Full Length Research Paper

ABSTRACT
Collodiaphyseal angle (CDA) is the angle formed between the femoral neck axis and the diaphysis axis. The aims of this study were to determine the normal range of collodiaphyseal angle in adults and to determine any difference in the collodiaphyseal angle between right and left femur and also between sexes. 340 subjects consisting of 170 (50%) males and 170 (50%) females were included in this study. Plain radiographs were taken with the patients lying supine and the medial malleoli touching each other to prevent the hips being laterally rotated. Films were shot at a film focal distance (FFD) of 90 cm to minimize magnification. Measurements were taken with calibrated ruler and the collodiaphyseal angle was measured using goniometer. Results showed a normal range of CDA among Nigerian males as mean ± SD of (133.2° ± 7.6) for the right and mean ± SD of (131.1° ± 7.3) for the left. In females, it was (125.1° ± 6.9) on the right and (123.0° ± 6.9) on the left. Based on the study, coxa vara and coxa valga could be diagnosed on the normal range of collodiaphyseal angle in Ile-Ife (118° -145° in males and 110° -138° females). There is also sex variation and difference in CDA between right and left femur.
Key words: Collodiaphyseal angle, coxa vara, coxa valga.
INTRODUCTION
The CDA (collodiaphyseal angle, angle of inclination) corresponds to the angle formed between the femoral neck axis and the diaphysis axis (Vemavarapu et al., 2016). This differs from the anteversion angle (angle of declination) which is the angle formed by the femoral condyles plane (bicondylar plane) and a plane passing through the centre of the neck of femoral head (Akman et al., 2017).
Several studies have been done on the CDA. It is widest at birth and diminishes until adolescence (Akman et al., 2017). Most of these studies showed regional and racial variations (Buford Jr. et al., 2014; Khan and Saheb, 2014; Romanes, 2012). The CDA was reported to be 120° (Khan and Saheb, 2014), some 125° (Romanes, 2012; Adekoya-Cole et al., 2016), 126° (Vemavarapu et al., 2016) among the Caucasians and over 130° (Gilligan et al., 2013; Otsianyi et al., 2011; Hamilton, 1982; Igbigbi, 2003) among the black Africans, Southern Chinese and native Indians. The inclination of the neck with the femoral shaft has also been shown to vary among sexes (Gilligan et al., 2013; Hamilton, 1982; Igbigbi, 2003; Bhosale and Zambare, 2013). It is less in females with shorter legs and wider pelvis. In the long-legged male, the shaft is nearer vertical and the neck lies more in line with the shaft. In the female, it makes less or obtuse angle (Gilligan et al., 2013; Otsianyi et al., 2011; Hamilton, 1982; Bhosale and Zambare, 2013). It also varies with age, diminishing from birth to puberty (Adekoya-Cole et al., 2016; Nwoha, 1991), from one region of a country to another (Bhosale and Zambare, 2013) and with stature of individual (Tahir et al., 2001). Several studies of the CDA has been done in Mongoloids (Hamilton, 1982; Bhosale and Zambare, 2013) and Caucasians (Vemavarapu et al., 2016; Gilligan et al., 2013; Hamilton, 1982) but few studies on the black population. There is a need to emphasize the importance of this angle since the increase or the reduction of this angle can imply a pathological process. The increase in CDA is called coxa valga and the reduction coxa vara.
Many imaging methods have been used to determine the CDA such as X-ray, computerized tomography, nuclear magnetic resonance and fluoroscopy (Otsianyi et al., 2011; Hamilton, 1982; Bhosale and Zambare, 2013). These studies have shown that plain radiograph method correlated strongly with other imaging techniques and it is in view of this that plain radiographic method which has the lowest cost is used in this study to determine the normal range of collodiaphyseal angle in adults. We therefore set to determine the normal range of collodiaphyseal angle in adults and to determine any difference in the collodiaphyseal angle between right and left femur and also between sexes.
MATERIALS AND METHODS
This is a prospective study that extended from July, 2006 to January, 2008. Three hundred and forty (340) plain anteroposterior radiographs of the pelvis taken at Obafemi Awolowo University Teaching Hospital, Ile - Ife were used. This comprised 170 male subjects and 170 female subjects making a total of 340 right femora and 340 left femora. Only radiographs that showed preservation of the Shenton’s line which is an uninterrupted line from the inferior border of the femoral neck to the inferior border of the superior pubic ramus and no obvious deformities or fractures and meet the criteria required for the measurements of the collodiaphyseal angles, were used. Also, only radiographs that showed both hip and femoral necks were used. Plain radiographs were taken with patient lying supine and the medial malleoli touching each other to prevent the hips laterally rotated which can increase the collodiaphyseal angle. Films were shot at a film focal distance (FFD) of 90 cm to prevent magnification. In all the cases, radiographs were placed on radiograph viewers for clear visualization. On each radiograph was placed a transclucent paper through which details of the underlying films were seen clearly. Tracing of the head and neck and shaft was done. The measurements were taken with calibrated ruler and the collodiaphyseal angle was measured using a goniometer. All measurements were in standard international unit (S.I.). The measurements that were taken are:
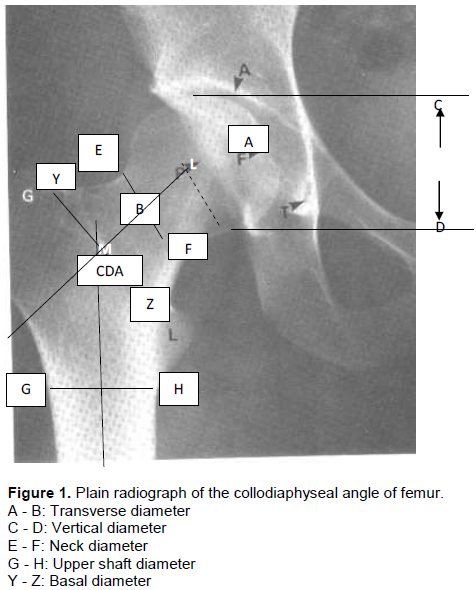
i) Transverse diameter (TD) of the head: A-B in Figure 1 - From the fovea centralis transversely to the junction with the neck.
ii) Vertical diameter (VD) of the Head: C-D in Figure1 - From the highest point to the lowest point vertically on the head.
iii) Neck diameter (ND): E-F in Figure 1 - This is the subcapital part. It measures the diameter of the narrowest part.
iv) Upper shaft diameter USD: G-H in Figure 1 - Transverse line passing through the lower pole of lesser trochanter.
v) Basal diameter BD: - Y-Z in Figure 1: Measured at the base of neck.
vi) Axis of Neck: A line that joins the midpoint of the head (L) with the midpoint of the basal diameter (M).
vii) Axis of the shaft: A vertical line that passes through the midpoint of USD (N).
viii) CDA: Angle formed by the axis of the neck with the axis of the shaft. This was measured by goniometer.
RESULTS
Figure 2 shows the pie chart of CDA in females. In RCDA, the group with CDA of 120° to 129° constituted the majority with a percentage of 56.5%. The least group are those with CDA of 110° to 119° with a percentage of 18.8%. In LCDA, the group of 120° to 129° also constituted the majority with a percentage of 56.5% while the least group is 110° to 119° with a percentage of 18.8%. Figure 3 shows the pie chart of CDA in males. In RCDA, the group 140° to 149° constituted the majority with 35.3% while the group 130° to 139° constituted the least with a percentage of 30.0%. In LCDA, the groups 130° to 139° constituted the majority with 44.7% while the group 110° to 119° constituted the least with a percentage of 4.7%.
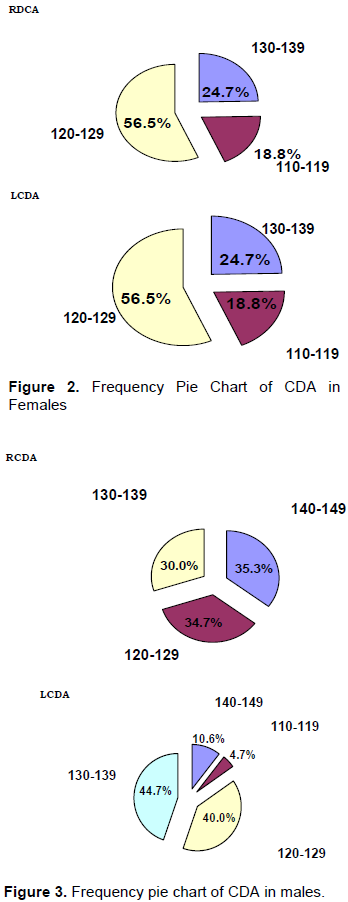
Table 1 shows the student ‘t’ test between the mean CDA in the right and left femora in male. It was observed that the RCDA was significantly greater than the left with a P value < 0.001. Table 2 depicts the student ‘t’ test for the significance of difference between mean CDA in the right and left femora for female. The RCDA was found to be significantly greater than the LCDA with a P-value < 0.001.
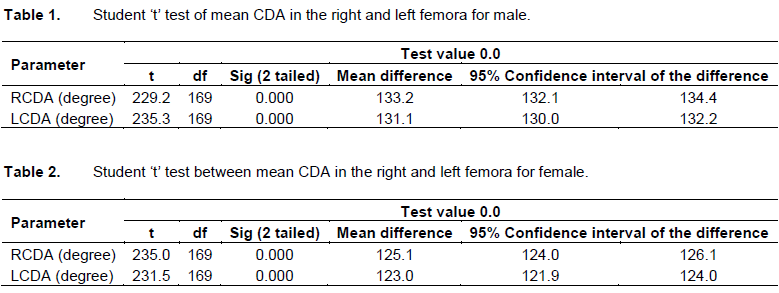
Table 3 shows the student ‘t’ test between the mean CDA in males and females. It was observed that the RCDA was significantly greater in males than in females with P< 0.001. Similarly, the LCDA was significantly greater in males than in females (P< 0.001). Table 4 shows the student ‘t’ test between the mean CDA in the right and left femora in male. It was observed that the RCDA was significantly greater than the left with a P value < 0.001.
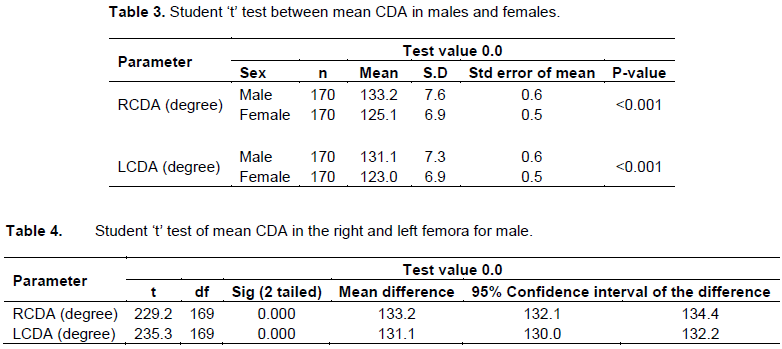
Table 5 depicts the student‘t’ test for the significance of difference between mean CDA in the right and left femora for female. The RCDA was found to be significantly greater than the LCDA with a P-value < 0.001.

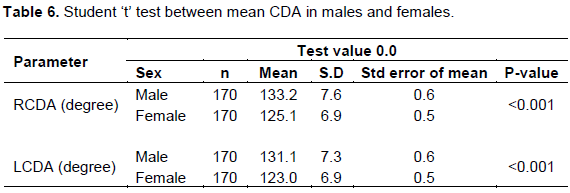
Table 6 shows the student ‘t’ test between the mean CDA in males and females. It was observed that the RCDA was significantly greater in males than in females with P< 0.001. Similarly, the LCDA was significantly greater in males than in females (P< 0.001).
DISCUSSION
This study has shown that the collodiaphyseal angle is greater in males than in the females. This sex variation was also observed by Singh et al., 1986, Tahir et al (2001) in Maiduguri and Igbigbi et al (2003) in Kenya and Uganda. The higher collodiaphyseal angle in males has been explained by the larger physique of males compared with their female counterparts. It may also be due to a more muscular activity in the males. The results also show a difference between the right and left collodiaphyseal angle, in which the collodiaphyseal angle is greater on the right than the left. This has also been observed by Singh et al., 1986, Tahir in Maiduguri (2001), and Igbigbi (2003) in Kenya and Uganda. The higher CDA on the right than the left may be associated with the handedness of these patients in which most people are right handed with more physical activity on that side.
Among patients of the same sex, it was observed that there is a wide range of CDA in them. While some have a low CDA, others have a high CDA. This may be attributable to the different stature or physique of these individuals. In the tall individuals, the shaft is nearer vertical and the neck lies more in line with the shaft, therefore they will have a higher collodiaphyseal angle (Vemavarapu et al., 2016; Adekoya-Cole et al., 2016; Nwoha, 1991; Tahir et al., 2001). However, this was not noticeable in this work. The work of Singh et al.,1986, supported by the present work, has shown that the mean collodiaphyseal angle reported for Nigerians (133°) is greater than that of Indians reported by Singh and Singh, 1975 (125°), for whites by Buford et al., 201 4(120°). Adekoya-Cole et al., 2016 (126°) and Hamilton (1982) (125°). This suggests that the black race has a higher collodiaphyseal angle than Mongoloids. This may be due to the black African babies being carried astride the back of their mothers with legs widely abducted while the angle in Ile - Ife (118° to 145° in males and 110° to 138° in females). There is a sex variation in collodiaphyseal angle and also a difference between right and left collodiaphyseal angle. Caucasians swaddle their babies and carry them with legs together, hips and knees fully extended. It may also be due to undetermined genetic and dietary factors.
From this study, coxa vara and coxa valga could be diagnosed based on the normal range of collodiaphyseal
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adekoya-Cole TO, Akinmokun OI, Soyebi KO, Oguche OE (2016). Femoral neck shaft angles: A radiological anthropometry study. Niger. Nigerian Postgraduate Medical Journal 23(1):17. |
|
|
Akman A, Demirkan F, Sabir N, Oto M, Yorykoglu C, Kiter E (2017). Femoral bowing plane adaptation to femoral anteversion. Indian Journal of Orthopaedics 51(1):49. |
|
|
Bhosale RS, Zambare BR. (2013). Sex determination from femur using length of femur in Maharashtra. Journal of Dental and Medical Sciences 3.4:01-03. |
|
|
Buford Jr WL, Turnbow BJ, Gugala Z, Lindsey RW (2014). Three-dimensional computed tomography–based modeling of sagittal cadaveric femoral bowing and implications for intramedullary nailing. Journal of Orthopaedics 28(1):10-16. |
|
|
Gilligan I, Chandraphak S, Mahakkanukrauh P (2013). Femoral neckâ€shaft angle in humans: variation relating to climate, clothing, lifestyle, sex, age and side. Journal of Anatomy 223(2):133-151. |
|
|
Hamilton WJ (1982). Textbook of Human anatomy. 2nd ed. London: Macmilliam Press P 117. |
|
|
Igbigbi PS (2003). Colloâ€diaphysial angle of the femur in East African subjects. The official Journal of the American Association of Clinical Anatomists and the British Association of Clinical Anatomists 16(5):416-419. |
|
|
Khan SM, Saheb SH (2014). Study on neck shaft angle and femoral length of south Indian femurs. International Journal of Anatomy Resources 2(4):633-635 |
|
|
Nwoha PU (1991). The collodiaphyseal angle of the femur in adult Nigerians. African Journal of Medicine and Medical Sciences 20(2):143-147. |
|
|
Otsianyi WK, Naipanoi AP, Koech A (2011). The femoral collodiaphy-seal angle amongst selected Kenyan ethic groups. Journal of Morphological Science 28(2):129-131. |
|
|
Romanes GJ (2012). Cunningham's Textbook of Anatomy.12th ed. Oxford: Oxford University Press P 127. |
|
|
Singh SP, Ekandem GJ, Ani OEO, Onuba O (1986). A study of the collodiaphyseal angle of the femur in Nigerians. West African Journal of Anatomy 1:28-32 |
|
|
Singh SP, Singh S (1975). Collodiaphyseal angle of the femur in North Indians. Indian Medical Gazette 15:11-4. |
|
|
Tahir A, Hassan AW, Umar IM (2001). A study of the collodiaphyseal angle of the femur in the North-Eastern Sub-Region of Nigeria. Nigerian journal of medicine: Journal of the National Association of Resident Doctors of Nigeria 10(1):34-36. |
|
|
Vemavarapu M, Kothapalli J, Kulkarni V (2016). Estimation of collo-diaphyseal angle of femur by Martin's dioptrograph: A comparative study. International Journal of Anatomy and Research 4(1):1772-1776. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


