Full Length Research Paper
ABSTRACT
Ever since it was first described by Billroth, there is an increasing incidence of multiple primary malignancies cases, due to increase in the survival rate of cancer patients and improvement of diagnostic tools. Incidence of second malignancies in cancer patients is 10 to 20%. A total of 10 patients who fulfilled the inclusion criteria were included. All the 10 patients’ case sheets were pursued, and the biochemical, radiological and histopathological reports were analyzed. Results revealed that out of the 10 patients, five were synchronous and the other five were metachronous with a median age of 59 years. Four male patients and six female patients are included. The most common malignancy sites were the stomach and breast, and the mean time interval between both the metachronous tumors is 7.2 years. Thus, a strong clinical suspicion is needed for detecting the multiple primary malignancies, anda treatment plan should be formulated individually for every case.
Key words: Neoplasm, multiple primary, synchronous neoplasm, metachronous neoplasm, therapeutics.
INTRODUCTION
The incidence of double primary malignancy is not very rare, Billroth has reported the first case in 1889 (Chakrabarti et al., 2015; Sehgal et al., 2018), while the first statistical analyses was reported by Bugher in 1934 (Sehgal et al., 2018; Sharma et al; 2016). Incidence of double primary malignancies has been underreported due to the difficulties in epidemiological data collection and is allegedly between 2.4 and 17%. Some authors define double primary malignancies as two or more cancers with no subordinate relationship occurring either simultaneously or not in the same patient. With the improvement in medical treatment modalities and imaging techniques (positron emission tomography), there is arise in the incidence of double primary malignancy as the overall survival rate of cancer patients has increased (Chakrabarti et al., 2015; Sehgal et al., 2018). Reported incidence of second cancer in a cancer patient is 10 - 20% (Chakrabarti et al., 2015). The aim of this research is to study the incidence of multiple primary malignancies.
MATERIALS AND METHODS
This is a retrospective observational study done at Saveetha Medical Hospital from January 2016 to December 2018. Hospital records were pursued to retrieve malignancies that qualified as double malignancies as per the International Agency for Research on Cancer Categorization.
We included all patients who had histological proof for double malignancy, fit these into Warren and Gates criteria (Bagri et al., 2014; Sakellakis et al., 2014) (Table 1) and are diagnosed in the period from January 2016 to December 2018. However, the patients who had no clear cut histological diagnosis and those with suspicion of second benign metastasis are excluded. Consent was obtained from the Dean of the Institute and Institutional Ethical Committee for publication of the data.

The cases sheets were analyzed for the biochemical (serological markers), radiological and histopathological (FNAC, Core needle biopsy) reports.
RESULTS
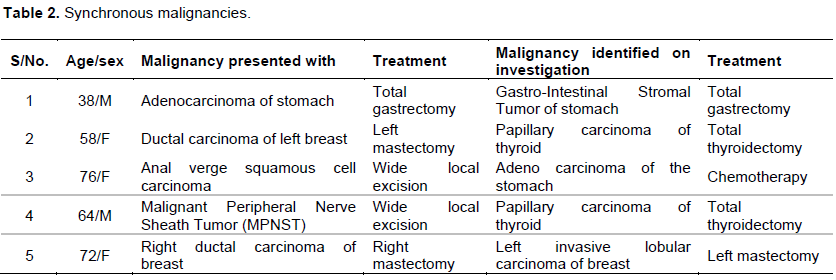
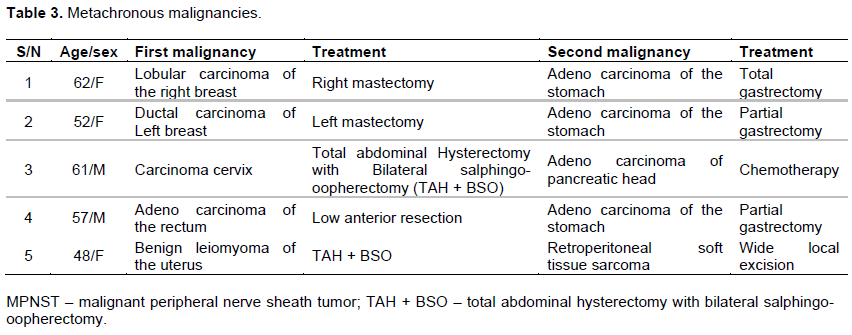
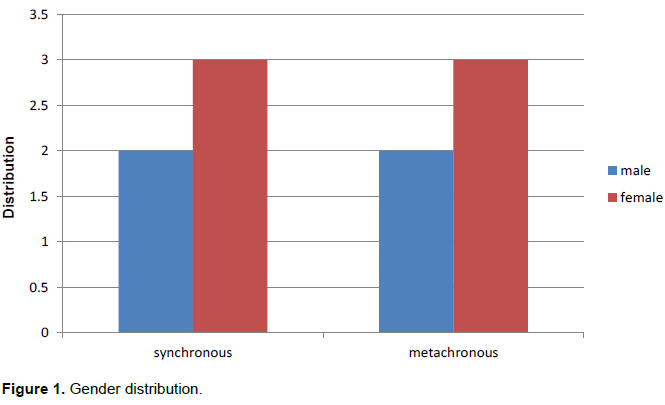
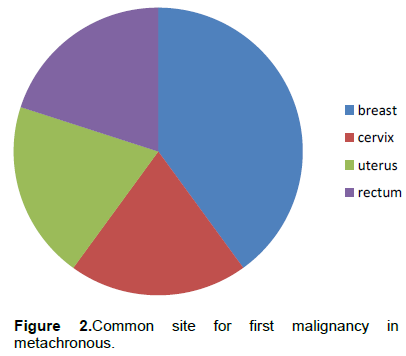
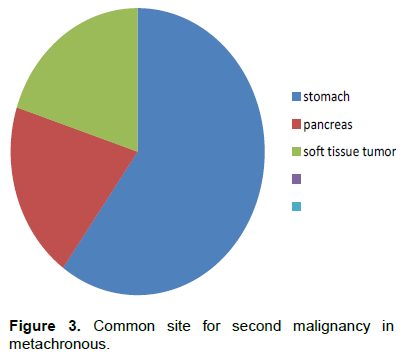
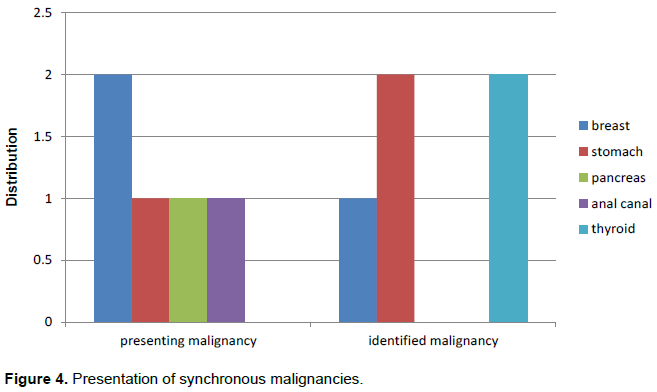
Over a 3-year period (2016 to 2019), we had 10 double primary malignancy cases in our institution. Median age of occurrence was 59 years, with a range of 38 to 76 years. Of the 10 cases, five were synchronous (Table 2) and five were metachronous (Table 3) with a ratio of 1:1 between synchronous and metachronous cases. Male to female ratio noted is 1:1.5 with four males (40%) and six (60%) female’s patients registered in the study (Figure 1). The most common site for primary malignancy in metachronous cases is breast with two cases (40%) and cervix, uterus and rectum each with one case (Figure 2) and the most common site for secondary malignancy in metachronous is stomach with three cases (60%) followed by one case each in pancreas and soft tissue tumor (Figure 3). The most common presenting malignancy in cases of synchronous tumor is breast with two cases (40%) followed by stomach, anal canal and nerve sheath tumor with one case each (Figure 4).The common identified malignancy in cases of synchronous tumors is stomach (40%) and thyroid (40%) with two cases each followed by one case of carcinoma breast (20%). Of the 10 cases, four were early tumors, sixwere advanced tumors, two cases had undergone palliative therapy whereas the other eight cases have undergone surgical treatment. The mean interval between appearances of metachronous tumor is 7.2 years ranging from 2 to 11 years. Majority of the cases are gastrointestinal tumors in this study followed by breast carcinoma.
DISCUSSION
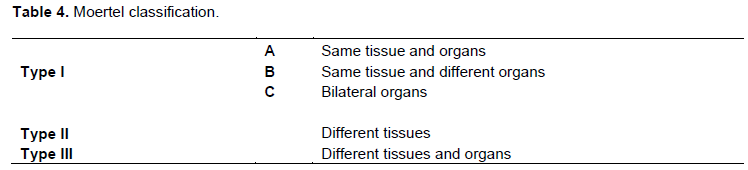
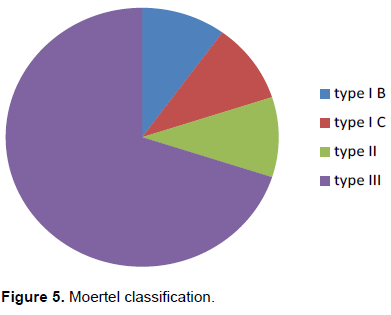
Ever since it was first reported by Billroth (Gupta et al., 2016), there were several studies reported on double primary malignancies. They can be classified by Moertel classification (Jena et al., 2016) or by time interval. By time interval, they are classified as synchronous and metachronous (Ahmed and Abbas 2014; Mesmoudi et al., 2011) tumors but there are no generalized categorization for the time limit.
The surveillance epidemiology and end result (SEER) suggest the interval as 2 months, whereas International Agency for Research on Cancer (IARC) suggest the interval to be 6 months (Sehgal et al., 2018).
In our study, we had one case of type IB (4th case in metachronous table), one case of type IC (5thcase in synchronous table), one type II (1st case in synchronous table), and a maximum of type III (7 cases) (Tables 4 and Figure 5). The pathophysiology in these cases is theorized to be the effect of a common etiological factor on multiple sites known as ‘Field cancerization’ (Joseph et al., 2016; Irmie et al.,2010), which is most commonly seen in head and neck cancers or due to the effect of the treatment to the first malignancy. The most cited etiological factors are genetic susceptibility, immune factors, as well as intensive exposure of carcinogens (Wood et al; 2012). Genetic changes that are noted in double primary malignancy patients are punctiform metastasis, loss of heterozygosity, and microsatellite instability (Bagri et al., 2014). A common genetic change is deleterious mutation. Various syndromes which have been reportedly associated with double malignancies are Hereditary breast and ovarian cancer syndrome (BRCA genes), Lynch syndrome (MMR genes), Von Hippel–Lindau disease (VHC genes), Li- Fraumen syndrome (p53 genes) (Raissouni et al., 2012), and MEN syndrome
(RET genes). Genetic testing can be warranted in patients with multiple primary malignancies but the barrier in Asian countries is the cost effect and misinterpretation of the results (Chan et al., 2018). Doxorubicin based treatment to first cancers show a higher incidence of second malignancy upto 7% (Joseph et al., 2016; Julie, 1995) in metachronous double primary malignancy.
The second malignancy in a metachronous patient is commonly harbored in head and neck cancers (36%) followed by Hodgkin’s lymphoma (26%) (Joseph et al., 2016; Doshi et al., 2017). The currentstudy however showed carcinoma stomach (60%) having a higher incidence followed by pancreas (20%) and soft tissue tumors (20%). Metachronous double primary malignancies are commonly seen in female patients and synchronous tumors have a slight male dominance.This study shows a similarity in metachronous tumors with female dominance (60%) but in synchronous we had female preponderance (60%) and the mean age group in our study is 59 years.
The clinical features that alert the physician to investigating for multiple primary malignancies are atypical metastatic spread, high tumor burden relative to tumor marker load, new metastasis several years after the primary, suspicious lesion in patient who underwent prior chemotherapy or radiotherapy and suspicious lesion on imaging (PET-CT) detected at staging or follow up of a tumor (Vogt et al., 2017; Krishnatreya et al., 2013). Most of the synchronouscases are diagnosed while doing a staging investigation for the first tumor. In this study, one case (case 2 in synchronous table) had presented with complaints pertaining to both tumors. In common, practitioners would label this second primary malignancy as a metastasis and leave it behind. Metachronous tumors are most commonly seen in head and neck region due to field cancerization with a latent interval period of 10-15 years (Bagri et al., 2014; Bolognesi and Bolognesi, 2014).This research showed a low latent interval period of 7.2 years with a range of 2 to 11 years.
This study has majority of casesfrom breast (5) and stomach (5). Incidence of multiple primary malignancies involving breast is 4-8%(Vogt et al., 2017). Patients with breast involvement show mutation of BRCA1 and BRCA2 gene. The common organ involved along with breast is cervix, whereas in patients who have undergone tamoxifen based chemotherapy, haemopoietic cancers are common (Vogt et al., 2017). Incidence of multiple malignancies involving stomach is 2.04 to 3.4%(Kim et al., 2017). A common cause for multiple malignancies involving stomach is field cancerization. Common geneticmutation in cases with stomach involvement includes loss of heterozygosity of APC and MMC genes (Kim et al., 2017).
Prognosis of patients with multiple primary malignancies is poorer when compared to those with a single malignancy(Etiz et al., 2017). Synchronous malignancies in different organs have poor prognosis compared to those in same organ(Joseph et al., 2016). There is no established treatment plan for double primary malignancies. Both tumors are to be thoroughly investigated to rule out the possibility of one being the metastasis of the other and both should be confirmed by histology. Management should be individualized to each case by taking into consideration the stage of disease, performance score of patient, age of patient and survival rate for the tumors individually and other factors. In our study, two cases (1 synchronous, and 1 metachronous) had widespread metastasis and had under palliative therapy.(Di Martino etal., 2002). reported that prognosis of metachronus tumor is better than synchronous tumor.
CONCLUSION
With the increase in survival rate of common cancers and better diagnostic modalities, the incidence of double primary malignancies has increased. A strong clinical suspicion should be there to detect the second malignancy and should be completely evaluated. A treatment plan should be formulated for each case as resectable synchronous tumors can be surgically tackled in a single setting. Long term follow up of the patient is necessary to diagnose any metachronous lesions at an early stage. The limitations of this study were the low sample size and a short study period.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ahmed O, Abbas T (2014). Metachronous double malignancy involving the kidney and the breast: A case report. Case Reports in Clinical Medicine 3:67-69. |
|
|
Bagri PK, Singh D, Singhal MK, Singh G, Mathur G, Jakhar SL, et al. (2014). Double Primary Malignancies: A Clinical and pathological Analysis Report from a Regional Cancer Institute in India. Iranian Journal of Cancer Prevention 7(2): 66-72. |
|
|
Bolognesi M, Bolognesi D (2014). Synchronous Detection of Dual Neoplastic Malignant Disease: Adenocarcinoma of the Caecum and Renal Cell Carcinoma. Journal of Clinical Case Reports.4: 377. |
|
|
Chakrabarti S, Chakrabarti PR, Desai SM, Agarwal D, Mehta DY, Somanath S (2015). Spectrum of second primary malignant neoplasms in central india: case series from a tertiary care centre. Nigerian Postgraduate Medical Journal 22:233-236. |
|
|
Chan GH, Ong PY, Low JJ, Kong HL, Ow SG, Tan DS (2018).Clinical genetic testing outcome with multi-gene panel in Asian patients with multiple primary cancers. Oncotarget. 9(55): 30649-30660. |
|
|
Di Martino E, Sellhaus B, Hausmann R, Minkenberg R, Lohmann M, Esthofen MW (2002). Survival in second primary malignancies of patients with head and neck cancer. Journal of Laryngology and Otology 116:831-838. |
|
|
Doshi PR, karandiakar MN, Swami RC, Singh HA, Nimbargi RC (2017). Dual tumor - clear cell sarcoma of kidney with differentiating neuroblastomaA rare case with review of literature. Indian Journal of Pathology and Microbiology 60: 111-114. |
|
|
Etiz D, Metcalfe E, Akcay M (2017). Multiple primary malignant neoplasms: A 10- year experience at a single institution from Turkey. Journal of Cancer Research and Therapeutics 13:16-20. |
|
|
Gupta D, Singh I, Mahajan N (2016). Second primary malignancies in head and neck region: Report on two cases. MAMC Journal of Medical Sciences 2:152-154. |
|
|
Irmie A, Achimas‑Cadariu P, Burz C, Puscas E (2010). Multiple primary malignancies‑epidemiological analysis at a single tertiary institution. Journal of Gastrointestinal and Liver Diseases 19:69‑73. |
|
|
Jena A, Patnayak R, Lakshmi AY, Manilal B, Reddy MK (2016). Multiple primary cancers: An enigma. South Asian Journal of Cancer 5(1):29-32. |
|
|
Joseph SC, Darlington CD, Anitha GFS (2016).A retrospective and prospective study of double malignancies in a tertiary care hospital in south India - a ten years' experience. International Surgery Journal 3: 674-682. |
|
|
Julie B (1995). Second Malignancies Associated with Doxorubicin, Pediatric Hematology and Oncology 12(2):111-113. |
|
|
Kim DH, Kim SM, Choi MG, Sohn TS, Bae JM, Kim S (2017).Multiple Primary Malignancies in Patients with Multiple Early Gastric Cancer. Journal of Gastric Cancer 17(2):154-161. |
|
|
Krishnatreya M, Rahman T, Kataki AC, Das A, Das AK, Lahkar K (2013). Synchronous primary cancers of the head and neck region and upper aero digestive tract: Defining high‑risk patients. Indian Journal of Cancer 50:322-326. |
|
|
Mesmoudi M, Boutayeb S, Mahfoud T (2011). Triple malignancy in a single patient including a cervical carcinoma, a basal cell carci-noma of the skin and a neuroendocrine carcinoma from an unknown primary site: A case report and review of the literature. Journal of Medical Case Reports 5:462. |
|
|
Raissouni S, Raissouni F, Rais G (2012). Radiation induced esophageal adenocarcinoma in a woman previously treated for breast cancer and renal cell carcinoma. BMC Research Notes 5:26. |
|
|
Sakellakis M, Peroukides S, Iconomou G, Boumpoucheropoulos S, Kalofonos H (2014). Multiple primary malignancies: a report of two cases. Chinese Journal of Cancer Research 26(2): 215-218. |
|
|
Sehgal SA, Gupta P, Dhull AK, Vivek K (2018). Tailored approach for multiple primary neoplasms. Journal of Evidence Based Medicine and Healthcare 5(47):3293-3296. |
|
|
Sharma D, Singh G, Kakkar N, Raj S (2016). Second primary malignancy: A retrospective analysis report from a tertiary cancer center of North India. Indian Journal of Cancer 53:595-599. |
|
|
Vogt A, Schmid S, Heinimann K, Frick H, Herrmann C, Cerny T, Omlin A (2017). Multiple primary tumours: challenges and approaches, a review. ESMO Open 2(2):e000172. |
|
|
Vogt A, Schmid S, Heinimann K, Frick H, Herrmann C, Cerny T, OmlinA(2017).Multiple primary tumours: challenges and approaches, a review. ESMO Open 2:e000172. |
|
|
Wood ME, Vogel V, Ng A, Andrea Ng, Lewis F, Pamela G, Lois BT (2012). Second malignant neoplasms: assessment and strategies for risk reduction. Journal of Clinical Oncology 30(30):3734-3745. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


