Full Length Research Paper

ABSTRACT
Because of, well established relationship between seasonal variability and diseases dynamism we embarked here in evaluating recurrently diagnosed diseases dynamism at Korhogo General Hospital in Northern Côte d’Ivoire from 2014 to 2018. For this purpose, clinical data with regard 1707 patients were collected and clusterized in 25 diseases cases. Data have been submitted to multivariate and computational statistical survey with the purpose to assess recurrently diagnosed diseases dynamism from 2014 to 2018. Results supported strong effect of year’s dynamism on recurrent diseases variability by exhibiting high frequency of malaria and hypertension diseases cases. Findings also revealed two diseases clustering groups in terms of diseases variability dynamism. Of note, malaria and high blood pressure diseases exhibited a contrasting attitude in assessing recurrently diagnosed diseases dynamism. Indeed, high blood pressure disease exhibited regular increasing dynamism by contrast to malaria that displayed a relative irregular increasing dynamism. Variance homogeneity tests and descriptive clustering analysis, clusterized recurrently diagnosed diseases at Korhogo General Hospital in two distinct groups, associated to malaria and hypertension, in terms of those diseases increasing dynamism. Diseases discriminated as exhibiting regular increasing dynamism (i.e. diabetes, gastritis, asthma, gastroenteritis and bronchitis) and associated to hypertension, meanly claim to be influenced by patients age parameter as opposed to those showing irregular increasing dynamism; i.e., malaria and influenza (p>0.05). Furthermore, findings revealed cardiac pathologies dynamism as relatively influenced by patients gender and age as opposed to lumbosciatic, back pain, pneumonia and osteoarthritis diseases dynamism that exhibited sole age parameter as a source of data variability (p=0.02-0.07). To conclude our study highlighted a relative yearly increasing diseases variability and revealed two tendencies in assessing recurrently diagnosed diseases dynamism at Korhogo General Hospital from 2014 to 2018.
Key words: Recurrently diagnosed diseases dynamism, Bartlett, Fligner-Killeen and Tukey statistical tests, Korhogo General Hospital.
INTRODUCTION
Several exogenous and endogenous factors can influence geographical disease increase dynamism. Of note, climate change is expected to impact across every domain of society, including health. The majority of the world's population is susceptible to pathological, infectious disease whose life cycles are sensitive to environmental and geographical factors.
Much has been written about climate change and its potential impact on civilizations in the coming decades (Alain, 2000; GIEC, 2001). The authors believe that climate changes are likely to be substantial effects on illness and mortality statistics, disproportionately affecting poorer regions (Patz et al., 2005). Africa's tropical climate is favorable to most major vector-borne diseases because the continent has a high diversity of vector species that have the ability to redistribute into new habitats depending on the climate (Andrew et al., 2000). This redistribution of vectors can lead to a new distribution of diseases as these organisms have varying susceptibility. Thus, seasonality has a major effect on the spatio-temporal dynamism of natural system and their populations’ heath state. Although, tropical area are strongly influenced by parasitic and infectious diseases (Booth, 2018), it is noteworthy to underline the high rate of pathological and as well non-infectious diseases in that area. Indeed, as climate and vector ecology may vary from season to season, each disease may have its own window of seasonal occurrence which may vary from one geographical location to another and differ from other diseases within the same location (Lindsay and Birley, 1996). Thus, establishing a link between an area diseases occurrence and seasons, climate and local comminatory practices, represents a valid tool in the understanding pathologies occurrence dynamism and/or evolution. Despite this link, disease seasonality has not yet been characterized in a systematic and/or rigorous manner for the majority of infections. Here, to contribute to the characterization of the seasonality of some diseases in Northern of Côte d'Ivoire, we evaluate the dynamism and/or the evolution of recurrent diseases diagnosed at the General Hospital of Korhogo from 2014 to 2018.
MATERIALS AND METHODS
Sampling
The authors recorded and collected patients consultation and as well diagnosis information during five (5) consecutive years; 2014, 2015, 2016, 2017 and 2018, at the general medicine subdivision of Korhogo General Hospital. Collected information’s regarded a total of 1707 patients; those were associated to 25 different diseases. Recorded diseases associated to sampling patients at general medicine subdivision of Korhogo General Hospital from 2014 to 2018 are as follow: malaria, AIDS, tuberculosis, varicella, hepatitis, herpes, influenza, gastroenteritis, shingles, hypertension, cardiac pathology, diabetes, lumbosciatic, back pain, osteoarthritis, pneumonia, bronchitis, rhinitis, sinusitis, asthma, gastrointestinal, ulcer, colopathy, gastritis and hemorrhoid. Basing on our previous diseases clustering surveys (Dago et al., 2017), above mentioned diseases have been summarized in (i) infectious and parasitic disease (malaria, AIDS, tuberculosis, varicella, hepatitis, herpes, influenza, gastroenteritis and shingles), (ii) cardiovascular diseases (hypertension and cardiac pathology), (iii) metabolic and endocrine diseases (diabetes), (iv) muscular and osteoarthritis diseases (lumbosciatic, back pain and osteoarthritis), (v) respiratory diseases (pneumonia, bronchitis, rhinitis, sinusitis and asthma) and (iv) digestive diseases (ulcer, colopathy, gastritis and hemorrhoid). Sampling patients (i) gender and (ii) age parameters have been reported and considered for subjacent statistical survey. For this purpose, age parameter has been organized in four (4) random classes’ intervals as follows: 5-14, 15-24, 25-49 and equal or more than 50.
Computational statistical analysis
Computational descriptive and analytical statistic analysis has been performed in R statistical software programming environment. They developed their own script in R version 4.1.0 (2021-05-18) Computing Platform: x86_64-w64-mingw32/x64 (64-bit) for the present statistical survey (R core Team, 2020). Computational statistical survey requested the following R packages installation: (i) pvclust, (ii) multcompView, (iii) factoextra, (iv) devtools to make developing R package easier, (v) ggplot2, (vi) ggfortify, (vii) paran, (viii) MASS, (ix) dplyr, a fast, consistent tool for working with data frame like objects, both in memory and out of memory, (x) ggpubr and/or ggplot2 package is excellent and flexible for elegant data visualization in R and (xi) qgraph. R bar-plot function and/or script have been used for patients’ frequency graph representation.
The authors performed several analytical statistical tests, that is, (i) ANOVA and Tukey multiple comparison statistical tests in comparing recurrently diagnosed diseases variability and Bartlett and Fligner-Killeen variant homogeneity tests in assessing increasing of recurrently diagnosed diseases dynamism.
Description of loaded R packages
Pvclust is a hierarchical clustering with p-values via multi-scale bootstrap re-sampling (Shimodaira, 2004; Suzuki and Shimodaira, 2006). MultcompView is a visualization of paired comparisons package and has been used for multiple data comparison analysis visualization (Piepho, 2004). Factoextra allows extracting and visualizing the results of multivariate data analyses. It provide some easy function to extract and visualize the output of multivariate data analyses, including principal component analysis (PCA), correspondence analysis, multiple correspondence analysis, factor analysis of mixed data, multiple factor analysis and hierarchical multiple factor analysis functions from different R packages. It contains also functions for simplifying some clustering analysis steps and provides ggplot2 package based elegant data visualization (http://www.sthda.com/english/rpkgs/factoextra).
Ggfortify package is for data visualization tools for statistical analysis results (Tang and Horikoshi, 2016; Horikoshi, 2018). Paran package that requests MASS library is an implementation of Horn's technique for numerically and graphically evaluating the components or factors retained in a principal components analysis (PCA) or common factor analysis (FA). Horn's method contrasts eigenvalues produced through a PCA or FA on a number of random data sets of uncorrelated variables with the same number of variables and observations as the experimental or observational data set to produce eigenvalues for components or factors that are adjusted for the sample error-induced inflation (Glorfeld, 1995; Hayton et al., 2004 and Dinno, 2009). Qgraph is the main function of R qgraph package, which automatically creates an appropriate network and sends it to the plotting method (Kraemer et al., 2009).
Description of R software used for analytical tests
Tukey test is a single-step multiple comparison procedure and statistical test. It allows finding means of a factor that are significantly different from each other, comparing all possible pairs of means with a t-test like method. In R, the multcompView allows to run the Tukey test thanks to the TukeyHSD () function. It also offers a chart that shows the mean difference for each pair of group. Assumption for Tukey test application: (i) observation being tested are independent within and among the group; (ii) groups associated with each mean in the test are normally distributed and (iii) there is equal within group variance across the groups associated with each mean in the test (homogeneity of variance) (Tukey, 1949 and William et al., 1981).
In many different types of experiments, with one or more treatments, one of the most widely used statistical methods is analysis of variance or simply ANOVA . In the present study ANOVA test has been applied to assess yearly recorded diseases data variance difference from 2014 to 2018 at Korhogo General Hospital. ANOVA is a form of statistical hypothesis testing heavily used in the analysis of experimental data. A test result (calculated from the null hypothesis and the sample) is called statistically significant if it is deemed unlikely to have occurred by chance, assuming the truth of the null hypothesis. A statistically significant result, when a probability (p-value) is less than a pre-specified threshold (significance level), justifies the rejection of the null hypothesis, but only if the a priori probability of the null hypothesis is not high (Dag et al., 2018).
In this study it performed two statistical analytical tests for variance comparing and/or assesses population and/or data variance homogeneity. The Fligner-Killeen (median) test has been determined in a simulation study as one of the many tests for homogeneity of variances which is most robust against departures from normality, Conover et al. (1981). By contrast to Fligner-Killeen test, Bartlett’s test by comparing variance of more sample (variance multiple comparison analysis) assumes that data are normally distributed. A test is considerate statistically significant for p ≤0.05.
RESULTS
Screening of recorded diseases at the general hospital in Korhogo Northern of Côte d’Ivoire from 2014 to 2018
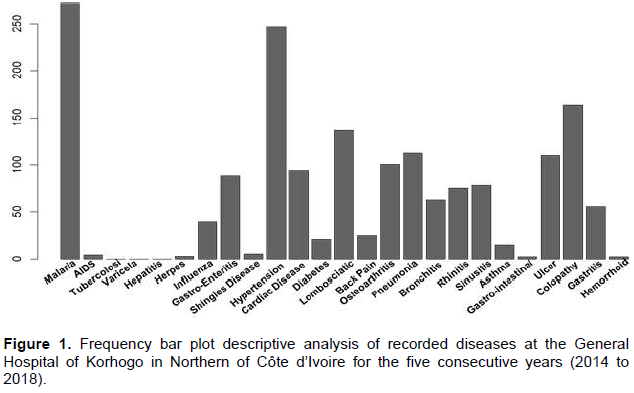
Frequency survey of recorded diseases at the regional general hospital in Korhogo displayed malaria (271 cases) and high blood pressure (247 cases) as the first reasons of patients’ consultation in that hospital (Figure 1). Considering malaria and/or high blood pressure diseases as benchmark, the five consecutive year of the present study supported relative high frequencies of the following diseases: (i) colopathy (p=0.1), (ii) lombosciatica (p=0.1), (iii) pneumonia (p=0.11), (iv) osteoarthritis and (v) ulcer (p=0.16), (vi) gastroenteritis and (vii) cardiac disease (p=0.13). Findings suggested, the modest recurrence of the following diseases: (i) sinusitis, (i) rhinitis, (iii) bronchitis, (iv) influenza, (v) diabetes, (vi) back pain, (v) gastritis and (vi) Asthma from 2014 to 2018 at the general hospital of Korhogo (Figure 1). Study shown weak consultations at the general hospital of Korhogo with regarding the following diseases: (i) AIDS, (ii) herpes, (iii) shingles disease, (iv) gastrointestinal disease and (v) hemorrhoid (Figure 1). Observations revealed no cases of (i) tuberculosis, (ii) hepatitis and varicella during the five consecutive years ranging from 2014 to 2018 (Figure 1).
Variability assessment of yearly recorded diseases at the General Hospital of Korhogo in Northern of Cote d’Ivoire by a p-value clustering analysis
Next, the authors focus on recorded diseases variability survey with the purpose to understand their dynamism during the five consecutive years ranging from 2014 to 2018. In total 187, 227, 258, 422 and 613 patients respectively recorded for years 2014, 2015, 2016, 2017 and 2018 have been included in the present clustering study. In total 1707 patients exhibiting 25 different diseases typologies were processed for above-mentioned statistical survey. P-value clustering analysis had shown high data variability for year 2017 and 2018 by contrast to years 2014 and 2015 (Figure 2A).
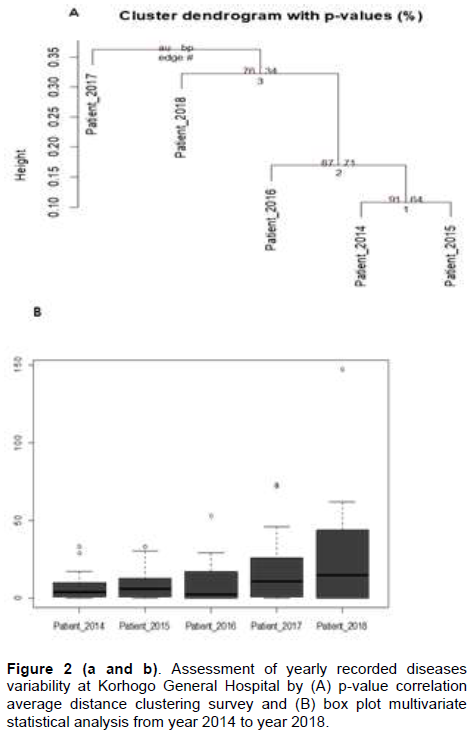
Multivariate box plot descriptive analysis shown a strong patients frequency data variability between year 2014 and year 2018 (Figure 2B). Of note, 613 patients have been received at Korhogo General Hospital in 2018 compared to 187 for the year 2014. In the other words, the number of patients visiting Korhogo General Hospital from 2014 to 2018 increased more than 3 times. Then checking for the effect of year on patient increasing factor, performed ANOVA test suggested statistically significant data variability (p=0.02). In the other words, the number of patients consulted at Korhogo General Hospital significantly increased from year 2014 to 2018. A Turkey test assessing yearly patient consultation mean difference at Korhogo General Hospital showed significant difference between years 2014 and 2018 in contrast to other considered years (supplementary Figure 1).
Whole analysis of the variability of recurrently diagnosis diseases at Korhogo General Hospital from 2014 to 2018
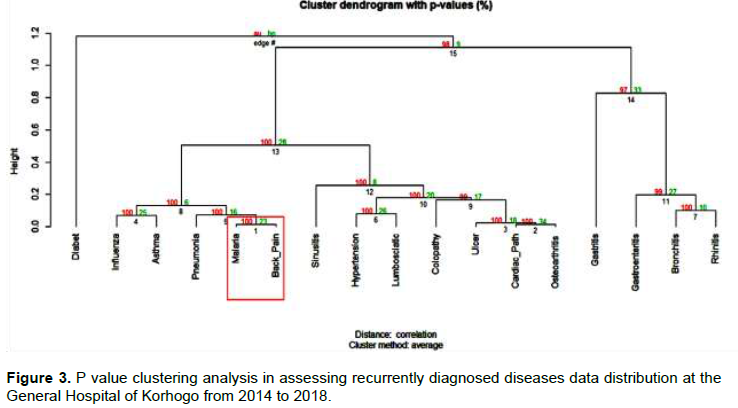
This part of the study processed diseases typologies that included at least 10 patients (patient number to be processed has been randomly chosen). So, 17 diseases have been considered as recurrently diagnosed at the General Regional Hospital of Korhogo from 2014 to 2018. Using eigende composition of correlation matrix by processing Horn's Parallel Analysis for component retention exhibited adjusted eigen values > 1, suggesting 1 component retained as enough in explaining diseases variability in presently analyzed patients’ population. However, even if probability clustering analysis meanly shown AU probability value > 95% recurrent diseases, malaria disease variability are considered to be strongly supported by data (Figure 3). By merging descriptive statistic analysis with principal component analysis (PCA) findings showed that malaria disease as a significant source of data variability (Supplementary Table 1 and Supplementary Figure 1). Principal component clustering analysis stimulation confirmed malaria patients’ population as data variability source and revealed high blood pressure and/or hypertension disease dynamism opposite attitude with respect to malaria disease in terms of potential source of data variability (Supplementary Table 1 and Supplementary Figure 1).
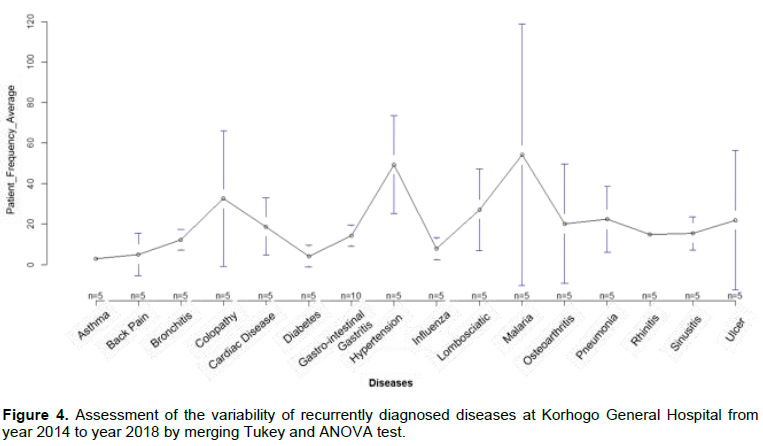
They focused on recurrent diseases dynamism by performing ANOVA test showing statistically significant data variability of the later from year 2014 to year 2018 (df=14, F= 3.21 and p=0.00). Interestingly Tukey to test each pair disease attributed above mentioned diseases data variability to malaria and hypertension patients distribution during the consecutive experimental years (Figure 4, Supplementary Table 2 and Supplementary Figure 2). The same surveys suggested a relative influence of osteoarthritis, colopathy and ulcer diseases on data variability (Figure 4, Supplementary Table 1 and 2).
Multivariate statistical survey in assessing malaria disease dynamism at the General Hospital of Korhogo from year 2014 to year 2018
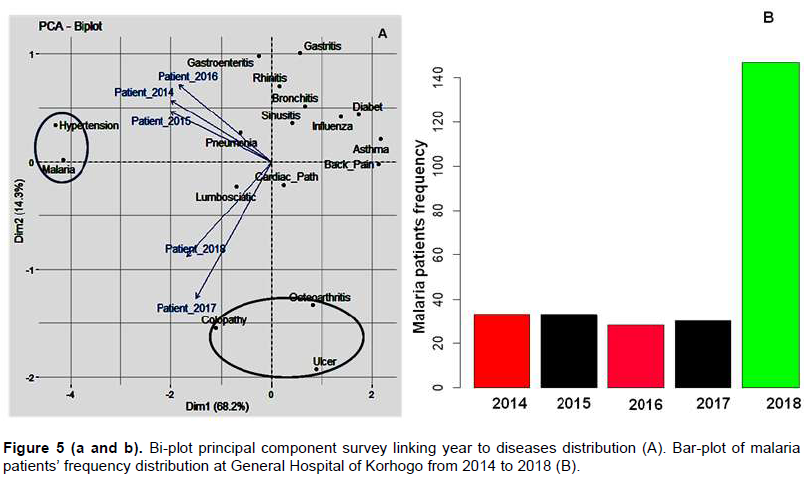
Biplot principal component analysis confirmed malaria and hypertension and/or high blood pressure diseases as good parameters in explaining data variability (Figure 4 and Figure 5A). The same survey reinforced colopathy, osteoarthritis and ulcer diseases as potential interesting parameters in explaining data variability source by clustering years variable in two cluster groups that is (i) years 2014, 2015 and 2016 and (ii) year 2017 and 2018 (Figure 1 and Figure 5A). Because of malaria data variability evidence as previously shown, we embarked here in analyzing inter year dynamism of that pathology. Descriptive statistic showed weak patient frequency variability from year 2014 to 2017; while year 2018 recorded the maximum malaria patients during experimental years (Figure 5B). Based on, year clustering analysis by assessing disease variability at General Hospital of Korhogo (Figure 5B), the authors performed Bartlett variance homogeneity test with the purpose to evaluate malaria patient’s frequency variability from year 2014 to year 2018. Bartlett test result is as following: df=1, K-squared= 7.3 with p= 0.00 suggesting strong data variability with regard malaria patient population between year interval (i) 2014-2016 and (ii) 2017-2018. Because of year 2018 discrepancy in term of patient frequency with respect other analyzed years, we introduced the Fligner Killeen test for homogeneity of variance which is most robust again departure from normality. Results of that test are as follows: Fligner-Killeen: med chi-squared = 3.5139, df = 1 with p = 0.06. Next, we assessed malaria normality distribution by performing Shapiro normality test. From the output, p << 0.05 implied that the distribution of malaria patients during the five consecutive experimental years is significantly different from normal distribution. In the other words, we cannot assume the normality with regard malaria patient’s dispersion.
Multivariate statistical analysis in assessing hypertension, ulcer, osteoarthritis and colopathy diseases dynamism at the General Hospital of Korhogo from year 2014 to year 2018
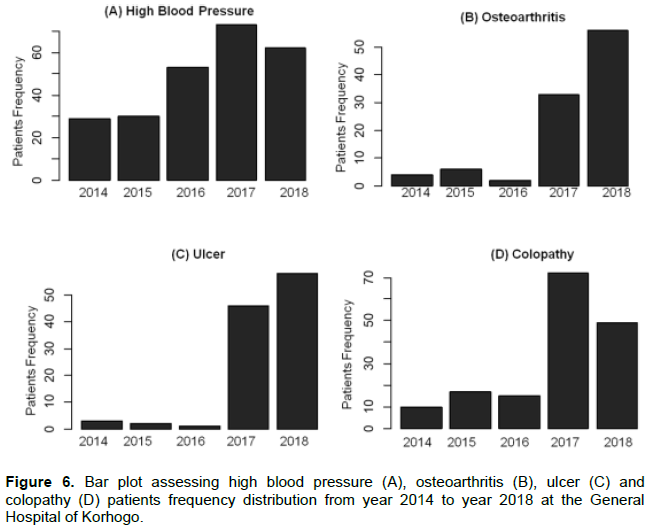
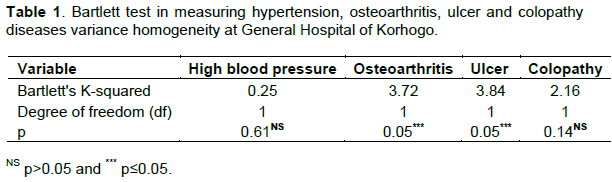
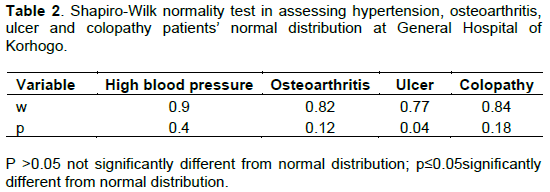
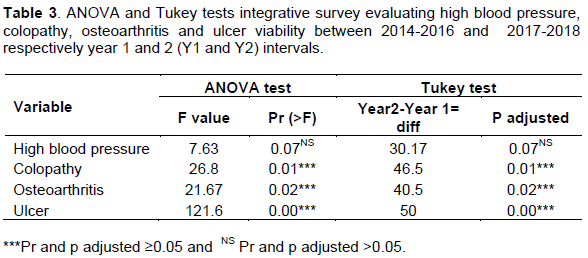
Because of previous results (Figure 5 and Supplementary Figure 2) suggested high blood pressure, ulcer, osteoarthritis and colopathy as influencing patients population dynamism at Korhogo General Hospital, they checked for these diseases variability from year 2014 to year 2018. Descriptive bar-plot statistical survey showed two tendencies with regard these diseases dynamism between year interval classes 2014-2016 and 2017-2018 (Figure 6). Analysis suggested regular increasing of hypertension cases between year interval 2014-2016 and year interval 2017-2018 by contrast to osteoarthritis, ulcer and colopathy diseases (Figure 6). Of note, Bartlett test confirmed hypertension variance homogeneity as previously supported by descriptive statistic and revealed relative regular increasing of colopathy cases by contrast to osteoarthritis and ulcer cases (Table 1). This result is partially in agreement with result reported in Supplementary Figure 2. In addition, Bartlett test attributed weak variance homogeneity (high data variability) to osteoarthritis and ulcer diseases cases (p<0.05) by contrast to high blood pressure and colopathy patients (p>0.05) from year 2014 to 2018 (Table 1 and Supplementary figure 2). Shapiro-Wilk normality test suggested that (i) high blood pressure, (ii) colopathy and (iii) osteoarthritis patient are not significantly different from normal distribution by contrast to ulcer patients’ data (Table 2). Next, the authors performed analysis of variance by integrating ANOVA and Tukey tests with the purpose to highlight homogeneity and/or heterogeneity distribution of the above mentioned diseases cases for 2014-2016 and 2017-2018 year intervals classes (Table 3). These analyses exhibited a significant difference in terms of patients’ frequency for (i) ulcer, (ii) colopathy and (iii) osteoarthritis cases between (i) 2014-206 and (ii) 2017-2018 year interval classes (Table 3). In the other words (i) ulcer, (ii) colopathy and (iii) osteoarthritis diseases cases increased significantly from year 2014 to year 2018 (p<0.05) by contrast to hypertension and/or high blood pressure cases (p>0.05).
Fligner Killeen test for homogeneity of variance analysis of recurrently diagnosed diseases in Northern of Côte d’Ivoire
The authors checked for variance homogeneity of recurrently diagnosed diseases at General Hospital of Korhogo by using Fligner Killeen test, because of highly observed data variability during experimental period, since Fligner Killeen test is very robust again departure from normality. Findings suggested variance homogeneity and/or no significant variance difference with regard recurrent diseases dynamism by considering both 2014-2016 and 2017-2018 year intervals classes (Table 4). Comparative analysis with regard recurrent diseases dynamism from year 2014 to year 2018 by performing Fligner Killeen test suggested a relative high variance homogeneity with regard (i) gastroenteritis,
(ii) lumbosciatic, (iii) diabetes, (iv) high blood pressure, (v) rhinitis, (vi) bronchitis and (vii) asthma diseases cases by contrast to (i) malaria, (ii) influenza, (iii) cardiac pathology, (iv) back pain, (v) osteoarthritis, (vi) pneumonia, (vii) sinusitis, (viii), (ix) ulcer and (x) colopathy diseases cases (Table 4). This result partially confirmed above performed PCA bi-plot analysis by it first component. Considering as a whole, findings supported two tendencies with regard recurrent diseases frequency dynamism at General Hospital of Korhogo from 2014 to 2018.

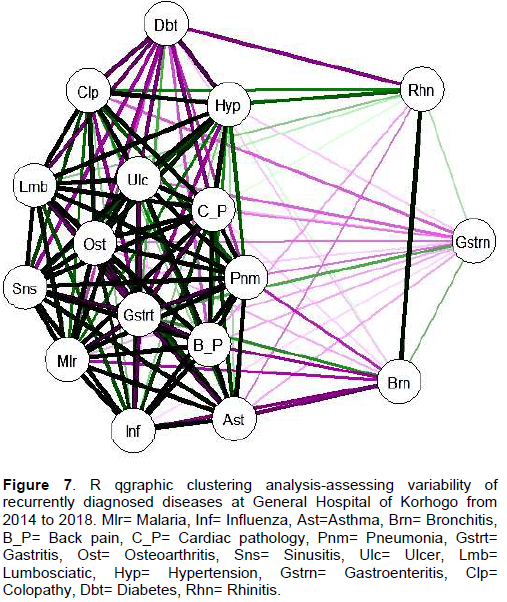
Clustering assessment of recurrently diagnosed diseases variability at General Hospital of Korhogo by R software qgraph package
This part of the study embarked on R software qgraph analysis in assessing variability of recurrently diagnosed diseases at General Hospital. R qgraphic clustering survey by measuring recurrent diseases dynamism and/or variability basing on scroll bar dimension and as well color, exhibited two distinct diseases clustering groups as following: (i) diabetes, rhinitis, hypertension gastroenteritis, gastritis, asthma and bronchitis and (ii) malaria, pneumonia, osteoarthritis, sinusitis, influenza, cardiac pathology, and back pain (Figure 7). Moreover, R qgraphic analysis suggested high dynamism contrast between (i) gastroenteritis, diabetes, rhinitis and bronchitis diseases cases and (ii) malaria, sinusitis, Lumbosciatic and influenza diseases cases. Of note, R qgraphic survey basing on scroll bar dimension revealed strong interaction between (i) diabetes and hypertension recorded cases as well as between (i) bronchitis and asthma in terms of measuring diseases dynamism. The same survey by assessing recurrent diseases dynamism from year 2014 to 2018 exhibited a strong interaction between lumbosciatic, osteoarthritis and back pain diseases (Figure 7). Taking together, present analysis supported evidence of two clustering diseases groups in evaluating recurrent disease dynamism in Northern of Cote d’Ivoire from year 2014 to 2018.
Interaction analysis between recurrent diagnosed diseases and patients morph-metric features (age) and gender parameters: case of malaria and hypertension diseases
Herein data have been organized base on patient age and gender features as follows: Female and male were associated to 5-15, 16-25, 26-50 and >50 age interval classes. Fligner test assessing variance homogeneity with regard diseases distribution at General Hospital of Korhogo by considering patient gender and age parameters supported significant data variability (p<0.05). In the others words, recurrently diagnosed diseases variability at Korhogo General Hospital could be explained by patients’ gender and/or age parameters. Because of contrasting behaviors between malaria and hypertension diseases in explaining data variability, we checked for the influence of patients’ gender and age in characterizing these diseases dynamism at the General Hospital of Korhogo. Interactions surveys by Bartlett variance homogeneity test, between malaria and/or hypertension diseases variability and patients anthropomorphic features exhibited a significant impact of age parameter on high blood pressure (hypertension) disease dynamism (p<0.05) by contrast to gender parameter from year 2014 to 2018 (Table 5). Merging Bartlett and Flinger tests results, findings revealed high blood pressure disease (p= 0.18-0.28) as relatively impacted by gender feature by contrast to malaria pathology (p=0.76-0.84). Considering as a whole, high blood pressure disorder dynamism at Korhogo General Hospital results to be significantly and relatively influenced by patients age and gender features respectively by contrast to malaria disease dynamism.

Comparative analysis of recurrently diagnosed diseases variance homogeneity at Korhogo General Hospital by patients’ age and gender parameters
The authors embarked in a comparative survey between (i) sinusitis, lumbosciatic, influenza, cardiac pathology, back pain, pneumonia and osteoarthritis diseases associated to malaria and (ii) diabetes, gastritis, asthma, gastroenteritis and bronchitis pathology linked to hypertension disease in terms of recurrent diseases dynamism parameter from 2014 to 2018 as supported by previous clustering analysis. They previously showed a regular dynamism of hypertension disease from 2014 to 2018 at Korhogo General Hospital by contrast to malaria. They also showed a strong relationship between high blood pressure disease dynamism and patient age as opposite to malaria pathology. The present analysis by Fligner Killeen test suggested recurrent diseases characterized by regular dynamism (Table 4); that is, lumbosciatic, diabetes, gastritis, asthma, gastroenteritis and bronchitis, as influenced by patient age parameter (p=0.07) and among them, lumbosciatic disease dynamism is significantly influenced by patient gender. Diseases associated with a relative heterogeneous dynamism; i.e. sinusitis, cardiac pathology, back pain pneumonia and osteoarthritis claim to be influenced by patient age only. Influenza disease dynamism does not exhibit any relationship with patient age and gender parameters as opposite to cardiac pathology. Considering as a whole, this findings suggested recurrently diagnosed diseases dynamism at General Hospital of Korhogo as potentially influenced by (i) age, (ii) gender and (iii) both age and gender parameters.
DISCUSSION
Diseases recrudescence dynamism can be explained by multitude exogenous and endogenous factors. It is well established that disease phenomena increases steadily with age parameter. Indeed, study assessing pathological and non-infectious disease that is, high blood pressure troubles contributing in cardio-vascular disease occurrence exhibited age parameter as a valid factor in explaining cardio-vascular pathologies ascension in a hypertensive patient population sampled at Korhogo General Hospital in Northern Cote d’Ivoire (Noel et al., 2017 and Dag et al., 2018). Previous studies performed in that locality (Northern Cote d’Ivoire) suggested female susceptibility with regard to infectious and parasitic diseases (Dago et al., 2017). Considering as a whole, integration between exogenous and endogenous factors associated to seasonal impact on diseases ascension can strongly help in highlighting and as well in understanding recrudescence dynamism sources of recurrent diseases in that area. Herein, the authors were interested in evaluating the dynamism of the increase in the frequency of recurrently diseases diagnosed at the general hospital of Korhogo during five (5) consecutive years from 2014 to 2018. Findings clearly suggested two tendencies evaluating recurrently diagnosed pathologies dynamism at Korhogo General Hospital from 2014 to 2018, when data were organized in year class interval. These two tendencies are characterized by malaria and high blood pressure troubles that respectively exhibited irregular and regular dynamism in terms of the increase in the frequency of recurrently diagnosed diseases at Korhogo General Hospital. In the other words parasitic and infectious disease (malaria) and pathological and non-infectious disease (high blood pressure) display a contrast dynamism tendency in terms of frequency increase regarding recurrently diagnosed disease in Northern of Cote d’Ivoire. Statistical clustering analysis and as well analytical statistical survey had shown a strong relationship between high blood pressure disease dynamism and/or occurrence and patient age as opposed to malaria. An age-related increase in blood pressure is viewed as a universal feature of human aging (Finch, 2007; O'Rourke and Nichols, 2005 and Baksi et al., 2009). Study suggests that people over age 40 years, systolic blood pressure increases by around 7 mmHg per decade (Wolf-Maier et al., 2003 and Stegmary et al. 2003). Epidemiological surveys show a progressive increase in systolic blood pressure with age, reaching an average of around 140 mmHg by the eighth decade (Whelton, 1994). Diastolic blood pressure also increases with age but at a lower rate than systolic blood pressure; diastolic blood pressure may even fall at late ages (Franklin et al., 1997). Their findings supported a relative significant impact with regard to patient gender, vis-à-vis of regular dynamism occurrence of hypertension. Coylewright et al., (2008), states that women show lower systolic and diastolic blood pressure than men up until the age of menopause, when women's systolic blood pressure surpasses that of men. In the same tendency our previous study in Korhogo locality suggested high susceptibility of women in exhibiting high blood pressure disturbs over age 40 years (Dago et al., 2018). Considering as a whole, the progressive increase of age and as well patient gender relatively modulates hypertensive state and/or occurrence. By contrast to hypertension disturbs and/or pathological and non-infectious disease, parasitical disease occurrence and ascension do not and/or relatively depend on patients age and gender parameters. Of note, parasitic diseases can be transmitted by animal (zoonotic), food, blood, water and insect (that is, malaria). Malaria transmission depends on climatic conditions that may affect the number and survival of mosquitoes, such as rainfall patterns, temperature and humidity. In many places, transmission is seasonal, with the peak during and just after the rainy season. Malaria epidemics can occur when climate and other conditions suddenly favor transmission in areas where people have little or no immunity to malaria. They can also occur when people with low immunity move into areas with intense malaria transmission. Some population groups are at considerably higher risk of contracting malaria, and developing severe disease, than others. These include infants, children under 5 years of age, pregnant women (Anna et al., 2015 and Brooker et al., 2009) and patients with HIV/AIDS, as well as non-immune migrants, mobile populations and travellers. So, contrasting dynamism of the increase in the frequency of hypertensive (noninfectious pathology) and malaria (infectious disease) patients from 2014 to 2018 at Korhogo General Hospital can be explained by the divergence and/or heterogeneity of factors and/or sources favoring their occurrence. Interestingly disease associated to hypertension in terms of regular dynamism regarding recurrently diagnosed diseases frequency increase at Korhogo General Hospital in Northern of Cote d’Ivoire from 2014 to 2018; that is diabetes, lumbosciatic, gastritis, asthma, gastroenteritis and bronchitis claim to be influenced by patients’ age parameter. Positive correlation evidence between diabetes ascension and age rising is currently discussed in medical field. Indeed, recent observation in that sense suggested as following: in the age group of 20-44 years, it was estimated about 3.7% people had diabetes; while in the age group 45-64 years the number increased to 13.7%; and the highest percentage of 26.9% was found in the age group of ≥ 65 years (Ketut et al., 2012). These observations clearly exhibit diabetes occurrence increase with rising age. The prevalence of glucose intolerance increases with advancing age. The main factors of that metabolic disorder are that aging induces decrease insulin sensitivity and alteration or insufficient compensation of beta cell functional in the face of increasing insulin resistance (Chang and Halter, 2003 and Ketut et al., 2012). Also, several findings prove that lumbar disc herniation level increase with age. Indeed, these studies supported that with increasing age, lumbar disc herniation is more cranially localized (Dammers and Koehler, 2002). It is noteworthy to underline that evidence between gastritis, asthma, gastroenteritis and bronchitis pathologies occurrence and age increasing is not clearly established, even if older age can represent a risk factor for gastritis ascension in the population (Green. and Graham, 1990). Asthma, a chronic inflammatory airway disease, is usually considered a disease of childhood onset. However, a large number of adults are reporting the onset of asthma past childhood (Thomsen et al., 2005). Although asthma is usually considered to originate in childhood, adult-onset disease is being increasingly reported. Sood et al. (2013) challenges the dictum that most asthma in adults originates in childhood. The second group of recurrently diagnosed diseases at Korhogo General Hospital from 2014 to 2018, characterized by irregular dynamism in terms of the increase in the frequency of those diseases, includes malaria, influenza, cardiac pathology, back pain, osteoarthritis, pneumonia, sinusitis, ulcer and colopathy diseases. The findings of the authors suggest that irregular dynamism with regard these pathologies as not depending necessary on patient age and/or gender parameters as opposed to the first group. Although malaria recrudescence and/or recurrent infection among children is well established, studies that assessed the relationship between malaria ascension and patient age increasing showed conflicting issues (Mawili-Mboumba et al., 2013). Further, according to the level of malaria transmission and immunity acquisition, vulnerable populations differ in endemic areas. In highly endemic settings, children under five years and pregnant women are the most affected, constituting the main target population of new malaria control strategies as recommended by the World Health Organization (WHO, 2010). Several studies exhibit influenza as a risk of death for older patients (Christopher et al., 2019). In the other words, there is no correlational evidence, between influenza occurrence and patient age increasing. The consequences of influenza virus infection are generally more severe in individuals over 65 years of age that is, the elderly (Hernandez-Vargas et al., 2014). Influenza is an acute viral disease that can cause varying mortality in different age groups. The morbidity, mortality and epidemic level of influenza usually vary by season, in part due to changes in the predominant circulating virus types and subtypes (Gavigan and McCullers, 2019). Ji-Rong et al. (2020) confirmed influenza cases from both community and severe complication surveillance studies revealed that age distributions varied by mild and/or severe cases, virus types and/or subtypes and seasons. Considering as a whole, observed irregular dynamism in the increase frequency of both malaria and influenza diseases at Korhogo General Hospital from 2014 to 2018 can be explained by the extreme and multiple heterogenic endogenous as well as exogenous factors that influence those diseases recrudescence. The authors’ findings revealed that colopathy disturbs among diseases with high recurrence frequency characterized by irregular dynamism. Due to its considerable reserve capacity, the gastrointestinal system is better insulated from the effects of aging than other organ systems in the body. Changes to the gastrointestinal system generally consist of a decrease or slowing of functions and an increased risk of digestive tract disorders. The gastrointestinal system extends from the mouth to the anus and includes the throat, esophagus, stomach, and intestines. It is responsible for breaking down food into nutrients, absorbing the nutrients into the bloodstream, and eliminating waste from the body. It remains relatively stable until approximately age 65 (Rémond et al., 2015). Malnutrition is one of the most relevant conditions that negatively influence the health of older people and the nutritional status of elderly was even recently shown to predict preterm death (Soderstrom et al., 2014). Although aging is not inevitably accompanied by malnutrition, many changes due to the aging process can promote this serious condition (Landi et al., 1999), suggesting gastrointestinal disease recrudescence as significantly influenced by heterogenic exogenous parameters.
As previously suggested, this evidence can be a source of observed irregular dynamism in the increase frequency of colopathy recrudescence. It is believe that, extending study year period could be useful in highlighting recurrently diagnosed diseases dynamism and the causes of that dynamism.
CONCLUSION
To conclude, the present study supported two disease categories, in terms of the dynamism of the increase of patients frequency associated to recurrently diagnosed diseases at Korhogo General Hospital from 2014 to 2018. These two diseases categories exhibited regular and irregular frequency increasing dynamism, and can be respectively grouped in (i) non-infectious pathologies and (ii) parasitical and infectious pathologies. So, while, pathological and non-infectious diseases exhibiting regular increase represented by high blood pressure troubles assert to depend on patients anthropomorphic features that is, age and gender, parasitical and infectious diseases linked to irregular increase dynamism that is, malaria, which claim to be non-strongly influenced by those parameters.
ACKNOWLEDGMENTS
The authors would like to thanks the central administration of Korhogo General Hospital for their kind collaboration in providing the clinical data for the present study.
CONFLICT OF INTERESTS
The authors have not declared any conflicts of interests.
REFERENCES
|
Alain B (2000). Les changements climatiques et leurs impacts. Vertigo la revue électronique en sciences de l'environnement, Changements climatiques. 1(2) Numéro Spécial. |
|
|
Andrew KG, Steve WL, Ulisses EC, Jonathan AP (2000). Changement climatique et maladies à transmission vectorielle: une analyse régionale. Bulletin of the World Health Organization 78(9):1136-1147. |
|
|
Anna ME, Jenny H, Abdisalan MN, Robert WS, Feiko OK (2015). Prevalence of malaria infection in pregnant women compared with children for tracking malaria transmission in sub-Saharan Africa: a systematic review and meta-analysis, The Lancet Global Health 3(10):e617-e628. |
|
|
Baksi AJ, Treibel TA, Davies JE, Hadjiloizou N, Foale RA Parker KH, Francis DP, Mayet J, Hughes AD (2009). A meta-analysis of the mechanism of blood pressure change with aging. Journal of the American College of Cardiology 54(22):2087-2092 |
|
|
Booth M (2018). Climate Change and the Neglected Tropical Diseases. Advances in parasitology 100:39-126. |
|
|
Brooker S, Kolaczinski JH, Gitonga CW, Noor AM, Snow RW (2009). The use of schools for malaria surveillance and programme evaluation in Africa. Malaria Journal 8(1):1-9. |
|
|
Chang AM, Halter JB (2003). Aging and insulin secretion. American Journal of Physiology and Endocrinology Metabolism 284(1):E7-12. |
|
|
Christopher AC, Lisa M, Nisha A, Heidi LW, Charisse NC, Melissa AR, Evan JA, Nancy MB, Laurie MB, Shua JC, Seth E, Robert M, Melissa McM, Maya LM, Alison M, Ilene R, William S, Ann RT, Kimberly YH, Shikha G, Rachel KH (2019). Age Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes among Older Adults Hospitalized With Influenza U.S. Influenza Hospitalization Surveillance Network (FluSurv-NET), Open Forum Infectious Diseases 6 (7). |
|
|
Coylewright M, Reckelhoff JF, Ouyang P (2008). Menopause and hypertension: an age-old debate. Hypertension 51(4):952-959. |
|
|
Dago DN, Diarrassouba N, Touré A, Lallié HD, N'Goran, KE, Ouattara H, Kouadio J, Coulibaly A (2017). Whole Screening Analysis Discerning Recurrently Diagnosed Diseases in a Northern Locality of Côte d'Ivoire. International Journal of Development Research 7(11):16598-16604. |
|
|
Dag O, Dolgun A, Konar NM (2018). One way test: An Package for one-way testing in independent group designs. The R Journal 10(1):175-199. |
|
|
Dago DN, Lallié HD, Moroh AJL, Niamien CJM, Ouattara H, Dagnogo O, Téhoua L, Touré A, Kouadio KJ, Kimou AF, Djaman AJ (2018). Relationship between Age and Weight Features in Discriminating Hypertensive Patient Population Gender, American Journal of Medicine and Medical Sciences 8(2):360-367. |
|
|
Dammers R, Koehler PJ (2002). Lumbar disc herniation: level increases with age. Surgical Neurology 58(3-4):209-212; discussion 212-3. |
|
|
Dinno A (2009). Exploring the Sensitivity of Horn's Parallel Analysis to the Distributional Form of Simulated Data. Multivariate Behavioral Research 44(3): 362-388. |
|
|
Franklin SS, Gustin W, Wong ND, Larson MG, Weber MA, Kannel WB, Levy D (1997). Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart StudyCirculation 96:308. |
|
|
Finch C (2007). The Biology of Human Longevity. San Diego, CA: Academic Press. |
|
|
Gavigan P, McCullers JA (2019). Influenza: annual seasonal severity. Current Opinions in Pediatric 31(1):112-118. |
|
|
Groupe d'Experts Intergouvernemental sur l'Evolution du Climat (GIEC) (2001). Climate Change2001: Third Assessment Report (Volume I). Cambridge, Cambridge University Press. |
|
|
Glorfeld LW (1995). An Improvement on Horn's Parallel Analysis Methodology for Selecting the Correct Number of Factors to Retain. Educational and Psychological Measurement 55(3):377-393. |
|
|
Green LK, Graham DY (1990). Gastritis in the elderly. Gastroenterology Clinics of North America 19(2):273-292. |
|
|
Hayton JC, Allen DG, Scarpello V (2004). Factor Retention Decisions in Exploratory Factor Analysis: A Tutorial on Parallel Analysis Organizational Research Methods 7(2):191-205. |
|
|
Horikoshi M, Tang Y (2018). Ggfortify: Data Visualization Tools for Statistical Analysis Results. |
|
|
Hernandez-Vargas EA, Wilk E, Canini L, Toapanta FR, Binder SC, Uvarovskii A, Ross TM, Guzmán CA, Perelson AS, Meyer-Hermann M (2014). Effects of aging on influenza virus infection dynamics. Journal of Virology 88(8):4123-4131. |
|
|
Ji-Rong Y, Chuan YH, Hsiang-Yi H, Shu-Zhen H, Fu-Ting W, Fang-Tzy W, Chung-Hao L, Ming-Tsan L (2020). Seasonal dynamics of influenza viruses and age distribution of infected individuals across nine seasons covering 2009-2018 in Taiwan, Journal of the Formosan Medical Association 119(4):850-860. |
|
|
Ketut S, Pande D, Made SS, Tuty KRA (2012). Age is an Important Risk Factor for Type 2 Diabetes Mellitus and Cardiovascular Diseases, Glucose Tolerance, Sureka Chackrewarthy, Intech Open, |
|
|
Kraemer N, Schaefer J, Boulesteix AL (2009). Regularized Estimation of Large-Scale Gene Regulatory Networks using Gaussian Graphical Models BMC Bioinformatics 10:384. |
|
|
Landi F, Zuccala G, Gambassi G, Incalzi RA, Manigrasso L, Pagano F, Carbonin P, Bernabei R (1999). Body mass index and mortality among older people living in the community. Journal of the American Geriatrics Society 47(9):1072-1076. |
|
|
Lindsay SW, Birley MH (1996). Climate change and malaria transmission. Annals of Tropical Medicine and Parasitology 90: 573-588. |
|
|
Mawili-Mboumba DP, Akotet MKB, Kendjo E, Nzamba J, Medang OM, Mbina MJR, Kombila M, MCORU team (2013). Increase in malaria prevalence and age of at risk population in different areas of Gabon. Malaria Journal 12(1):1-7. |
|
|
Noel DD, Nafan D, Hermann DL, Souleymane S, Tuo Y, Inza JF, Edouard KN, Florent AK Adama C (2017). Performance Assessment of the Recurrence of Cardiovascular Pathologies Symptoms in a Hypertensive Population. Journal of Health Science 7(1):9-19. |
|
|
O'Rourke MF, Nichols WW (2005). Aortic diameter, aortic stiffness and wave reflection increase with age and isolated systolic hypertension. Hypertension 45:652-658. |
|
|
Patz JA, Campbell-Lendrum D, Holloway T, Foley JA (2005). Impact of regional climate change on human health. Nature 438(7066):310-317. |
|
|
Piepho HP (2004). An Algorithm for a Letter-Based Representation of All-Pairwise Comparisons, Journal of Computational and Graphical Statistics 13(2):456-466. |
|
|
R core Team (2020). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienne, Austria. |
|
|
Rémond D, Danit RS, Doreen G, Paula P, Josefa K, Marie-Agnès P, Claudia NDS, Barbara W, Alessandra B, Didier D, Lidia TC, Guy V (2015). Understanding the gastrointestinal tract of the elderly to develop dietary solutions that prevent malnutrition. Oncotarget 6(16):13858. |
|
|
Shimodaira H (2004). Approximately unbiased tests of regions using multistep multi-scale bootstrap re-sampling. Annals of Statistics 32:2616-2641. |
|
|
Soderstrom L, Rosenblad A, Adolfsson ET, Saletti A, Bergkvist L (2014). Nutritional status predicts preterm death in older people: a prospective cohort study. Clinical Nutrition 33:354-359. |
|
|
Sood A, Qualls C, Schuyler M, Arynchyn A, Alvarado JH, Smith LJ, Jacobs DR Jr (2013). Adult-onset asthma becomes the dominant phenotype among women by age 40 years. The longitudinal CARDIA study. Annals of the American Thoracic Society 10(3):188-197. |
|
|
Stegmary B, Thamm M, Tuomilethto J, Vanuzzo D, Vescio F (2003). Hypertension prevalence and blood pressure levels in six European Countries, Canada and Inited States. JAMA 289:2363-2369. |
|
|
Suzuki R, Shimodaira H (2006). Pvclust: an R package for assessing the uncertainty in hierarchical clustering. Bioinformatics 22(12):1540-1542. |
|
|
Tang Y, Horikoshi M, Li W (2016). Ggfortify: Unified Interface to Visualize Statistical Result of Popular R Packages. The R Journal 8(2):474. |
|
|
Thomsen SF, Ulrik CS, Kyvik KO, Larsen K, Skadhauge LR, Steffensen I, Backer V (2005). The incidence of asthma in young adults. Chest 127(6):1928-1934. |
|
|
Tukey J (1949). Comparing Individual Means in the Analysis of Variance. Biometrics 5(2):99-114. |
|
|
William JC, Mark EJ, Myrle MJ (1981). A comparative study of tests for homogeneity of variances, with applications to the outer continental shelf bidding data. Technometrics 23(4):351-361. |
|
|
Wolf-Maier K, Cooper RS, Banegas JR, Giampaoli S, Hense HW, Joffres M, Kastarinen M, Poulter N, Primatesta P, Rodriguez-Artalejo F, Stegmayer B, Tuomilehto J, Vanuzzo D and Vescio F (2003). Hypertension prevalence and blood pressure levels in 6 European countries, Canada and the United States. JAMA, 289, 2363-2369. |
|
|
Whelton PK (1994). Epidemiology of hypertension. Lancet 344(8915):101-106. |
|
|
World Health Organization (WHO) (2010). Guidelines for the treatment of malaria. Geneva: WHO. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


