Full Length Research Paper

ABSTRACT
The use Dental radiographs has become an integral part of modern clinical dentistry to investigate complaints of patients. This study aimed at determining the level of awareness of dental radiological examination among patients attending dental treatment at the Muhimbili University of Health and Allied Sciences (MUHAS) dental clinic in Dar es salaam, Tanzania. This was a descriptive cross-sectional study, which included patients who underwent radiological examination. A specially designed questionnaire was used to gather information on the demographics and level of awareness of the patients regarding X-ray examination. The data obtained was analyzed using the Statistical Package for Social Science-V23. The association between variables was assessed by the Chi-square test, and p-value was set at p<0.05. A total of 322 participants were included in the study of which 184 (57.1%) were females. The age range of the participants was 18 to 89 years (mean of 37.2 ± 15.2 years). There was a statistically significant association between self-perceived awareness about dental radiographs and level of education, age and previous experience of the participants. Only 39.4% reported to have had some information regarding dental X-rays and among them, in 89%, the source was dental personnel. Only 36% said there was no problem in exposing a pregnant woman to dental X-rays. 92.7% said there is a need of using special protective gear when exposing a pregnant woman to dental X-ray. Generally, there was a low awareness of dental X-ray examination in this group of patients.
Key words: Awareness, dental X-ray examination, Muhimbili, Tanzania.
INTRODUCTION
Dental radiological examinations are usually employed to investigate some definite complaint of a patient, todetect the extent of disease or in screening to prove or rule out the presence of a disease where physical signs or symptoms are not clearly apparent. Their use has become an integral part of modern clinical dentistry with some form of radiographic examination necessary on a good proportion of patients in daily dental practice (Hamza et al., 1998; Msagati et al., 2013; White et al., 1994; Matee and Simon, 2000). In general dental practice in developing countries about 10% of dental patients undergo radiological examination (White et al., 1994; Matee and Simon, 2000).
The trend may be a bit different in developed countries because of the differing demands that is, some sophisticated treatment modalities including orthodontic reasons, endodontic treatment, dental checkups, implants placement and general medical/dental examination (Wenzel and Møystad, 2010; Berkhout et al., 2003). In a previous study in Tanzania, the main reasons for taking dental X-rays were diagnosis of dental caries and associated lesions, fractures, investigating tumours, periodontal diseases among others (Hamza et al., 1998). Examples of dental radiographs include bitewings, periapical, orthopantomograms, upper or lower standard occlusal, hand-wrist radiographs, and temporomandibular joint radiography (Murage, 2001). The advent of new technologies in the form of digital radiography and advanced treatment modalities like implantology might have modified to a certain extent utilization of X-rays in the wide range of dental treatments (Wenzel and Møystad, 2010; Berkhout et al., 2003; Shahab et al., 2012).
Although dental radiology has a great importance in dentistry, it also has associated health effects. Repeated exposure to dental X-rays may result in various health problems including head and neck tumors and various systemic problems (Hwang et al., 2018). In Tanzania, there is paucity of information on patients’ awareness of dental radiography, its importance and associated effects in individual’s general health. The only available studies on X-ray examination was on the utilization of dental services and reasons for taking radiographs in the school of dentistry (Hamza et al., 1998; Matee and Simon, 2000). These studies were carried out more than 15 years ago when the utilization of dental radiographs was found to be 9.48% of all patients who were attended. During that time the number of dental practitioners and correspondingly the number of attended patients were moderately low. Furthermore, the type of treatment procedures that were available then was limited to oral surgical procedures and restorative care. With sophisticated treatment procedures like implantology and orthodontic treatments gaining popularity in daily dental practice in Tanzania, the need for X-ray examination have similarly increased. In 2011, a study was done in Kenya among 172 patients visiting the university of Nairobi dental hospital in which 97.7% were found to have knowledge on uses of X-rays, while 79.1% had knowledge about scatter of X-rays to unintended areas of the body during taking of X-rays (Murage, 2001). Furthermore, all of the respondents thought that X-rays could improve the management of their dental problems. Also, a study done in Malaysia showed that most patients neither had a clear understanding why X-rays were taken nor did they know their benefits (Aravind et al., 2016). A study in Australia showed that most (41%) parents displayed a low level of knowledge, but had positive attitude towards dental radiographs (Kelaranta et al., 2015).
In the recent past the Tanzanian government made tremendous efforts in improving the provision of oral health services. Such measures included equipping the regional and district dental clinics with new and modern dental units and dental X-ray machines. Despite the increase in the number of both public and private dental clinics with the capability to order and take X-rays, information on patients’ level of awareness on dental X-ray examination is completely lacking. The aim of this study therefore was to assess the level of awareness on dental X-ray examination and associated factors among patients attending MUHAS Dental clinic.
MATERIALS AND METHODS
Type of study and setting
This was a descriptive cross-sectional study conducted at the Muhimbili University of Health and Allied Sciences (MUHAS) dental clinic, Dar-es-Salaam, Tanzania from September to November 2018.
Sampling
It included all patients who were to undergo X-ray examination at the MUHAS Dental clinic during the study period. Patients who did not consent, failed for one reason or another to answer questions coherently, and those who had dental radiological investigation done within past 5 years were excluded from the study.
Data collection
A structured questionnaire (which was validate by an expert in the field of dental radiology) was used to collect relevant information on the social-demographics factors, the provisional diagnosis, type of X-ray and level of awareness on dental X-ray examination and use of dental X-rays for age determination. Each participant was interviewed separately by the researchers immediately after undergoing dental radiograph investigation. Quality assurance was carried out by blindly repeating some of the participants every day of the study.
Data analysis
Information gathered was entered into computer and data was processed and analyzed using version 23 of Statistical Package for Social Science (SPSS). Age was dichotomized into those who were 40 years or younger and those who were above 40 years. Education level was dichotomized to those who had primary school education or below (low level) and those who had above primary school education (high level). Chi-square test was used to look for association between the different independent variables whereby the p-value was set at p<0.05.
Ethical approval
The study was approved by the Institutional Review Board of the Muhimbili University of Health and Allied Sciences (MUHAS). Participation was voluntary and each participant was given detailed information on the study, before they signed a written informed consent form to agree to participate. The participants were assured of confidentiality and their right to participate or withdraw without any conditions. No names were used, to avoid identification.
RESULTS
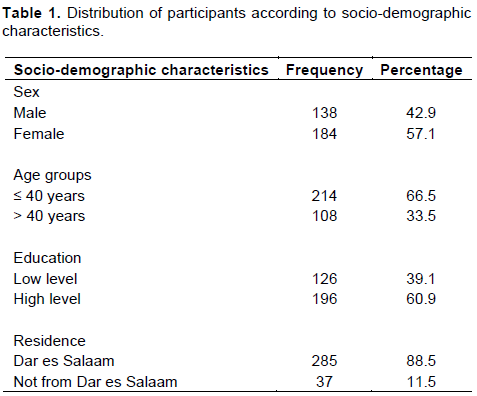
A total of 322 patients who underwent dental radiological investigations were included in the study. Females were 184 (57.1%) and the male to female ratio was 1:1.4. The age range of the participants was 18 years to 89 years with a mean of 37.2 ± 15.2 years. The age group ≤ 40 years had more (66.5%) participants. About 60% of the participants had high level of education. The majority (88.5%) of participants were from Dar es Salaam (Table 1).
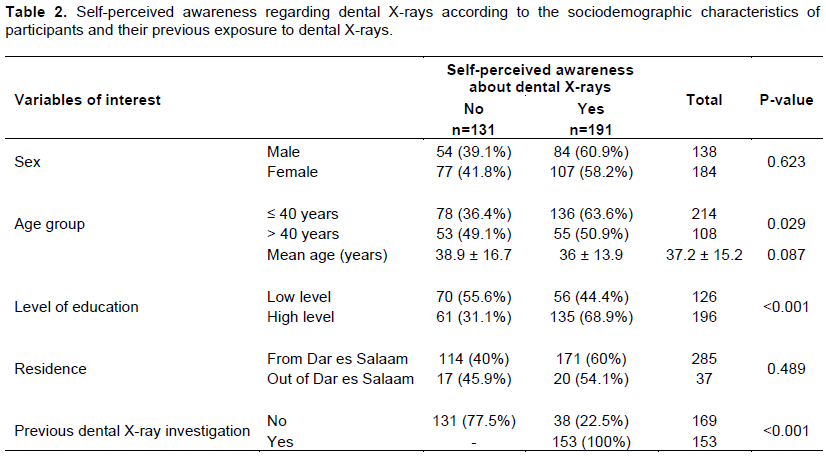
The periapical X-ray was ordered in 211 (65.5%) participants, orthopantomograms in 93 (28.9%) and in the remaining 18 (5.6%) participants, both OPG and PA X-rays were ordered (Figure 1). Out of 191 (59%) participants who reported to have heard about dental X-rays before, 153 (80.1%) had undergone dental radiological investigations in the past. There was a statistically significant association (p < 0.05) between self-perceived awareness about dental X-rays and level of education, age and previous experience of the participant (Table 2).
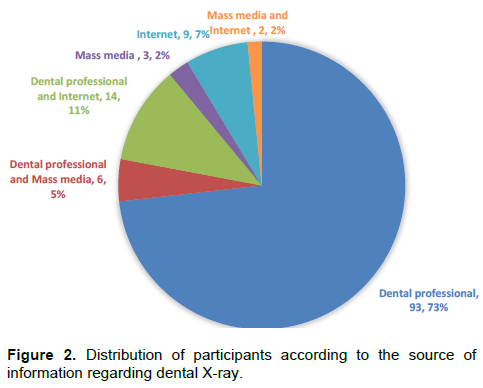
Only 127 (39.4%) participants reported to have had information regarding dental X-rays and among them, in 113 (89%) participants the source was dental personnel (Figure 2). When the participants were asked about the use of dental X-rays, most (122, 37.9%) said it was for helping the doctor to confirm a diagnosis. Other reasons were that it was for both diagnosis and treatment (114, 35.4%) or it was a form of treatment (52, 16.1%).
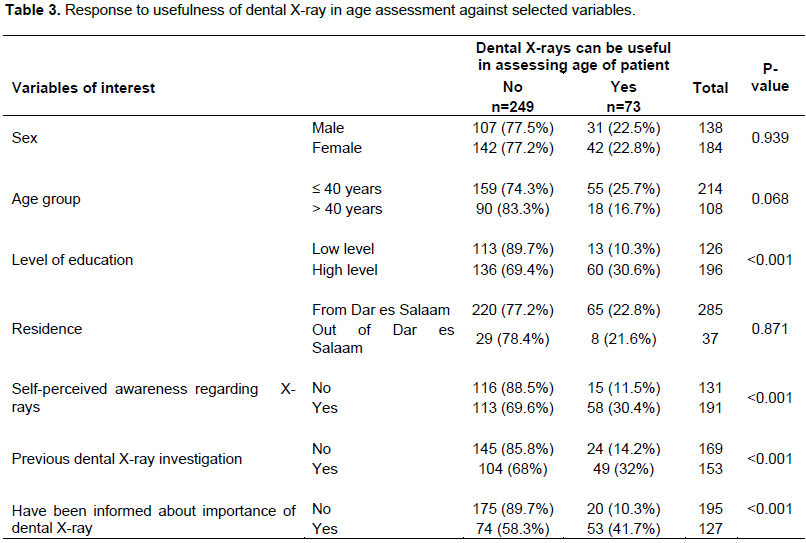
A few (22.7%) participants knew that dental X-rays can be useful in assessing the age of a patient. There was a statistically significant association (p < 0.05) between knowledge that dental X-rays may be used to assess patients’ age and participants’ level of education, self-perceived awareness, previous experience of having dental X-rays taken and having been informed about dental X-rays (Table 3).
Regarding exposing a pregnant woman to dental X-ray, 116 (36%) participants said there was no problem in doing so, and among these 107 (92.7%) said there is a need of using special protective gear when a pregnant woman is exposed to dental X-ray. The majority (96%) of participants had the notion that it was harmful to an unborn child when a pregnant woman was exposed to dental X-rays.
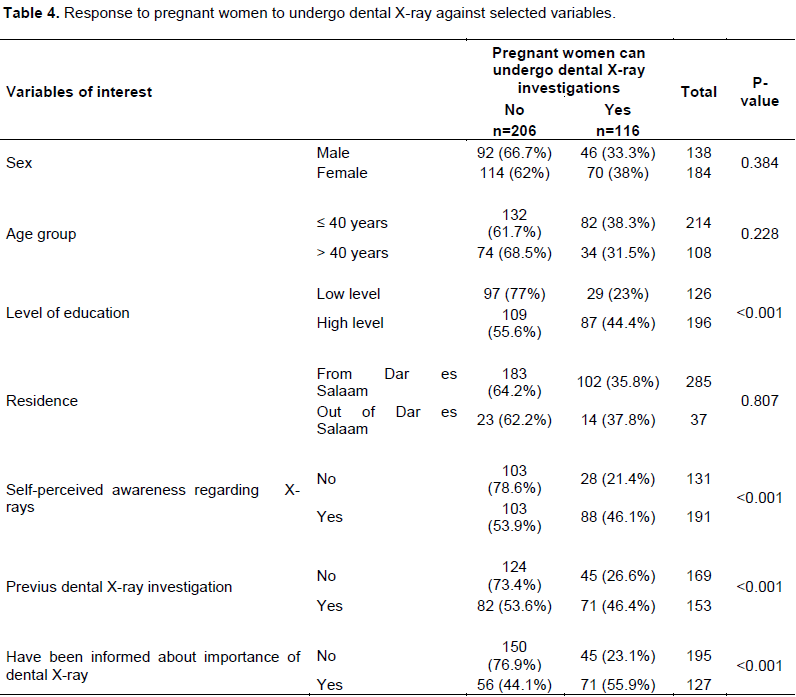
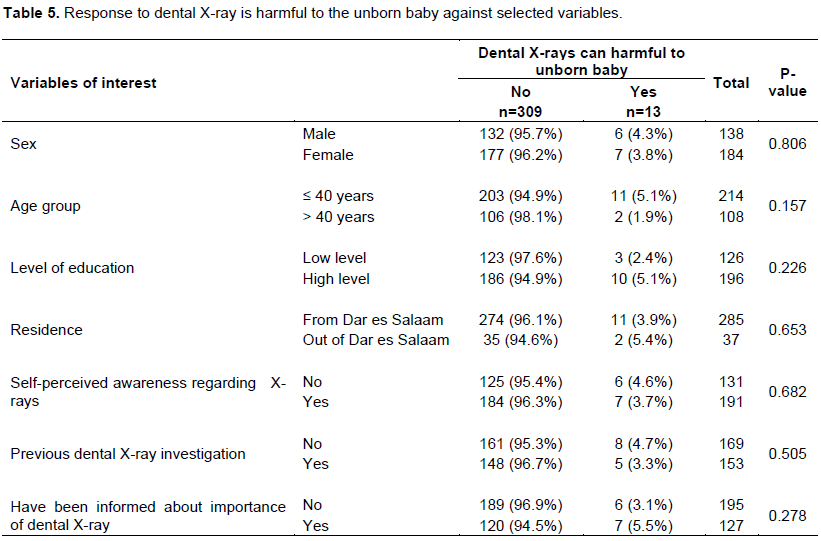
There was a statistically significant association (p < 0.05) between knowledge that dental X-rays can be taken in pregnant patients and the participants’ level of education, self-perceived awareness, previous experience of having dental X-ray taken and having been informed about dental X-rays (Table 4). Knowledge that dental X-rays cannot be harmful to the unborn child was very low, and there was no statistically significant association between the difference in knowledge on the particular matter with the sociodemographic characteristics of patients, their self-perceived awareness, previous experience of having dental X-ray taken and having been informed about dental X-rays (Table 5).
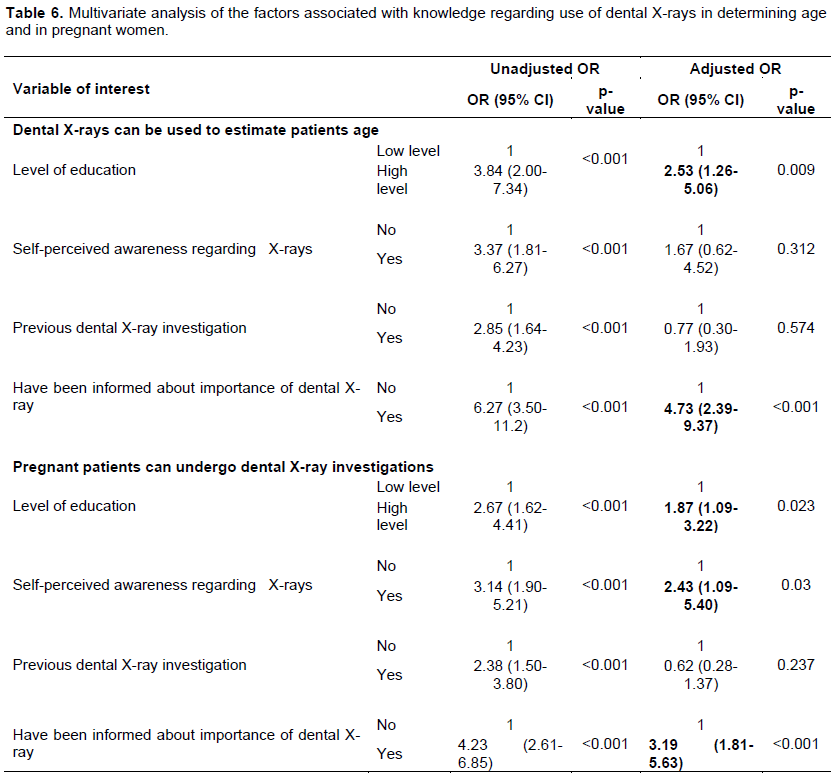
The multivariate logistic regression analysis for factors associated with knowledge that pregnant patients can undergo dental radiological investigation showed a significant association with level of education of the participants, self-perceived awareness and having been given previous information regarding dental X-rays. On performing multivariate logistic regression analysis for factors associated with awareness about dental X-rays, the odds of participants with a high level of education to have awareness about dental X-ray was 2 times more than that of participants with a low level of education (Table 6).
DISCUSSION
This study was conducted in patients who were attended at the clinics of the School of Dentistry which is the biggest oral health unit in the country with different specialties. There are more patients who undergo dental X-ray examination in this institution than any other in the whole country. Clients who are attended in this unit include referred patients from other clinics in the city and upcountry hospitals. Interview was chosen as the best approach in this type of study because the patients attended are of different social backgrounds including some with minimum levels of education who needed help in understanding the questionnaire.
The higher number of female participants in this study is supported by the fact that generally majority of the patients attending for service in this clinic are females. The age group ≤ 40 years had the highest number of participants. This corresponds well with studies which had shown that the majority of patients with dental caries, which is the main reason of taking X-rays (qv) were young (Matee and Simon, 2000). The fact that majority of the patients had attained education levels of secondary school and above may be explained by the urban nature of the population. Nevertheless, only 24% had attained college education. Regarding the place of domicile, majority (59%) of the participants was from Dar es Salaam region, and the rest were mainly referrals from different regions some as far away as the lake zone regions.
Only fifty-nine percent of the patients had heard of X-rays before. This is different from developed countries where in similar studies higher percentages of the patients had heard of X-rays (White et al., 1994; Murage, 2001; Aravind et al., 2016; Newman et al., 2009). This might have some more implications on the level of knowledge displayed by the patients on different aspects of X-rays in this study. The source of information on X-rays for about one third of the participants who responded that they had heard of X-rays before was dental professionals. Very few of the patients mentioned the media as their source of information on X-rays. In studies elsewhere mass media including television were mentioned by a considerable number of patients as the main source of information on dental X-rays (Kelaranta et al., 2015; Chiri et al., 2013; Abbott, 2000).
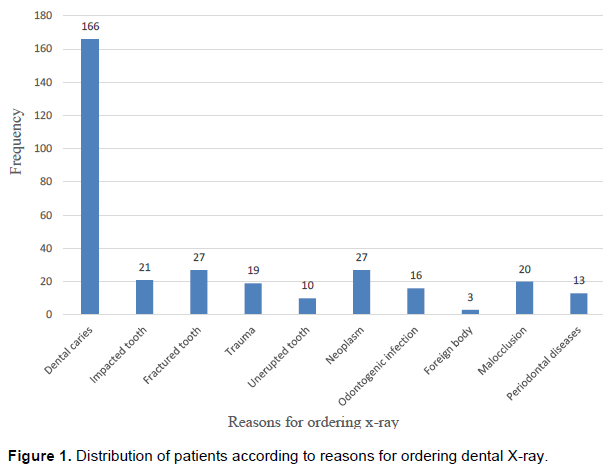
Most (51%) of the patients had never had any X-rays taken before. However, in comparison with those who have had X-rays done before, the difference was not significant. In Kenya, the number of patients who had X-rays done before was much higher than that of this study. This might explain the differences in awareness between these two groups of patients. The main reason for ordering X-rays was dental caries in 166 (51.6%) of the patients followed by fractures of teeth and general trauma. Hamza et al. (1998) in their study on reasons for taking X-rays in the same setting similarly reported dental caries as the main reason for ordering X-rays (Hamza et al., 1998). This is germane to available information that majority of dental visits in public dental clinics in Tanzania are due to dental caries (Matee and Simon, 2000). Also, some modalities of treatment of advanced dental caries like endodontic treatment necessitate multiple exposures of the same tooth during the same visit or during subsequent visits. When considering the different types of X-rays separately, for periapical view dental caries still remained the main reason for ordering this type of X-ray, however, for the OPG tumors, malocclusion and trauma were the main reasons for ordering X-ray. This is mainly because in these conditions the clinicians intend to visualize larger areas of the jaws rather than a single or few teeth in order to reach a plausible diagnosis and consequently arrive at a good treatment plan. In situations where both PA and OPG had to be ordered, the main reason still remained dental caries most possibly intended for visualizing several teeth in the region of interest. Nevertheless, this information is slightly different from studies from some developed countries where OPGs were mostly used for dental caries (White et al., 1994; Newman et al., 2009). Dental caries is a condition in which exposure of a single tooth is adequate to show most of the information necessary for reaching the diagnosis and drawing appropriate treatment plan. Further, endodontic treatment which is mostly done because of dental caries often requires several radiographs of the same tooth during the course of treatment which may entail several sessions. This may seem to be disadvantageous to the patient but it has the big advantage of limiting cost and minimized exposure compared to the extra oral views that expose larger areas. The OPG, on the other hand, is usually done once, mainly for diagnosis and treatment plan and the same radiograph can be used during several subsequent visits. Multiple exposures for OPG, however, are often ordered in situations where control X-rays are needed after a treatment procedure, such as during treatment of fractures or reconstruction of the jaws. Also, because the periapical radiograph can accommodate one or two teeth only, in patients with several teeth that require treatment it is necessary to order an OPG.
On the level of knowledge on why X-rays are taken, 37% of the participants knew that it was for diagnostic purposes, 35% thought it was for both diagnosis and treatment and 16% thought that it was a form of treatment. There were only few who did not know completely the purpose of taking X-rays. These findings differ from studies in Kenya and Malaysia where majority of patients who were interviewed actually knew the reasons for ordering of X-rays (Murage, 2001; Aravind et al., 2016). This difference might be attributable to regular visits to the dental clinic in those countries compared to Tanzania where majority of the patients attend for dental treatment on emergency basis. It is also possible that patients in those countries have better exposure to sources of information on dental treatment compared with Tanzanian patients. The level of education in the group of patients in this study was generally low which might have also contributed to the low level of awareness on matters related to X-ray examination. The majority (49.7%) of the study participants did not know whether X-rays can be used to estimate the age of an individual. This low level of knowledge on the different uses of X-rays was possibly attributable to lack of exposure in form of dental checkups and lack of sources of information to the majority of the population.
On whether X-rays can be ordered for pregnant women a slight majority (36%) agreed while an almost equal number either disagreed (32%) or did not know (31%). These results are different from findings by others who have postulated that if there was a clinical justification pregnant mothers could be exposed to X-rays (Purmal et al., 2013). A great majority (72%) of those who responded that X-rays can be ordered for pregnant women also preferred to have special protection for the pregnant women who were to undergo X-ray examination. Strangely the majority of the participants responded that X-rays have an effect on the unborn child.
This is important because it will encourage pregnant women to inform the operator when they are to undergo an X-ray examination so that special protection is dully taken. Over 99% of the respondents thought that they needed to get more informed on dental X-rays examination.
One of the drawbacks of the study was some breakdowns of the X-ray equipment or power outages which meant a longer time to get the required sample size. It also led to some patients getting impatient and leaving the premises without having the X-rays and before getting interviewed. Nevertheless, generally the outcome and relevance of this study was not significantly rarified by these drawbacks.
CONCLUSION
Generally, there was a low awareness of dental X-ray examination in this study which might be attributable to low exposure to information, lack of dental checkup culture in the general population and lack of media outlets that provide information on oral health in general and dental X-ray examination in particular.
RECOMMENDATIONS
There is a need to raise the awareness of patients regarding dental X-ray examination, its importance and associated risks. This can be done by incorporating educational materials with information on dental X-rays in the oral health education that is routinely provided to dental patients.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors are grateful for grant given by the government of Tanzania through the Muhimbili University of Health and Allied Sciences and the Department of Orthodontics, Paedodontics and Community Dentistry. The authors also wish to thank all the participants who voluntarily spared their time to participate in this study.
REFERENCES
|
Abbott P (2000). Are dental radiographs safe? Australian Dental Journal 45(3):208-213. |
|
|
Aravind BS, Joy ET, Kiran MS, Sherubin JE, Sajesh S, Manchil PRD (2016). Attitude and awareness of general dental practitioners toward radiation hazards and safety. Journal of Pharmacy and Bioallied Sciences 8(Suppl 1):S53-S58. |
|
|
Berkhout E, Sanderink G, Van der Stelt P (2003). Digital intra-oral radiography in dentistry. Diagnostic efficacy and dose considerations. Oral Radiology 19(1):1-13. |
|
|
Chiri R, Awan S, Archibald S, Abbott PV (2013). Parental knowledge and attitudes towards dental radiography for children. Australian Dental Journal 58(2):163-169. |
|
|
Hamza O, Matee M I N, Sultan HH (1998). Reasons for taking radiographs in general dental practice in Dar-es-Salaam, Tanzania. International Dental Journal 48(4):374-377. |
|
|
Hwang SY, Choi ES, Kim YS, Gim BE, Ha M, Kim HY (2018). Health effects from exposure to dental diagnostic X-ray. Environmental Health and Toxicology 33(4):e2018017. |
|
|
Kelaranta A, Ekholm M, Toroi P, Kortesniemi M (2015). Radiation exposure to foetus and breasts from dental X-ray examinations: Effect of lead shields. Dentomaxillofacial Radiology 45(1). |
|
|
Matee M, Simon E (2000). Utilisation of dental services in Tanzania before and after the introduction of cost-sharing. International Dental Journal 50(2):69-72. |
|
|
Msagati F, Simon ENM, Owibingire S. (2013). Pattern of occurrence and treatment of impacted teeth at the Muhimbili National Hospital, Dar es Salaam, Tanzania. BMC Oral Health 13(1). |
|
|
Murage D (2001). Knowledge, Attitude and Behaviour of Patients Visiting University of Nairobi Dental Hospital towards Risks of Dental X-rays. Nairobi. |
|
|
Newman B, Seow WK, Kazoullis S, Ford D, Holcombe T (2009). Clinical detection of caries in the primary dentition with and without bitewing radiography. Australian Dental Journal 54(1):23-30. |
|
|
Purmal K, Alam MK, Nambiar P (2013). Patient's perception on dental radiographs. International Medical Journal 20(2):235-238. |
|
|
Shahab S, Kavosi A, Nazarinia H, Mehralizadeh S, Mohammadpour M, Emami M (2012). Compliance of Iranian dentists with safety standards of oral radiology. Dentomaxillofacial Radiology 41(2):159-164. |
|
|
Wenzel A, Møystad A (2010). Work flow with digital intraoral radiography: A systematic review. Acta Odontologica Scandinavica 68(2):106-114. |
|
|
White SC, Atchison KA, Hewlett ER, Flack VF (1994). Efficacy of FDA guidelines for ordering radiographs for caries detection. Oral Surgery, Oral Medicine, Oral Pathology 77(5):531-540. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


