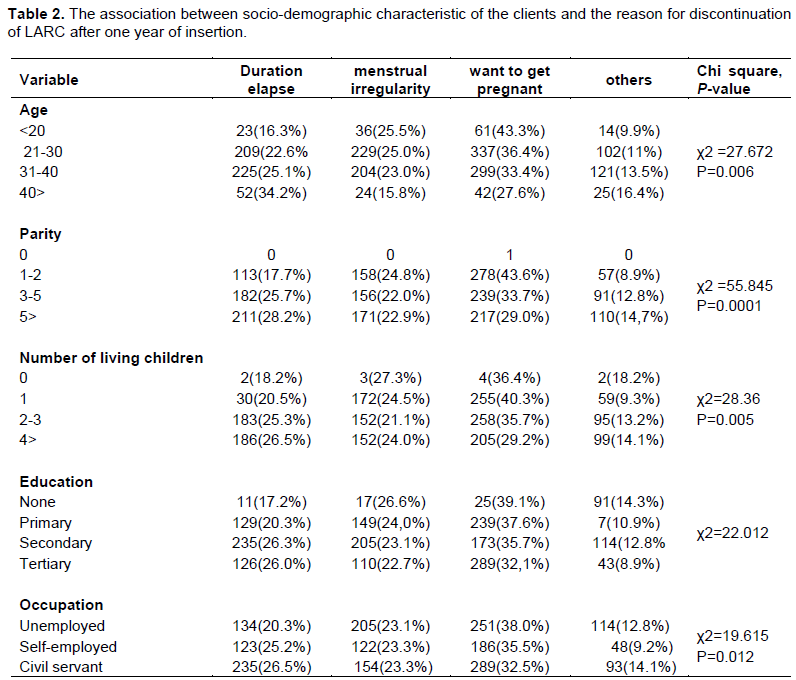
Clients with fewer numbers of children were more likely to discontinue LARC due to desire for pregnancy (43.6%) compare to those with more children (29.0%). Those with Para 1 to 2 were more likely to discontinue the methods as a result of menstrual irregularity (24.8%) while those with high parity are more likely to continue till the time had elapsed (28.2%).
Those with one living child were more likely to discontinue the method for desire for more pregnancy (40.3%) and menstrual irregularity (24.5%), while those with more than four living children were more likely to use it till the duration elapsed (26.5%). Clients who had no formal education were more likely to discontinue due to desire for more children (39.1%), menstrual irregularity (26.6%) compare to those who had tertiary education (32.1%). Those who are not employed were more likely to discontinue LARC due to desire for more children (38.0%) while civil servants were more likely to continue using LARC till the time elapsed (26.5%).
DISCUSSION
In this study, the trends and uptake of long-acting reversible contraception has increased, this is primarily attributable to an increase in Implant use, and IUCD uptake is low. The reason for discontinuation was desire for another pregnancy, irregular menses, husband refusal, weight gain and pelvic infection among LARC users. Socio demographic characteristics such as age of women, parity, occupation, education were the contributing factors of LARC use and early discontinuation.
The uptake rate of 52.1% for LARC in the study is high. This is in contrast to the finding from previous study (38.7, 2.0.4 and 14.8%) (Mohammed et al., 2017; Bolarinwa and Olagunju, 2019). This may be probably as a result of increase awareness and skill of health care provider on the insertion and removal skill. Among those who used LARC methods, substantial proportion of them used implants (43.1%) and only 9.0% used IUCD. This finding agreed with other findings which reported that majority of their respondents used implants (Aregay et al., 2018; Bolarinwa and Olagunju, 2019; Igwebueze, 2017). Lower rate of IUCD utilization among acceptors may be partially explained by misconceptions about LARC methods and their related side effect.
Annual trends in LARC uptake in the study demonstrate a steady upward slanting in contraceptive implants and decline in IUD uptake. This is in accordance from previous finding (Moreau et al., 2013; Adedini et al., 2019; Darroch et al., 2013). Women might choose implants probably because they like the convenience and duration of contraceptive protection, and implants can be inserted without undergoing a pelvic exam. This could suggest a provider preference for implants with a prepackaged applicator over IUCD that require a trocar for insertion (Bikorimana, 2015; Bolarinwa and Olagunju, 2019).
Clients using LARC were mostly aged 21 to 39 years, educated up to secondary level, multiparous and had at least one living child. This is similar to the study done in Kaduna and Enugu (Mohammed et al., 2017; Igwebueze, 2017). Findings showed that older women were more likely to use LARC methods, compared to their younger counterparts. Possible explanation for this is that older women tend to have more children, have completed their family size and perhaps desire no more children; hence their preference for LARC method compared to short acting contraceptives (Coombe et al., 2017; Bratlie et al., 2014). Adolescent are less likely to use LARC, this is in line with some previous study (Nicole et al., 2017; Lisa et al, 2015; Francis et al., 2017); these group of clients are very fertile and vulnerable to unintended pregnancy and its complications. Unfortunately, it appears that our family planning clinic is not adolescent-friendly, or they are afraid of stigmatization. This may explain the poor uptake rate by adolescents in this study.
The results also showed that likelihood of using LARC methods was significantly much higher among multiparous women, particularly those who had 5 or more children, compared to their childless counterparts. In addition, women who had no desire for more children were more likely to adopt LARC methods than those who desired more children. This is expected, as long-acting contraceptives are generally viewed as permanent contraceptive methods and are mostly used to limit childbearing.
Furthermore, the use of LARC methods was higher among educated women compared to those with no education. This is in agreement with previous study (Luchowski et al., 2014; Ochako et al., 2016). Correct knowledge about LARC methods is a key factor to ensure increased and appropriate use, and also avoid misinformation that can hinder women to adopt methods not suitable for them.
The study shows that the acceptors of LARC were more likely from those who had never use any form of contraception before and those who have had sub-dermal implant want .to continue with the method. This is probably because they had good counseling on the effectiveness and safety on LARC in the clinics.
The finding that most of the clients uses LARC till the duration elapses and contraception failure is about 5% makes sense. With adequate counseling and provision, it is presumed that women who choose an IUD or implant intend to use it for a sustained period of time (Ochako et al., 2015; Thompson et al., 2018). IUDs and implants are also provider-discontinued methods, whereas injectable and some modern methods can be discontinued passively, require continuous renewal, or are coitus-dependent.
The study showed that younger women were more likely to discontinue the methods compared to older one (P<.05). The commonest reason for discontinuation was desire for another pregnancy among users and irregular menses. Clients aged less 20 years were less likely to continue the method till the duration elapse. This is in accordance with previous study. (ACOG, 2012; Ezegwui et al., 2011; The American College of Obstetricians and Gynecologists, 2014). The increased risk of early discontinuation among adolescents, as compared with older women, may reflect lower adherence to the method. Most pregnancies among teenagers are unintended and many can be attributed to contraception misuse or nonuse (Sharma et al., 2014) (Kalayu et al., 2015). Furthermore, women of low parity are more likely to discontinue due to desire for more pregnancy, while those with high parity were more like to continue till the time elapse.
Number of living children at the time of contraceptive use was signiï¬cantly associated with the reason for discontinuation, suggesting that women wanted to space or limit childbirth as the number of surviving children increases. The higher the number of living children the higher the possibility of adopting LARC. The desire to limit the number of children will come to play when women believe they have sufï¬cient numbers of children so rather adopting short-lasting, long-lasting methods will be better for them (Melese et al., 2017).
In addition, level of education was found to be associated with the reason for discontinuation of LARC. The possibility of women with at least secondary school education to control her reproductive need is very high. The higher the education of women the higher the propensity that they will continue the contraception till the duration elapses, and less likely to discontinue due to desire for more pregnancy. This is in line with previous study (Tadele, 2017; Azmoude et al., 2017; Biza et al., 2016; Zenebe et al. 2017; Adolescents and Long-Acting Reversible Contraception, 2012). Educated women tend to adhere more to contraception.
Furthermore, civil servants were less likely to discontinue due to desire of pregnancy and more likely to continue till the duration elapsed. This is possible because empowered women can able to control their reproductive need.
This review also found that pelvic infection, and husband refusal was other reason for discontinuation and, expulsion, weigh gain also contributed. This finding is in line with previous studies (Olson et al., 2018; Black et al., 2013; Thanel et al., 2018). Husband refusal is another barrier for contraception use. This probably may be their ignorant of the benefit of contraception in women reproductive life.
CONCLUSION
The finding in this study revealed that uptake of Jadelle and Implanon increased over the period of 2015 to 2019, but IUCD use remains low. Adolescent are less likely to use LARC. The identified reason for early discontinuation among LARC users was desire for another pregnancy, irregular menses, husband refusal, pelvic infection and weight gain. Adolescents should have access to client-friendly family planning services without bias, and stigmatization. Effective, confidential communication with sensitive language to inform adolescents of the different types of LARC is necessary to normalize offering LARC as a contraceptive option and improve its uptake among adolescents. Appropriate follow up case, management of side effects and involving men in family planning will improve the uptake and minimized the rate dis-continuation of LARC.
LIMITATIONS AND STRENGTHS OF STUDY
The study had some limitations. This study was a retrospective facility-based review of the uptake of LARC and the reason for early discontinuation. There were missing information on marital status, religion, sources of family planning information and husband education and occupation in the new client register. Such data can affect uptake rates of the methods by the clients. The study being a facility-based one cannot be generalized to all women of reproductive age for the entire study population. Postpartum LARC was not included because of limited data. Despite these limitations, this study has filled an important gap in the literature on family planning by providing evidence on the trends, uptake, and reason for discontinuation of LARC use in centers, and highlights the characteristics of uses, in an area where fertility and maternal mortality is high and the utilization of these methods has remained consistently low.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
American College of Obstetricians and Gynecologists (ACOG) (2012). Adolescents and long-acting reversible contraception: implants and intrauterine devices. Committee Opinion No. 539. American College of Obstetricians and Gynecologists. Obstetrics and Gynecology 120: 983-988. |
|
|
Adedini SA, Omisakin OA, Somefun OD (2019).Trends, patterns and determinants of long-acting reversible methods of contraception among women in sub-Saharan Africa. PLoS ONE 14(6):e0217574. |
|
|
Adolescents and Long-Acting Reversible Contraception (2012). Implants and Intrauterine Devices. ACOG Committee Decision No. 539. |
|
|
Aregay W, Azale, T, Sisay M. et al (2018). Utilization of long acting reversible contraceptive methods and associated factors among female college students in Gondar town, northwest Ethiopia, institutional based cross-sectional study. BMC Research Notes 11:862. |
|
|
Aruna S, Yellayi R, Sarada BK (2015). A Study on acceptance and discontinuation of intrauterine contraceptive device and its determinants in a tertiary care centre". International Journal of Evidence-Based Healthcare 2:3804-3811. |
|
|
Azmoude E, Behnam H, Barati-Far S, et al (2017). Factors Affecting the Use of Long-Acting and Permanent Contraceptive Methods Among Married Women of Reproductive Age in East of Iran 4(3):23-30. |
|
|
Bhandari R, Pokhrel KN, Gabrielle N, Amatya A (2019). Long acting reversible contraception use and associated factors among married women of reproductive age in Nepal. PLoS ONE 14(3):e0214590. |
|
|
Bikorimana E (2015). Barriers to the use of Long acting contraception methods among married women of reproductive age in Kicukiro District, Rwanda. International Journal of Scientific and Research Publications 5:12. |
|
|
Biza N, Abdu M, Reddy PS (2016). Long acting reversible contraceptive use and associated factors among contraceptive users in Amhara region, Ethiopia. A community based cross sectional study. Medico Research Chronicles. 4(5):469-480. |
|
|
Black KI, Lotke P, Lira J, Peers T, Zite NB (2013). Global survey of healthcare practitioners’ beliefs and practices around intrauterine contraceptive method use in nulliparous women. Contraception 88:650-656. |
|
|
Bolarinwa OA, Olagunju OS (2019). Knowledge and factors influencing long acting reversible contraceptive use among women of reproductive age in Nigeria [version 1; 3 :7[version) |
|
|
Bratlie M, Aarvold T, SkÃÂ¥rn ES, Lundekvam JA, Nesheim BI, Askevold ET (2014). Long-acting reversible contraception for adolescents and young adults - a cross-sectional study of women and general practitioners in Oslo, Norway. European Journal of Contraception and Reproductive Health Care 19:194-202. |
|
|
Coombe J, Harris ML, Loxton D (2017). Who uses long-acting reversible contraception? Profile of LARC users in the CUPID cohort. Sexual & Reproductive Healthcare 11:19-24. |
|
|
Darroch JE, Singh S (2013). Trends in contraceptive need and use in developing countries in 2003, 2008, and 2012: an analysis of national surveys. The Lancet 381(9879):1756-1762. |
|
|
Ezegwui H, Ikeako L, Ishiekwene C, Oguanua T (2011). The discontinuation rate and reasons for discontinuation of implanon at the family planning clinic of University of Nigeria Teaching Hospital (UNTH) Enugu, Nigeria. Nigerian Journal of Medicine 20:448-450. |
|
|
Francis RKJ, Melanie A, Gold AM (2017). Long-Acting Reversible Contraception for Adolescents A Review. JAMA Pediatrics 171(7):694-701. |
|
|
Igwebueze OI (2017). Uptake of Long-Acting Reversible Contraceptive Methods in Enugu State University Teaching Hospital Enugu, South-East, Nigeria. Diversity & Equality in Health and Care 13(13):216-220. |
|
|
Kalayu B, Seifu H, Magana F (2015). Early Discontinuation Rate of Implanon and its Associated Factors among Women who ever Used |
|
|
Implanon In Ofla district, Tigray, Northern Ethiopia. International Journal of Pharmaceutical Sciences and Research P 6. |
|
|
Lisa R, Pazol K, Lee Warner LG, Moskosky S, Besera G, Briceno AC, Jatlaoui T, Barfield W (2015). Vital Signs: Trends in Use of Long-Acting Reversible Contraception Among Teens Aged 15-19 Years Seeking Contraceptive Services United States, 2005-2013 MMWR Morb Mortal Weekly Report 64(13):363-369. |
|
|
Luchowski AT, Anderson BL, Power ML, Raglan GB, Espey E, Schulkin J (2014). Obstetician-Gynecologists and contraception: long-acting reversible contraception practices and education. Contraception 89:578â:583. |
|
|
Melese S, Zerfu M, Mulunesh A, Habtamu K (2017). Implanon Discontinuation Rate and Associated Factors among Women who ever Used Implanon in the Last Three Years in Debre Markos Town, Northwest Ethiopia, Cross Sectional Study. ARC Journal of Public Health and Community Medicine 2(1):8-16. |
|
|
Mohammed DA, Joel A, Bature S, Abubakar A, Mohammed C, Taingson M (2017). Uptake and Predictors of Long-Acting Reversible Contraceptives among Women in a Tertiary Health Facility in Northern Nigeria doi: 10.4103/2278-960X.194504. |
|
|
Moreau C, Bohet A, Hassoun D, Teboul M, Bajos N, FECOND Working Group (2013). Trends and determinants of use of long-acting reversible contraception use among young women in France: results from three national surveys conducted between 2000 and 2010. International Journal of Fertility and Sterility 100:451-458. |
|
|
Mukamuyango J, Ingabire R, Parker R, Nyombayire J, Easter SR, Wall KM, Tichacek A, Nyirazinyoye L, Kaslow N, Allen S, Karita E (2014). Motivational interviewing to promote long-acting reversible contraception among Rwandan couples wishing to prevent or delay pregnancy. American Journal of Obstetrics and Gynecology 30:20-20. |
|
|
National Population Commission (2018). Population and housing census of the Federal Republic of Nigeria: priority tables volume 1. Abuja: National Population Commission |
|
|
National Population Commission and ORC/Macro. National Population Commission/Federal Ministry of Health (2018). Population and the quality of life in Nigeria. Abuja: National Population Commission. |
|
|
Nicole M, Pritt BA, Alison HN, Berlan DE (2017). Barriers and Facilitators to Adolescents' Use of Long-Acting Reversible Contraceptives Journal of Pediatric and Adolescent Gynecology 30(1):18-22. |
|
|
Ochako R, Izugbara C, Okal J, Askew I, Temmerman C (2016). Contraceptive method choice among women in slum and non-slum communities in Nairobi, Kenya. BMC women's health. 16(1):35. |
|
|
Ochako R, Mbondo M, Aloo S, Kaimenyi S, Thompson R, Temmerman M, Kays M (2015). Barriers to modern contraceptive methods uptake among young women in Kenya: a qualitative study. BMC Public Health 15:118, |
|
|
Olson EM, Kramer RD, Gibson C, Wautlet CK, Schmuhl NB, Ehrenthal DB (2018). Health Care Barriers to Provision of Long-Acting Reversible Contraception in Wisconsin. WMJ 117(4):149-155. |
|
|
Sharma M, Joshi S, Nagar O, Sharma A (2014). Determinants of Intrauterine Contraceptive Device Discontinuation Among Indian Women. Journal of Obstetrics and Gynecology of India 64:208-211. |
|
|
Staveteig S, Mallick L, Winter R (2015). Uptake and Discontinuation of Long Acting Reversible Contraceptives (LARCs) in Low-Income Countries. DHS Analytical Studies No. 54. Rockville, Maryland, USA: ICF International. |
|
|
Tadele GA (2017). Early Discontinuation of Long Acting Reversible Contraceptives among Married and in Union Women: A Systematic Review and Meta-analysis. Annals of Medical and Health Science Research 7:113-118. |
|
|
Thanel K, Garfinkel D, Riley C, Esch K, Girma W, Kebede T, et al (2018). Leveraging long acting reversible contraceptives to achieve FP2020 commitments in sub-Saharan Africa: The potential of implants. PLoS ONE 13(4):e0195228. |
|
|
The American College of Obstetricians and Gynecologists (2014). Committee on Gynecologic Practice, Long-Acting Reversible Contraception Working Group. Increasing use of contraceptive implants and intrauterine devices to reduce unintended pregnancy (opinion no. 450). |
|
|
Thompson CM, Broecker J, Dade M, Nottingham K (2018). Influences on Intentions to Place Long-Acting Reversible Contraceptives: A Pilot Study Comparing According to Provider Specialty in Ohio. Journal of Pediatric and Adolescent Gynecology. 5: 509-515. |
|
|
Usman NO, Abdullahi HM, Nmadu AG, Omole VN, Ango JT (2019). Estimation of maternal mortality by sisterhood method in two rural communities in Kaduna State, Nigeria. Journal of Tropical Medicine 21:62-66. |
|
|
World Health Organization, UNICEF, United Nations Population Fund and the World Bank (2019). Trends in Maternal Mortality: 2000 to 2017 WHO, Geneva, 2019. |
|
|
Zenebe CB, Adefris M, Yenit MK, et al (2017). Factors associated with utilization of long-acting and permanent contraceptive methods among women who have decided not to have more children in Gondar city. BMC Womens Health 17(1):75. 10.1016/j.pedhc.2018.02.009. Epub. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


