Full Length Research Paper

ABSTRACT
The aim of this work is to report the clinical presentation and management of pregnancy epulis (PE) among pregnant women that attended ante-natal clinic in Barau Dikko Teaching Hospital, Kaduna, Northern, Nigeria. Three hundred and twenty self-administered, structured questionnaires were administered to pregnant women that attended ante-natal clinic in Barau Dikko Teaching Hospital, Kaduna. Intraoral examination was done for all that filled the questionnaire. The study was done from January 2018 to July 2018. Eight cases (2.5%) of pregnancy epulis were diagnosed among 320 pregnant women. The age of the women ranged between 23 to 34 years with mean age ±28.5 years (SD=3.9); four (50%) were in their third trimester, three (37%) in their second trimester and one (12.5%) was in her first trimester of pregnancy. Five (62.5%) occurred in the anterior gingiva of the maxillary teeth, and two (25%) mandibular anterior gingivae and one (12.5%) at the mandibular posterior gingivae. The prevalence of PE from this study was one pregnant woman among forty, ratios 1:40. Our treatment modalities included: Oral hygiene prophylaxis and surgical excision of the tumour under local anaesthesia. There is need to pay attention to plaque control in pregnant women to reduce the incidence and prevent complications that may arise from the tumour such as life threatening haemorrhage. All pregnant women should have routine oral hygiene prophylaxis to reduce incidence of pregnancy epulis.
Key words: Pregnancy, epulis, gingivae, women, tumour, Kaduna.
INTRODUCTION
Pregnancy epulis is a tumour like growth of the gingivae that is non-neoplastic in nature (Sooriyamoorthy and Gower, 1989). It is a pyogenic granuloma that occurs on the gingivae during pregnancy (Sooriyamoorthy and Gower, 1989). It was originally reported in 1897 by two French Surgeons Poncet and Dor (Courtney et al., 2003). The tumour developed due to irritation or physical straining from calculus or cervical restorations. Also some contributions from hormonal factors usually affect the gingivae. Areas of frequent trauma such as lower lip, tongue, oral mucosa and palate are also affected (Courtney et al., 2003). The growth is typically seen on or after the third month of pregnancy and occurs in up to 5% of pregnancies (Soyele et al., 2019. The gingivae is more often involved, followed by the tongue, lips and buccal mucosa (Ye et al., 2019).
However, the lesion has been described as painless, erythematous and exophytic. It could be smooth surfaced or lobulated and there may be a fibrinous covering (Fonseca et al., 2014). It most frequently develop on the buccal gingivae in the interproximal tissue between teeth, the base usually extends from the gingival margin and in most instance in the maxillary anterior teeth (Ye et al., 2019). The lesion usually bleeds easily on the slight provocation (Ye et al., 2019).
The tumour could be quite frightening to the patient, sometimes affecting chewing or be misdiagnosed as a malignancy especially as the lesion has high tendency to recur if excised before delivery, and if not completely excised (Ye et al., 2019). It is also an uncommon gingivae tumour in pregnancy and could be life threatening due to severe haemorrhage from the tumour.5Therefore; we report eight cases among pregnant women that attended antenatal clinic at Barau Dikko Teaching Hospital, Kaduna in Northern Nigeria.
MATERIALS AND METHODS
The study was carried out at the antenatal clinic of BarauDikko Teaching Hospital, from January 2018 to June 2018. The hospital is a tertiary center in North-west Nigeria. All pregnant women attending the antenatal clinic for the first time in the hospital and consented to participate in the study were included. Pretested, structured and interviewer-administered questionnaires allowing open and closed responses were used for data collection. Information collected includes information on demographics, reproductive characteristics, and information relating to oral health. Intra-oral examinations were also performed by the dental surgeon and trained dental nurses to check for oral health status and oral diseases. Referrals were made to the dental clinic as required. Yaro (1967)’s formula was used to calculate the sample size.

Where:
n= Sample size (unknown), N= Population = 1,600, I= Constant, e=Margin of error = 5%=0.05
The data were analyzed using the SPSS for window’s (version 11.0; SPSS Inc Chicago)
Ethical issue
Permission was obtained from the BarauDikko Teaching Hospital, Kaduna, Nigeria; ethical committee and written informed consent was obtained from the women, including permission to use their pictures anonymously.
RESULTS
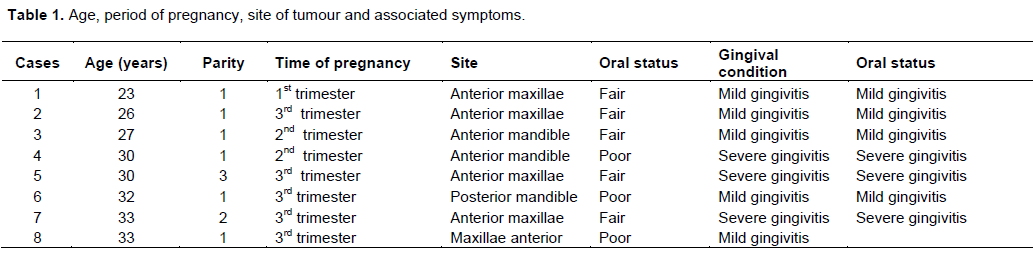
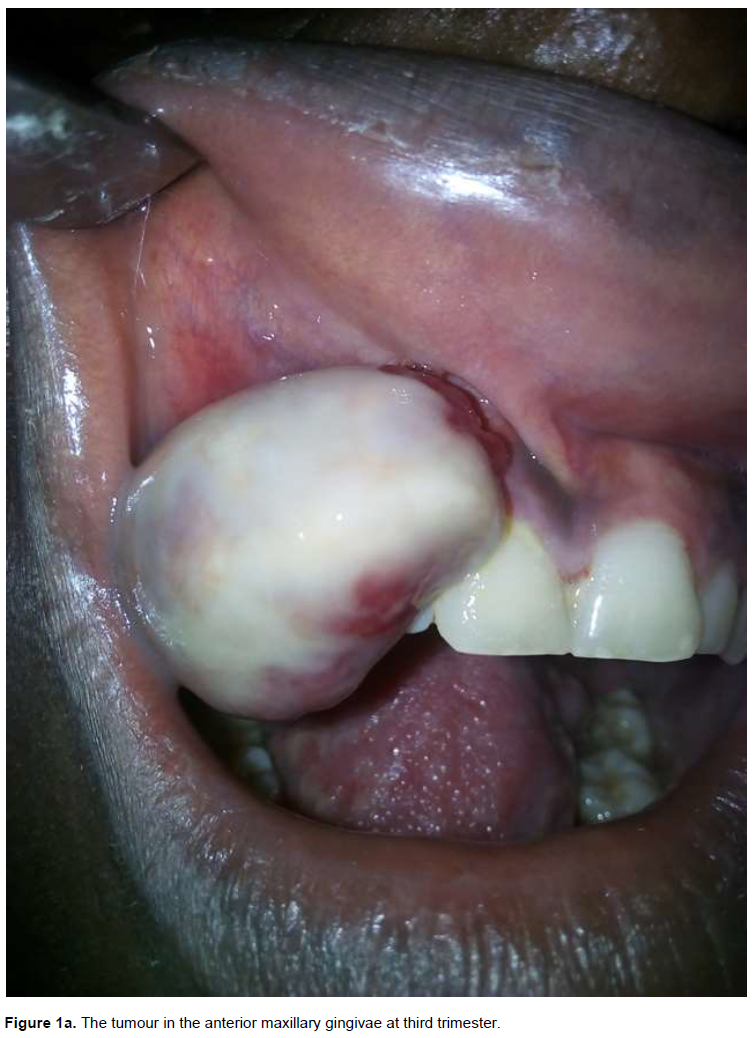
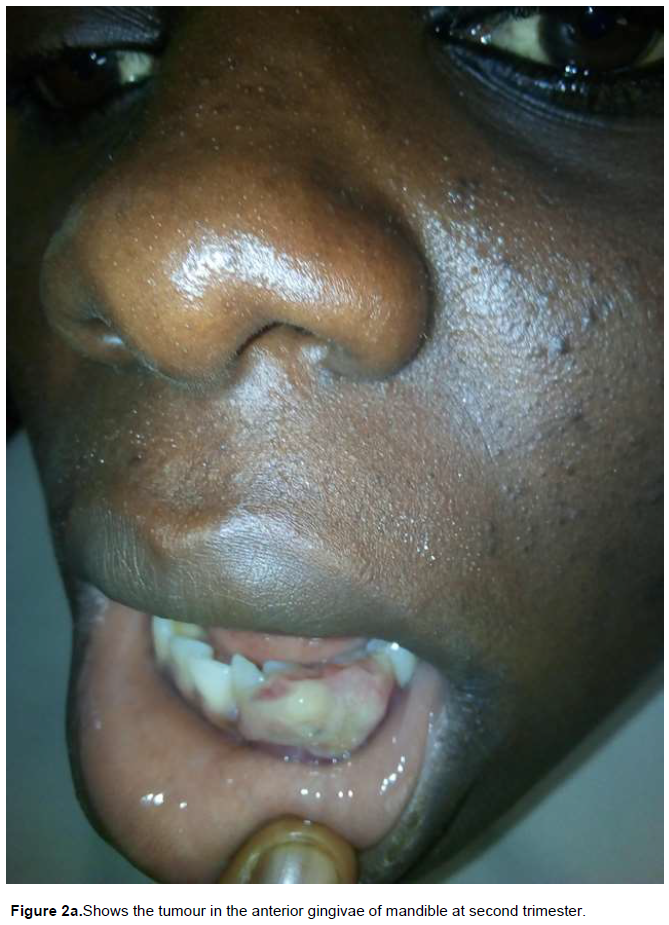
Among the 320 pregnant women seen for antenatal care, thirty-five were referred to the dental clinic of whom eight were diagnosed with pregnancy epulis. All the cases of PE showed evidence of gingivitis which ranged from mild to severe. At the time of diagnostic, their sizes ranged from 2 to 8 cm at the widest dimension, with mean size of ± 5cm (SD=2). We got eight samples for histological examination. The prevalence rate of the tumour is one in forty pregnant women (1:40). The age range of the women was from 23 to 33 years with mean age of ± 29 years (SD=3.9) (Table 1). The tumour occurred mostly on the anterior maxillary gingivae (n=5, 62.5%) (Figure 1a) then mandibular anterior gingivae (n=2, 25%) (Figure 2a) and one at the mandibular posterior gingivae (n=1, 12.5%). Our diagnosis of PE was based on clinical evaluation of the location of the tumour in the interproximal surface between teeth and tendency to bleed on slight provocation and association with pregnancy. The tumour mass was fixed in 10% neutral buffered formalin solution and embedded in paraffin. Five-micrometer sections were obtained and submitted for routine haematoxylin and eosin staining. Histological finding confirmed our diagnosis. The tumour was managed conservatively. Routine oral hygiene prophylaxis was administered to reduce irritants at the gingival margin. The tumour regressed post parturitionin all the women with sizes ranged from 1 to 6cm with mean size of ± 3.5cm (SD=1.7) at the widest dimension; the remnants were excised under local anaesthesia. Six months follow up showed no recurrence in all women.


Histopathological report
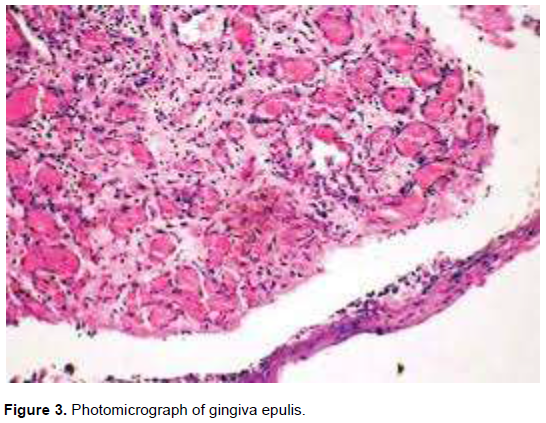
Two histological types were reported from our cases; one type is characterized by proliferating blood vessels that are organized in lobular aggregates, no inflammatory granulation tissue reaction. This was diagnosed as lobular capillary haemangioma. Only case 6 exhibited these features. The second is non-lobular capillary haemangioma or granulomatous type. This showed vascular proliferation that resembles granulation tissue; typically chronic inflammatory cells were seen (Figure 3). Seven of our cases exhibited these features.
DISCUSSION
Pregnancy epulis occurs in 0.48 to 5% of pregnant women (Soyele et al., 2019), our study showed 2.5% occurrence among pregnant women. The gingiva is involved in 70% of cases followed by the tongue, lips and buccal mucosa (Ye et al., 2019). The eight cases reported here occurred in the gingivae. It usually occurs at the end of the first trimester and rapid growth usually accompanies the steady increase of circulating estrogens and progesterone (Ye et al., 2019). One case occurred in the first trimester while two occurred in second trimester and five at the third trimester (Table 1). Partial and complete regression is common after child birth (Fonseca et al., 2014). All the women had remarkable regression after delivery from mean size of ±5cm to ±3.5 cm at the widest dimension. It rarely exceeds 2 cm in size and has a tendency to recur, if not completely excised (Regezi et al., 2003). In our study cases 7 and 8 were 4-8 cm in diameter (Figure 1a) while all others were 2-3 cm (Figure 2a).
Gestational steroid changes, accompanied with the presence of irritants such as calculus which could exacerbate inflammatory response, leading to the development of this proliferating lesion (Jafarzadeh et al., 2006). Oral examination of our cases showed mild calculus accumulation. Therefore, an exaggerated gingival response could have provoked the growth of the tumour due to increase in level of estrogen and progesterone (Soyele et al., 2019; Ye et al., 2019; Fonseca et al., 2014; Regezi et al., 2003). Our cases were assured that the tumour will regress and be excised after delivery.
The precise mechanism for the development of PE is unknown but trauma, hormonal influence, viral oncogenes, underlying microscopic arterio-venous malformations, the production of angiogenic growth factors and cytogenic abnormalities have been postulated to play a role (Azodo and Erhabor, 2017). Our study noted gingival irritation from bacterial plaque to be a major factor in the onset of the tumour.
However, bacterial plaque and gingival inflammation are necessary for subclinical PE which causes much alteration leading to gingivitis (Azodo and Erhabor, 2017). Pregnancy epulis is a result of gingivitis that leads to local hyperplasia (Taiwo et al., 2010). All the cases reported showed evidence of gingivitis which ranged from mild to severe. The severity of gingivitis was not directly related to oral hygiene status (Table 1). There were exaggerated gingival inflammation to mild irritation from dental plaque and calculus. The tumour bleeds on slight provocation (Azodo and Erhabor, 2017). Three of our cases bleed during tooth brushing and on slight provocation during oral examination (Cases 4, 5, 7). Taiwo et al. (2010) reported that haemorrhage resulting from pregnancy epulis could be life threatening, however, none of our cases presented with any haemorrhage.
Clinically, the lesion is painless, erythematous, exophytic which could be smooth or lobulated which may have a fibrinous covering (Soyele et al., 2019). All our cases were painless, erythematous and exophytic. Five were smooth surfaced and sessile, three were lobulated and pedunculated. Younger tumours are soft in consistency, progressing to a rubbery texture on maturation (Taiwo et al., 2010).The colour may range from pink to bright red to purple or brown (Jafarzadeh et al., 2006). Our cases showed variation in colour from pink to bright red; case 2 showed fibrin covering the tumour (1a). Pregnancy epulis most frequently develop on the buccal gingivae in the interproximal tissue between teeth (Ye et al., 2019; Fonseca et al., 2014). All our cases had the tumour on the buccal gingivae (Figure 2a). Human gingivae contain receptors for estrogens and progesterone and increased plasma levels results in an increase in accumulation of these hormones in gingival tissue (Taiwo et al., 2010).
It had been reported by several authorities (Ye et al., 2019; Fonseca et al., 2014; Regezi et al., 2003; Jafarzadeh et al., 2006; Azodo and Erhabor, 2017; Taiwo et al., 2010; Tsai et al., 2015) that the histology showed proliferating vascular channels, immature fibroblastic connective tissue, scattered inflammatory cells. Our cases showed two histological types, granulomatous (Figure 3) and lobular capillary haemangioma. Majority of our cases were granulomatous type. This agreed with findings of Regezi et al. (2003); Jafarzadeh et al. (2006); Azodo and Erhabor (2017); Taiwo et al.(2010); Tsai et al.(2015) and Nambiar et al. (2016). However, recently alternative conservative treatments such as cryosurgery, laser surgery, injection of absolute ethanol and sodium tetradecyl sulfate, cryotherapy, transarterial embolization have been used in treating epulis, but excisional surgery still remains the most common therapy for epulis (Azodo and Erhabor, 2017; Taiwo et al., 2010; Tsai et al., 2015; Nambiar et al., 2016). All our cases underwent conservative surgical excision after delivery and none reoccurred after six month of follow up.
CONCLUSION
Pregnancy gives an opportunity to disseminate oral hygiene knowledge to women and ensure compliance, because this period women are motivated to adopt healthy behaviours. Therefore this important period must be utilized to educate pregnant women about oral health. It is recommended that oral health care should be an integral part of antenatal care in hospitals.
RECOMMENDATION
Oral health care should be an integral part of antenatal care in the hospitals.
ACKNOWLEDGEMENT
The authors appreciate the Dental Staff, and Nurses in our ante-natal clinic for their role in the various processes of the study.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Azodo CC, Erhabor P (2017). Discrete enlargement gingival enlargement resulting from artificially created maxillary midline diastema. Journal of Clinical Sciences 14:49-50. |
|
|
Courtney MJ, Koleda C, Titchener G (2003). Aural granuloma gravidarium. Otolaryngology Head Neck Surgery 129:149-51. |
|
|
Fonseca MG, Fonseca MP, Cantin M (2014). Massive fibrous epulis- a case report of 10 -year-old-lesion. International Journal of Oral Sciences 6(3):182-184 |
|
|
Jafarzadeh H, Sanatichani M, Mohtasham N (2006). Oral pyogenic granuloma: A review of literature. Journal of Oral Science 48:167-75. |
|
|
Nambiar S, Hallikeri K, Anehosur V, Rai P, Hegde V (2016). Large recurrent gingival growth in the maxilla: A case report. Journal of the Scientific Society 43:92-95. |
|
|
Regezi JA, Scrubba JJ, Jordan RC. Oral pathology (2003): Clinical pathologic considerations. 4th ed. Philadelphia: WB Saunders,.pp 115-6. |
|
|
Sooriyamoorthy M, Gower DB (1989). Hormonal influences on gingival tissue: Relationship to periodontal disease. Journal of Clinical Periodontology 16:201-8 |
|
|
Soyele OO, Ladeji AM, Adebiyi KE, Adesina OM, Aborisade AO et al (2019). Pattern of distribution of reactive localized hyperplasia of oral cavity in patients at a tertiary health institution in Nigeria. African Health Sciences 19(1):1687-1694. |
|
|
Taiwo OA, Adeyemo WL, Ladehinde AL, Ajayi OF, Umeizuelike k et al (2010). Pregnancy epulis associated with life haemorrhage in a Nigeria woman. Nigeria Quarterly Journal of Hospital Medicine 20(1):10-2 |
|
|
Tsai KY, Wang WH, Chang GH, Tsai YH (2015). Treatment of pregnancy associated oral pyogenic granuloma with life threatening haemorhage by transarterial embolization. Journal of Laryngology and Otology 129:607-10. |
|
|
Ye C, You M, Cheng G, Zhao L, Huang P (2019). A puzzling pregnancy epulis with aggressive loss mimicking malignant neoplasm.A case report. Journal of Oral and Maxillofacial Surgery 6(5):204-209. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


