Full Length Research Paper

ABSTRACT
Limited studies have examined arousal perception in obstructive sleep apnea (OSA) or other sleep disorders. The aim of this study is to evaluate the factors that affect patients’ arousal and total sleep time perception. This is a retrospective study of 210 subjects divided into 5 groups: Primary insomnia; upper airway resistance syndrome (UARS)/primary snoring; mild, moderate and severe OSA. Perceived arousals were compared to objectively defined arousals. The subjects’ age, body mass index (BMI), total sleep time (TST), perceived TST, sleep efficiency, stage shifts, rapid eye movement (REM) and delta time were compared. UARS/primary snoring group had significantly higher perceived arousal relative to arousal events and shorter total arousal duration than in primary insomnia and all OSA groups. There was a significant linear increase in total arousals and respiratory arousal as OSA severity increased. The number of perceived arousal events was negatively correlated with perception of TST. There was a trend for the insomnia group to have more perceived non-respiratory arousals compared with all OSA groups. Although subjects with UARS/primary snoring had the lowest total arousals, they perceived the highest arousals. The non-respiratory related arousals are probably perceived differently from respiratory arousal related perception. For the insomnia group to have more arousals not driven by respiratory events suggests that insomnia may be better defined as a disorder by being driven to arousals rather than apneas, who are aroused despite being driven towards sleep.
Key words: Arousal perception, arousal misperception, insomnia, primary snoring, upper airway resistance syndrome, sleep
INTRODUCTION
Arousal misperception (as referred to misperception of sleep) is the state of wakefulness with no objective sleep disturbances (Harvey and Tang, 2012). It is defined as a perceived total sleep time (TST) that is less than 80% of objective TST demonstrated in polysomnography (PSG) (Laranjeira et al., 2018). The misperception of TST was defined as abnormal if it was 2 or more standard deviation from the mean for each group studied (Khan et al., 2009). Misperception can also be differentiated by each sleep state such as wake after sleep onset, wake after sleep onset (WASO) or sleep onset latency (SOL) (Hermans et al., 2019).
Self-report sleep quality, which mainly depends on clinical history, may be inconsistent with objective finding on PSG. Poor sleep quality measured by Pittsburgh sleep Quality Index (PSQI) has been reported as the result of sleep state misperception (Slightam et al., 2018). Sleep misperception may be related to hyperarousal which is noted by an increase in high frequency spectral content on the EEG (Maes et al., 2014; Perlis et al., 1997).
Misperception of sleep has been shown to be a common characteristics of insomnia and other psychopathologies (Takano et al., 2016; Harvey, 2012). In insomnia subjects, SOL misperception was related to sleep fragmentation (Hermans et al., 2019).
Misperceived TST defined by the difference between perceive TST and TST from NPSG evaluated by percentage perceived TST related to TST (Pinto et al., 2009). Data from Sleep Disorders Institute showed that in subjects with approximately 20% of rapid eye movement (REM) sleep, 32% with various disorders will not correctly perceive their TST. Furthermore, subjects with the greatest TST misperception had the fewest number of stages shifts on the NPSG (Khan et al., 2009). Compared to subjects with underestimation of sleep, subjects with overestimation of sleep have significant higher daytime sleepiness (Trajanovic et al., 2007). To date, limited studies have examined sleep misperception in patients with sleep disorders (Choi et al., 2016). The objective of this study is to evaluate the factors that affect subjects’ perception of arousals and total sleep time in 5 groups: 1) primary insomnia, 2) upper airway resistance syndrome (UARS)/primary snoring 3) mild obstructive sleep apnea (OSA) 4) moderate OSA and 5) severe OSA.
MATERIALS AND METHODS
Study design and setting
This was a retrospective study from Sleep Disorder Institute, New York. The protocol was approved by the ethics committee and institutional review board of this institution. Subjects’ charts from January 2007 to June 2009 were reviewed. Perceived arousal events and duration, as documented subjectively by the patients after their PSG, were compared to objectively defined sleep arousals duration from NPSG. Perceived TST were also compared to objectively defined TST.
Participants
The inclusion criteria included adults of 18 years or older, normal percentage of REM sleep for age and gender, TST of at least 4.5 h using diagnostic single night nocturnal polysomnogram (NPSG), and insomnia subjects who had apnea-hypopnea index (AHI) <5. Exclusion criteria included patients with the diagnosis of any of the following: REM sleep behavioral disorders, narcolepsy, parasomnias, lung disease, lung surgeries (lobectomy or pneumonectomy), neuromuscular disease, seizure disorders, kyphosis, scoliosis, peripheral vascular diseases, illicit substance abuse (cocaine, heroin or marijuana), and REM altering medications including benzodiazepines and selective serotonin receptor inhibitors, active smoker, ex-smoker who quit within 6 months, subjects with OSA but with symptoms of insomnia and subjects with insomnia with symptoms of OSA. Charts were also excluded for subjects who did not complete all questions on the Questionnaire after their NPSG (incomplete data).
Variables
Patient characteristics including age, gender, body mass index (BMI) were obtained from the electronic charts. Duration of TST, perceived TST, total arousals time including respiratory and non-respiratory related arousal, number of perceived arousal events, number of actual arousal, percentage of sleep efficacy (SE), sleep onset (SO), REM time (REMT), sleep onset REM (SOREM), delta time (N3) and stage shifts were obtained from diagnostic nocturnal PSG (NPSG). Our NPSG montage had measurements of the left and right anterior tibialis muscle electromyography (EMG) lead; two respiratory devices, one on the chest and the other on the abdomen; three chin leads; electrocardiogram and electro-encephalogram electrodes. The international 10-20 system was used. E1, E2, M1, M2, F3, F4, C3, C4, O1, O2 were electrodes were used (Klem et al., 1999). Perceived arousal and perceived TST were subjectively determined just after study completion. These were compared with the objectively obtained arousals and objectively obtained TST from NPSG.
Measurement
The participants were divided into five groups:
(1) Primary insomnia (defined as difficulty initiating or maintaining sleep or nonrestorative sleep according to DSM-IV-TR, 2000),
(2) UARS or primary snoring,
(3) Mild OSA (AHI more than 5 but not more than 15 events/h),
(4) Moderate OSA (AHI more than 15 but not more than 30 events/h) and
(5) Severe OSA (AHI more than 30 events/hour).
American Academy of Sleep Medicine (2005) criteria were used. Scoring of events was done using AASM Manuel for Scoring of Sleep and Associated Events (2007). Two experienced (>15 years of scoring) technologists scored the studies; their reliabilities for identifying arousals were 0.97 and 0.98.
Statistical analysis
The program Statistical Package for Social Sciences (version number 20) was used for data analysis. Continuous data with normal distribution were presented as mean and standard deviation (SD) and median and interquartile range (IQR) for non-normal distribution. Categorical data were number (n) and percentage (%).The continuous PSG variables across all groups were analyzed using one-way Analysis of Variance (ANOVA). Bonferroni corrections were used for multiple comparisons between individual groups. Pearson correlation was used to find the correlation between 5 variables (number of perceived arousal events, perceived arousals relative to NPSG arousals, stage shift, perceived TST, and perceived TST relative to TST from NPSG). P value < 0.05 was considered as statistically significant.
RESULTS
From 2550 participants, the final number of the participants was 210; data are shown in Table 1. Participants were divided into 5 groups based on their sleep disorder type: 1) Primary Insomnia (n = 6), 2) UARS/primary snoring (n 52), 3) Mild OSA (n = 79), 4) Moderate OSA (n = 50), and 5) Severe OSA (n = 23).
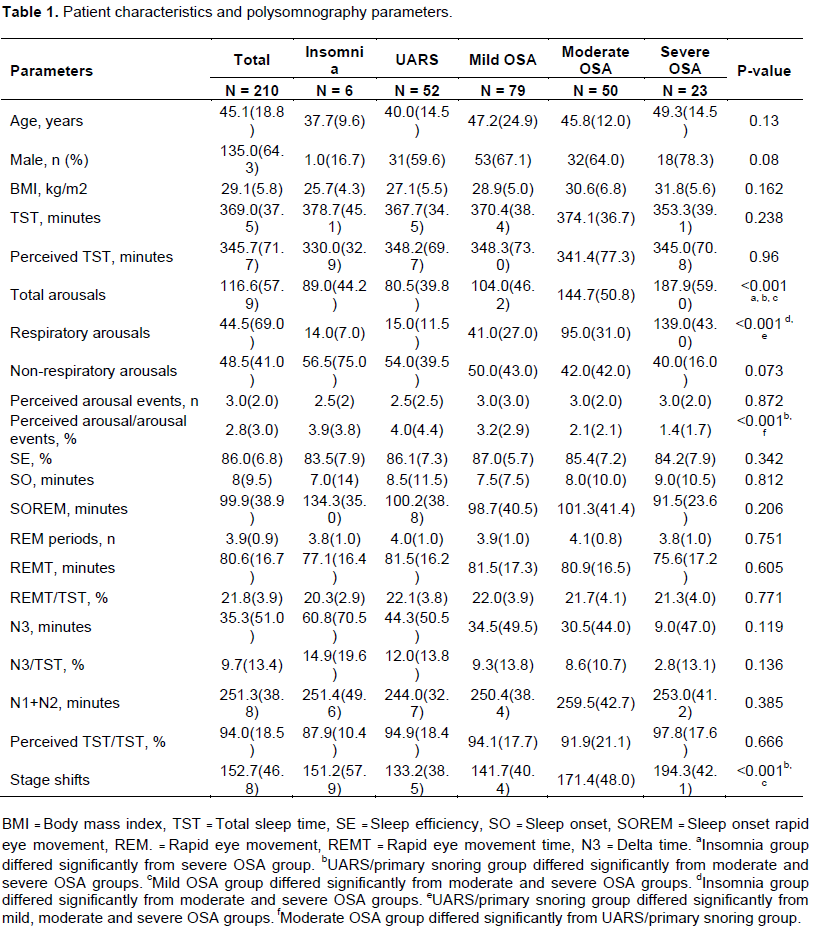
Patients’ characteristics and PSG parameters
When the data were analyzed across all groups, there was no statistically significant difference in age, gender, BMI, TST, perceived TST, perceived arousal events, non-respiratory related arousals, SE, SO, SOREM, REM period (number of REM events), REMT, REMT relative to TST, N3, N3 relative to TST, and perceived TST relative to TST and the sum of N1 and N2 time (Table 1). Significant differences of NPSG data were found in total arousals, respiratory related arousals, perceived arousal relative to NPSG arousal events and stage shifts (p < 0.001). There is a linear increase of total arousals, respiratory related arousals, stage shifts as OSA severity increase with the maximum total duration found in severe OSA. Minimum total arousals and stage shifts were found in UARS/primary snoring and minimal respiratory related arousals were found in primary insomnia. The UARS/primary snoring group had a significantly higher median of perceived arousals relative to NPSG arousal events than in insomnia, followed by mild, moderate, and severe OSA respectively (p < 0.001). There was a trend for insomnia group to have more non-respiratory arousals compared with all the OSA groups and UARS/primary snoring group.
Outcomes
A Bonferroni corrections, using age and NPSG parameters (TST, SE, SO, total arousal, respiratory related arousal, non-respiratory related arousal, perceived arousal events, REM periods, REMT, SOREM, N3, N3 relative to TST, perceived TST relative to TST and perceived arousal relative to NPSG arousal events) were compared between each groups ( primary insomnia, UARS/primary snoring, mild, moderate and severe OSA). Age, TST, SE, SO, non-respiratory related arousal, perceived arousal events, REM periods, REMT, SOREM, N3, N3 relative to TST, perceived TST relative to NPSG TST were not significant when compared to each group (Table 2). UARS/primary snoring group differed significantly from the moderate and severe OSA groups in terms of perceived arousal relative to NPSG arousal events (p = 0.001 and p < 0.001), total arousal ( p < 0.001 and p < 0.001), respiratory arousal (p < 0.001 and p < 0.001) and stage shifts (p < 0.001 and p < 0.001, respectively).
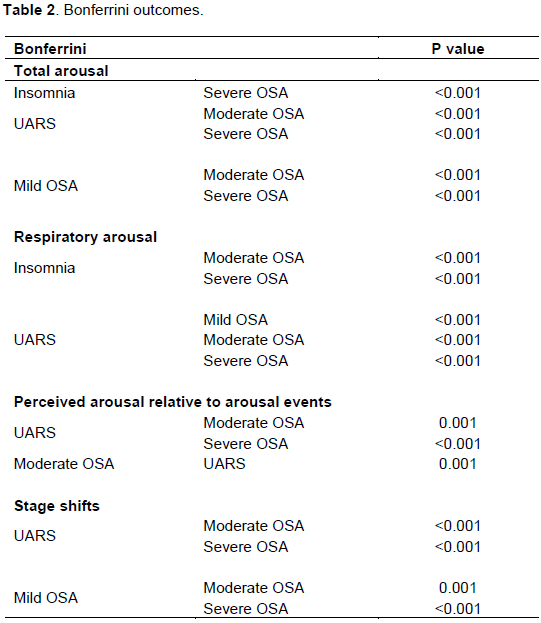
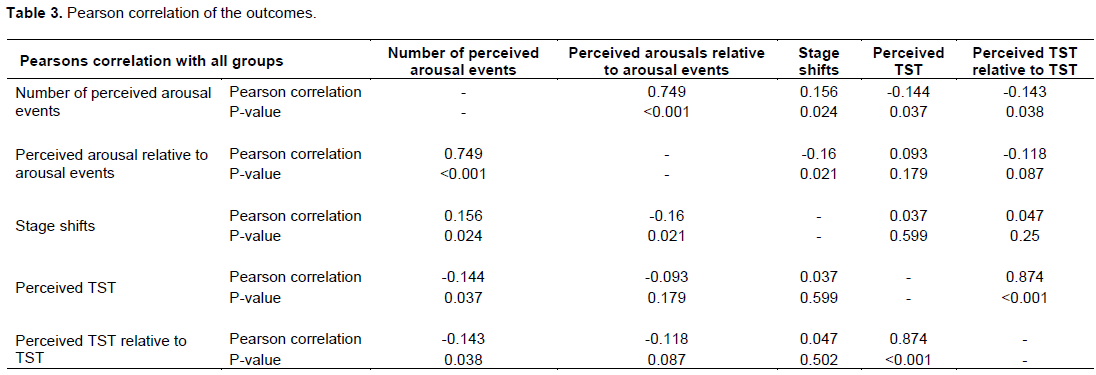
Insomnia differed significantly from severe OSA (p < 0.001) in terms of total arousal. It also differed significantly from moderate and severe OSA in terms of respiratory arousal. For correlation, the number of perceived arousal events showed negative correlation with perception of TST (-0.144, p = 0.037); perceived arousals relative to NPSG arousal events showed a negative correlation with stage shifts (0.749, p < 0.001), and stage shifts (-0.16, p = 0.021) (Table 3). There was no significant correlation between stage shift and perceived TST or perceived TST relative to NPSG TST. Since the insomnia group (group 1) only had six subjects, another analysis was done with the removal of this group. The following results were obtained (Tables 4 to 6).
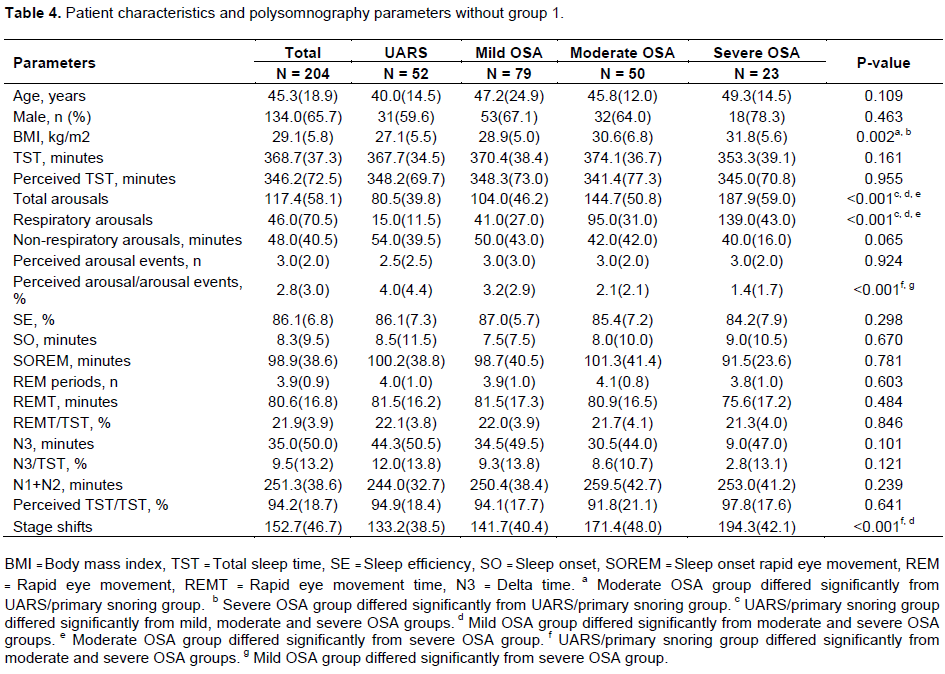
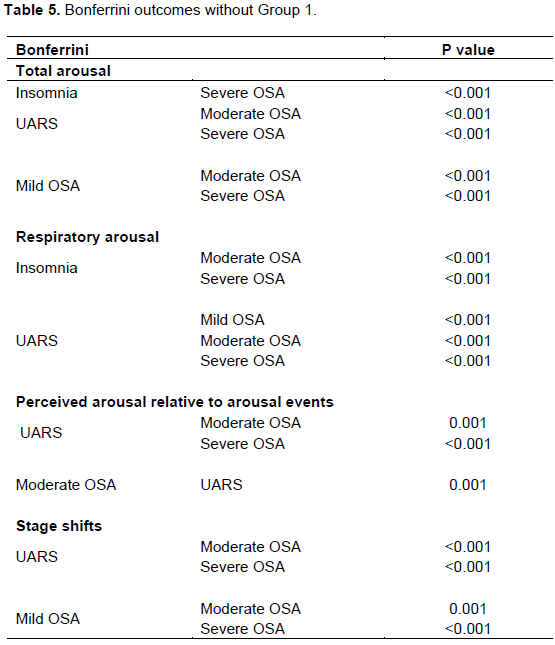
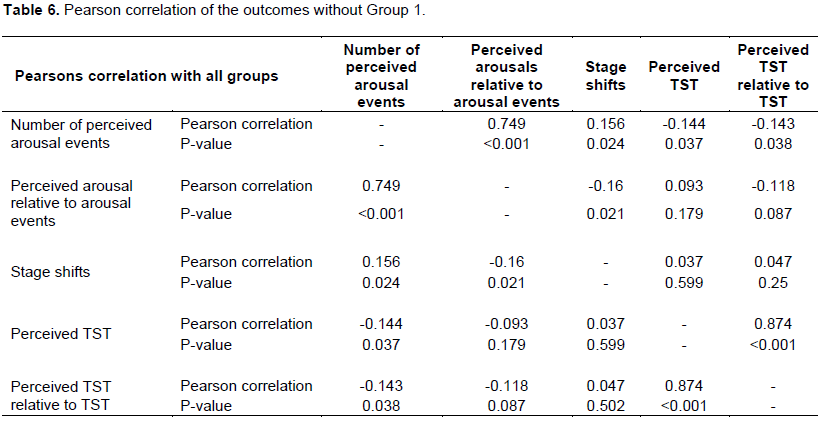
The results were essentially the same as when the insomnia group was included in analysis across all the groups except in BMI. After performing multiple comparison, UARS/primary snoring group still differed significantly from mild, moderate and severe OSA groups in terms of respiratory arousal. UARS/primary snoring group again differed significantly from moderate and severe OSA groups in terms of perceived arousal relative to arousal events. Perceived arousal events also have significant correlation with perceived TST, perceived TST relative to TST. Stage shifts remained significantly correlated with number of perceived arousal events, perceived arousal relative to arousal events but not perceived TST relative to TST.
DISCUSSION
Factors that affect a person’s subjective perception of arousal are important to understand, as they have significant clinical implications in managing patients with sleep disorders. Arousal is an abrupt change in the pattern of brain wave activity which typically represents a shift from deep sleep (REM sleep), to light sleep (NREM sleep), or from sleep to wakefulness. It is crucial to understand that subjective arousal may vary among patients with different sleep disorders. This study tried to compare arousal perception among patients with primary insomnia, UARS, mild, moderate and severe OSA. The study shows four major findings among these groups. The UARS/primary snoring group differed significantly from the moderate and severe OSA groups in perceived arousals relative to arousal events. The UARS/primary snoring group perceived more arousals than the moderate and severe OSA groups. Insomnia differed significantly from severe OSA (p < 0.001) in terms of total arousal. It also differed significantly from moderate and severe OSA in terms of respiratory arousal. But, our sample size was very small.
Broderick et al. (2014) have also noted in their study that patients with UARS have increased somatic arousal compared to healthy controls and that these increased somatic arousals have been directly correlated to increased fatigue, decreased sleep quality and decreased cognitive function affecting physical and mental health adversely. Since somatic arousal is a component of chronic stress, their study supported the hypothesis that UARS represented a syndrome of chronic stress.
Therefore, it would be reasonable to predict that UARS patients could be subjected to more adverse health implications due to this higher perception of arousability as compared to OSA group, which has been demonstrated in our study. However, it has not been established whether increased somatic arousal “causes” the sequelae of poor sleep quality. In order to determine the implications that this can have, more studies are required to clearly establish the pathophysiology of UARS. One thing to note from our study was that we could not demonstrate whether there was a significant difference between TST and perceived TST among insomnia and OSA groups. However, there was one study by Bianchi et al. (2013) that showed that:
(1) The insomnia group underestimated their TST substantially when compared to the OSA group (Bianchi et al., 2013).
(2) The UARS/primary snoring group had fewer respiratory arousals compared to the other apnea
groups but more than the primary insomnia group. One study by Fietze et al. (1999) showed that detecting respiratory arousals helps in understanding the sleep architecture, provides assistance in verifying patients with mild OSA, and aids in managing their treatment (Fietze et al., 1999). Based on our study, we could invite more investigations that support counting respiratory arousals to differentiate UARS from the apneic and insomnia groups.
(3) For the total number of scored arousals, there was a linear increase in total arousals as the severity of OSA increased. The insomnia groups and UARS groups had fewer total arousals.
(4) The differences in total number of arousals were also significant.
Bradley et al. (2014) have shown that respiratory arousal threshold (ArTH) can be used as a clinical predictor for diagnosing OSA, which could eliminate invasive modalities such as the measurement of epiglottic or esophageal pressures using catheters (Edwards et al., 2014).
Similar to the findings of the aforementioned study, our study also suggests that as OSA severity increases, there is increase in respiratory arousal. This could be explained by decrease in arousal threshold. Therefore, it is possible that ArTH can be used as a clinical marker to calculate OSA severity. In our study, stage shifts were correlated with arousal perceptions. From our previous study with TST misperception, this correlation was also noted. N3 in our study was not different significantly among all groups. A study by Ratnavadivel et al. (2009) shown that OSA patients show marked reduction in respiratory and arousal events during slow wave sleep compared to light NREM and REM sleep.
LIMITATIONS AND FUTURE DIRECTIONS
Our study had a few limitations. Night-to-night variability could not be accounted for in a single night study design. Similarly, there may be differing results between studies performed at the patient’s home vs the laboratory. In addition, the subjective reporting of perceived arousals might differ due to recall errors. Our data did not document N1 and N2 times as separate time, but we had TST, REM time, arousal times and N3 time for each subject. We used a formula to find the sum of N1 and N2 times and found no significant difference among all group when analyzed using one-way ANOVA. Our Insomnia group only consisted of 6 patients. Finally, comorbidities such as cardiopulmonary disease, PVD, smoking history and substance abuse usage may alter arousal perception. Our patients report that no illicit substances were used before the NPSGs but drug screens were not done just prior to NPSGs.
CONCLUSION
Although subjects with UARS/primary snoring had fewer total arousals compared to other groups, they perceived their arousals more than subjects with insomnia, mild, moderate or severe OSA. The non-respiratory related arousals are probably perceived differently than respiratory arousal related perception. There was a trend for the insomnia group to have more arousals not driven by respiratory events suggesting that insomnia may be better defined as a disorder of being driven to arousals versus apneics, who are aroused despite being driven towards sleep. In our previous study, TST misperception was correlated with stage shifts like this study arousal perception relative to NPSG arousal events also shows a correlation to stage shifts. This brings to light an unanswered question that needs further research, if a subject with a sleep disorder has more/less stage shifts would he/she have better subjective sleep?
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
AASM Manuel for scoring of sleep and associated events (2007). Rules, terminology and technical specifications, American academy of sleep medicine, Westchester, IL. |
|
|
American Academy of Sleep Medicine (2005). The international classification of sleep disorders, 2nd ed, Diagnostic and Coding manuel, 2nd ed, Hauri PJ (Ed), Westchester, IL. |
|
|
Bianchi MT, Williams KL, McKinney S, Ellenbogen JM (2013). The subjective-objective mismatch in sleep perception among those with insomnia and sleep apnea. Journal of Sleep Research 22(5):557-568. |
|
|
Broderick JE, Gold MS, Amin MM, Gold AR (2014). The association of somatic arousal with the symptoms of upper airway resistance syndrome. Sleep Medicine 15(4):436-443. |
|
|
Choi SJ, Suh S, Ong J, Joo EY (2016). Sleep misperception in chronic insomnia patients with obstructive sleep apnea syndrome: Implications for clinical assessment. Journal of Clinical Sleep Medicine: JCSM: Official publication of the American Academy Sleep Medicine 12(11):1517-1525. |
|
|
Edwards BA, Eckert DJ, McSharry DG, Sands SA, Desai A, Kehlmann G, Bakker JP, Genta PR, Owens RL, White DP, Wellman A, Malhotra A (2014). Clinical predictors of the respiratory arousal threshold in patients with obstructive sleep apnea. American Journal of Respiratory and Critical Care Medicine 190(11):1293-300. |
|
|
Fietze I, Quispe-Bravo S, Schiller W, Röttig J, Penzel T, Baumann G, Witt C (1999). Respiratory arousals in mild obstructive sleep apnea syndrome. Sleep 22(5):583-589. |
|
|
Harvey AG, Tang NK (2012). (Mis)perception of sleep in insomnia: a puzzle and a resolution. Psychological Bulletin 138(1):77-101. |
|
|
Hermans LWA, Leufkens TR, Van Gilst MM, Weysen T, Ross M, Anderer P, Overeem S, Vermeeren A (2019). Sleep EEG characteristics associated with sleep onset misperception. Sleep Medicine 57:70-79. |
|
|
Khan Z, Bachan M, Hyatt S, Ghassibi J, Lund S, Freeman J (2009). Perception of total sleep time (TST) in subjects with various sleep disorders but normal rapid eye movement Sleep (REM). Chest 136(4):67S. |
|
|
Klem GH, Lüders HO, Jasper HH, Elger C (1999). The ten-twenty electrode system of the International Federation. The International Federation of Clinical Neurophysiology. Electroencephalography and Clinical Neurophysiology 52:3-6. |
|
|
Laranjeira CM, Barbosa ERF, Rabahi MF (2018). Is subjective sleep evaluation a good predictor for obstructive sleep apnea? Clinics 73:e355. |
|
|
Maes J, Verbraecken J, Willemen M, Volder I, Van Gastel A, Michiels N, Verbeek I, Vandekerckhove M, Wuyts J, Haex B, Willemen T, Exadaktylos V, Bulckaert A, Cluydts R (2014). Sleep misperception, EEG characteristics and Autonomic Nervous System activity in primary insomnia: A retrospective study on polysomnographic data. International Journal of Psychophysiology 91(3):163-171. |
|
|
Perlis ML, Giles DE, Mendelson WB, Bootzin, RR, Wyatt JK (1997). Psychophysiological insomnia: The behavioural model and a neurocognitive perspective. Journal of Sleep Research 6(3):179-188. |
|
|
Pinto LR, Pinto MCR, Goulart LI, Truksinas E, Rossi MV, Morin CM, Tufik S (2009). Sleep perception in insomniacs, sleep-disordered breathing patients, and healthy volunteers-an important biologic parameter of sleep. Sleep Medicine 10(8):865-868. |
|
|
Ratnavadivel R, Chau N, Stadler D, Yeo A, McEvoy RD, Catcheside PG (2009). Marked reduction in obstructive sleep apnea severity in slow wave sleep. Journal of Clinical Sleep Medicine 5(06):519-524. |
|
|
Slightam C, Petrowski K, Jamison AL, Keller M, Bertram F, Kim S, Roth WT (2018). Assessing sleep quality using selfâ€report and actigraphy in PTSD. Journal of Sleep Research 27(3):e12632. |
|
|
Takano K, Yannick B, Filip R (2016). I sleep with my mind's eye open: Cognitive arousal and overgeneralization underpin the misperception of sleep. Journal of Behavior Therapy and Experimental Psychiatry 52:157-165. |
|
|
Trajanovic NN, Radivojevic V, Kaushansky Y, Shapiro CM (2007). Positive sleep state misperception-A new concept of sleep misperception. Sleep Medicine 8(2):111-118. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


