ABSTRACT
Rabies is a fatal neglected viral zoonosis which causes encephalitis in many warm-blooded animals and humans. It is an incurable disease once the clinical signs appear. However, it can be prevented via vaccination and community awareness. This study was therefore designed to determine the level of community knowledge, attitude and practices (KAP) regarding rabies. Cross sectional study was conducted from December 2016 to January 2017 in Dedo district, Jimma zone, southwestern Ethiopia. Multistage sampling technique was employed for selection of sample unit and data were collected from 135 household by face-to-face interview using a semi structured and validated questionnaire. Logistic regression was used for assessing the association of independent variable with KAP score. Out of 135 participants interviewed, 71.1% were urban and 57% were male respondents. All (100%) participants had heard about rabies and 88.9% were aware that rabies is zoonotic. However, there were misperceptions about the causes, transmission and incubation period of rabies. Overall KAP score revealed that 51.9% of the respondents had a good KAP, whereas 48.1% was found to have poor KAP score. Multivariable analysis showed that a good KAP score was significantly higher in male than female (OR= 37.16, CI=4.7- 92.1, p= 0.001), in age group >46 years than 15 to 30 years (OR=8.9, CI=1.6-47.2) in urban than rural residents (OR=4.35, CI=1.3-14.14, p= 0.014), education (P= 0.040), in respondent who were at secondary school education level than illiterate (OR=7.7, CI=1.05 - 56.64), in dog owners than those who had no dog (OR=2.9, CI=1.12-7.93, P=0.029), and in trained respondents than non-trained respondents (OR=3.37 CI=1.17-9.69, p=0.024). Generally, the overall, KAP score recorded in this study is an indication of low overall awareness level in the study area. This reflects the urgent need for rabies awareness programmes within the community. Thus, close collaboration of public health, veterinary sector and local authorities is a key element for preventing this fatal incurable disease.
Key words: Attitudes, knowledge, rabies, practices, Dedo.
Rabies is an acute viral infection of the central nervous system, caused by a lyssavirus in the family Rhabdoviridae (Nilsson, 2014). It is a fatal neglected viral zoonosis which causes encephalitis in many warm-blooded animals and humans. This virus is a highly neurotropic pathogen that typically leads to mortality of infected animals and humans. Globally, it is estimated that at least 55,000 people die of rabies each year (Andrea and Jesse, 2012). Wild animals serve as a large and mainly uncontrollable reservoir of sylvatic rabies, which is an increasing threat to the human population and domestic animals in many countries (Rupprecht et al., 2002). Worldwide, the dog is the principal vector in transmitting rabies to human, irrespective of whether the reservoir hosts are wild animals or dogs themselves (Williams and Barker, 2001; Abbas et al., 2011).
The virus is present in the saliva of affected animals, and the most frequent method of transmission to humans is by bites, scratches or licks from infected animals in open wounds or on mucosal membranes (Jackson, 2010; Depani et al., 2012; WHO, 2013; Nilsson, 2014). The clinical features of rabies are similar in most species, but there is great variation between individuals. Following the bite of rabid animal, the incubation period varies from 5 days to several years (usually 2 to 3 months; rarely more than 1 year) depending on the amount of virus in the inoculum, the density of motor endplates at the wound site and the proximity of virus entry to the central nervous system (WHO, 2013).
Rabies is one of the most neglected infectious diseases affecting mainly the low and middle income countries (Abbas et al., 2011). It constitutes a serious public and animal health problem in Africa including Ethiopia. In Ethiopia, rabies has been known for centuries in society as “Mad Dog Disease (Fekadu, 1997) and has been recorded scientifically since 1903 (Pankhrust, 1990). To date, rabies is an important disease in Ethiopia both in human and animals (Tschopp et al., 2002; Deressa et al., 2010; Yimer et al., 2016; Teklu et al., 2017). In four-year retrospective study by Teklu et al. (2017) in Northwestern Tigray, the incidence of human rabies exposure cases calculated per 100,000 populations was 35.8, 63.0, 89.8 and 73.1 in 2012, 2013, 2014 and 2015, respectively.
Rabies is incurable once the clinical signs of the disease appear (Deressa et al., 2010). However, it is possible to prevent a person exposed to the virus from getting ill to rabies by neutralizing virus with antibodies before the virus invades the nervous tissue. This is done through vaccination and/or use of immunoglobulins, so called post-exposure prophylaxis (PEP) (Permpalung et al., 2013; Nilsson, 2014). Controlling rabies in dogs, and especially free-roaming (stray) dogs, is also the ï¬rst priority for prevention of human rabies (Nilsson, 2014). Moreover, successes of rabies control through mass vaccination of dogs have been reported in South America and Asia (Abbas et al., 2011). Vaccinating 70% of the dog population will eliminate dog rabies and hence human rabies (Cleaveland et al., 2014).
Community awareness about rabies has significant role in rabies prevention and control (Chernet and Nejash, 2016; Abdela and Teshome, 2017). Knowledge, attitudes and practices (KAP) studies have been used widely to enhance community knowledge and thus change attitude and improve practices that may aid in disease prevention and control (Sambo et al., 2014; Tiembré et al., 2014; Digafe et al., 2015; Abdela and Teshome, 2017). Despite the endemic nature of rabies in Ethiopia, little is known about level of community awareness in Ethiopia in general and in Dedo in particular. However, for efficiently increasing awareness, the knowledge gap among the community should be identified and targeted. Thus, this KAP study aimed at generating information that will help to identify knowledge gaps and act as baseline data for evaluation of community awareness; thereby helps in planning and implementation of rabies control programs.
Study area
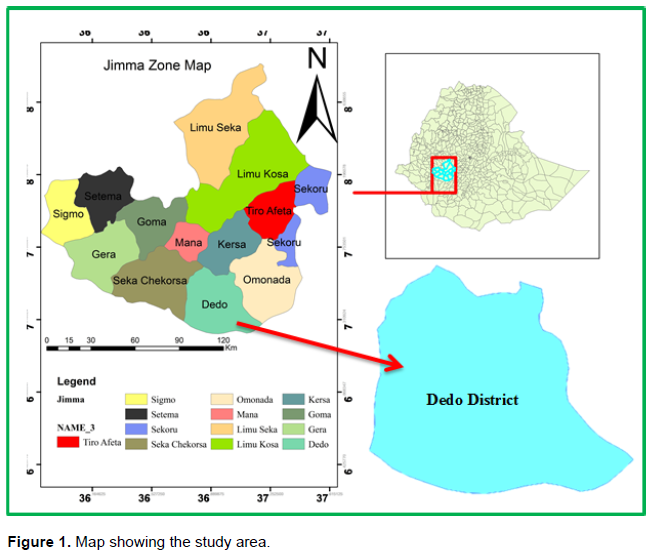
The study was conducted from December 2016 to January 2017 in Dedo district. Dedo is one of the district in Jimma zone of Oromia regional state, southwestern Ethiopia. It has an area of about 1459.1 km2. Dedo shares common boundaries with Omo Nada, Kersa and Seka Chekorsa district, and regional state of Nations, Nationalities and Peoples of South Ethiopia (Figure 1). Dedo is located at distances of 12 km from Jimma town. Jimma town is the capital of jimma zone and found at distance 352 km from Addis Ababa, the capital of Ethiopia. Topographically, mountains, plateaus, hills, plains and valleys characterize the district. About 63.1, 13.6 and 9.3% of the district’s total area were arable, gazing and forest lands, respectively. The altitude of this district ranges from 880 to 2400 m above sea level. Furthermore, this district is known by mixed crop – livestock agricultural production system. The 2007 national census reported a total population for Dedo district to be of 288,457, of whom 143,935 were men and 144,522 were women; 5,755 or 2% of its population were urban residents and majority of the inhabitants were Muslim, with 92.98% of the population.
Study methodology
Community based cross-sectional study was conducted from December 2016 to January 2017 to assess the knowledge, attitude and practice towards rabies in Dedo district. The community of Dedo district who are above 15 years and lived in the district for at least six months were included in this study. The required number of population to be sampled was calculated using the formula given by Arsham (2005). N = 0.25 / SE2, Where N = sample size, S = standard error, 5%. Accordingly, the required sample size was 100. However, to increase the precision and representativeness, the sample size was increased, 135. The calculated sample was proportionally distributed to the selected kebele based on their number of households.
A multi-stage sampling technique was employed for the selection of the sampling units. From the entire study, population in the district five kebeles (the smallest administrative unit) were selected by simple random sampling methods. Then, the household in the selected kebeles was further selected using a systematic random sampling technique. Finally, from all the eligible respondents in a household, only one was selected randomly for the interview. However, in the absence of eligible respondent in a given household, a replacement was immediately made by an individual in the next household until required sample size was obtained.
Data were collected by face-to-face interview by using a semi structured and pre-tested questionnaire. The questionnaire was first prepared in English and translated to Afaan Oromo for appro-priateness and easiness in approaching the study participants. Before the interview begun, they were briefed about the purpose of the study and asked for their consent. Only voluntary participants were involved in the study. All the information obtained from the study participants was kept confidential.
For validation of questionnaire, a sample of 15 randomly selected individuals in the study area who are not included in the main study was used. The questionnaire was assessed for its understandability, clarity, completeness, reliability, and sociocultural acceptability and the edited as required. The questionnaire had different sections including socio-demographic factors like age, sex, marital status, religion, monthly income, educational status and occupation. Moreover, the questionnaire also incorporated questions concerning the knowledge about rabies aetiology, transmission, clinical manifestations, prevention and control measure.
For assessing the community knowledge, attitude and practices (KAP) about rabies each respondent were asked for twenty questions regarding cause, sources, mode of transmissions, clinical singes, prevention practices and treatment measures. The questions were multiple choices question with both open and close ended. Respondents who answered the questions correctly had got one mark and zero for incorrect or do not know responses. Then, the responses for which respondents give correct answer was counted and scored.
This score was then pooled together and the mean score was computed to determine the overall KAP of respondents. Respondents who score greater than or equal to the mean value (Mean= 11.33, SD=2.185) were grouped to good KAP and coded as 1 whereas, the respondent who scored less than the mean value were grouped to poor KAP level and coded as 0.
Data management and analysis
After collecting, the data were cleaned and checked for its completeness and entered into Microsoft Excel 2010 spread sheet. The data generated were analyzed using the Statistical Package for Social Science (SPSS) Version 20.
The descriptive statistics was used for calculating frequency and percentage of both dependent and independent variable. Logistic regression was used for calculating the association between independent variables and dependent variable (KAP scores) of community regarding rabies. A 95% confidence interval of the OR and p-values were used to describe statistical significance associations. The association is judged as significant when p- value is less than 0.05.
Socio demographic character of the participants
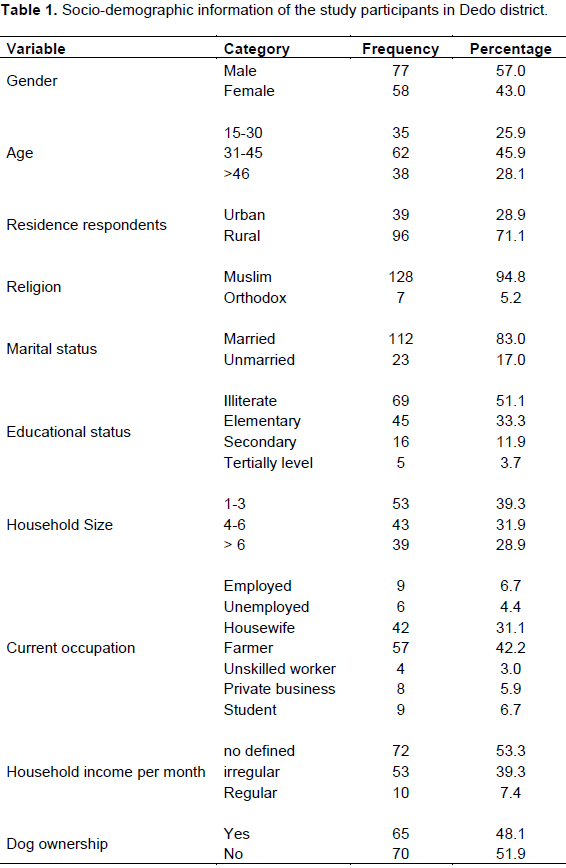
A total of 135 community members were interviewed during the study period and all respondents were responded to the questioner. The majority of the respondents in this study were males 77 (57.0%), while the number of females was 58 (43.0%). From all participants of the study, about 83.0% (112) were married and 17.0% (23) were unmarried. The ages of respondents were classified as 15-30, 31-45 and above 46 years old, which comprises about 35 (25.9%), 62 (45.9%) and 38 (28.1%), respectively. The majority of the respondents were rural, 96 (71.1%) while that of urban was 39 (28.9%). Concerning the religion, the majority of respondents were Muslim 128 (94.8%), followed by Orthodox 7 (5.2%). Regarding the educational status of respondents, 51.1% were illiterate, 33.3% had elementary education, 11.9% had secondary education, and the rest 3.7% had tertially education. With regards to the family size, about 53 (39.3%) participants were from family size of one to three persons and similarly most of the respondents, 57 (42.2%) were farmers and 72 (53.3%) had no defined income. From the whole respondents/ participants (135) in this study, about sixty five (48.1%) had dogs while seventy (51.9%) respondents had no dogs. Socio demographic characters of the participants are summarized in Table 1.
Knowledge of respondents in relation to cause, host range, clinical signs and transmission of rabies
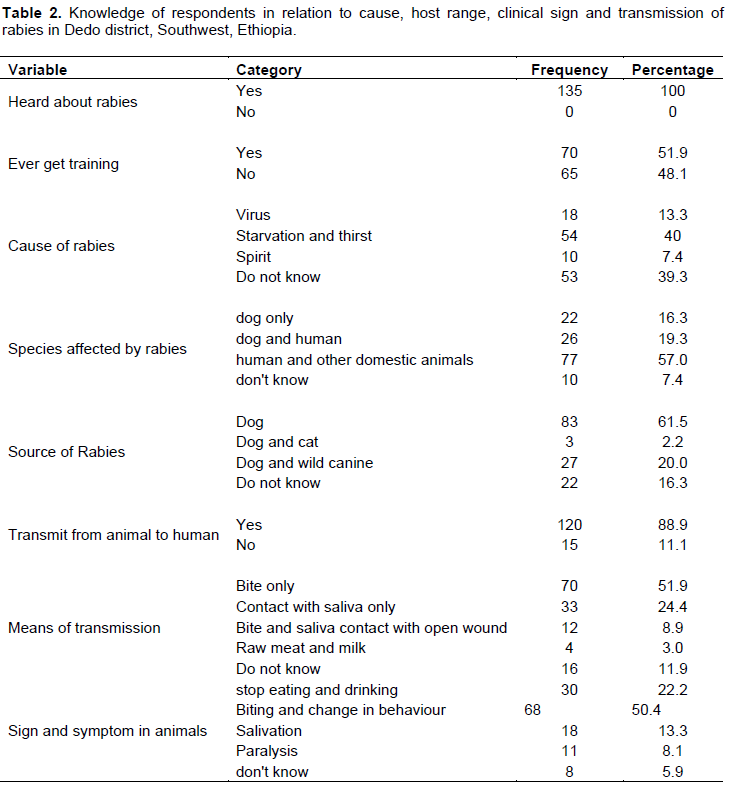
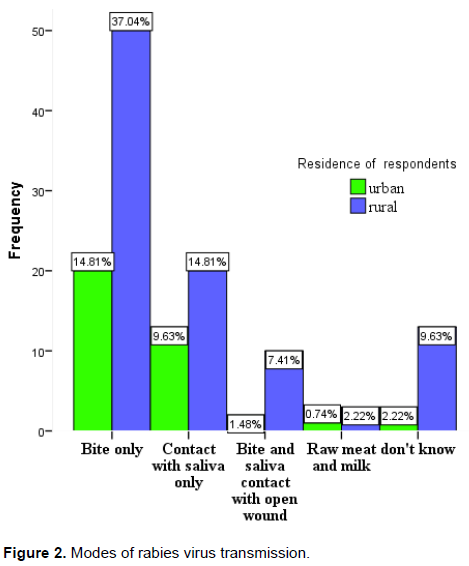
The knowledge on cause, host range, clinical signs and transmission of rabies were summarized in Table 2. All respondents (100%) had heard about rabies. However, only small proportion (13.3%) of respondents knew the causative agent of rabies. 39.3% of the participants responded that they do not know the causative agent and 40% were found to have misperception about causative agent which was starvation and thirst. The majority of study participants (57.0%) knew that rabies can affect both human and other domestic animals and mentioned dogs (61.5%) as a major source of rabies. Moreover, 88.9% of respondents knew that rabies can be transmitted from animal to human. However, most of respondents (51.9%) replied dog bite as the only transmission method. Bite and saliva contact with open wound were replied by 8.9% of respondents of which 7.41% were rural residents and 1.48% were urban residents (Figure 2). Regarding the clinical signs of rabies in animals, biting and change in behaviour were resported by 50.4% of the participants.
Community attitudes and practices regarding rabies
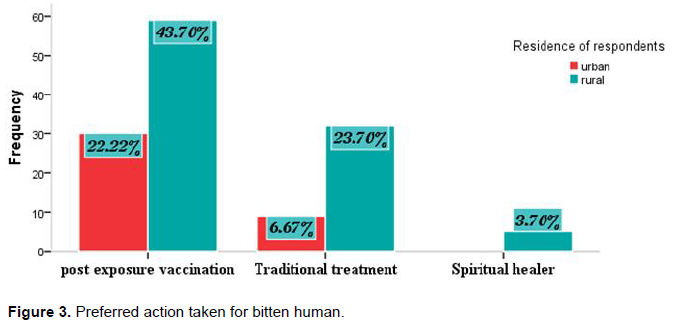
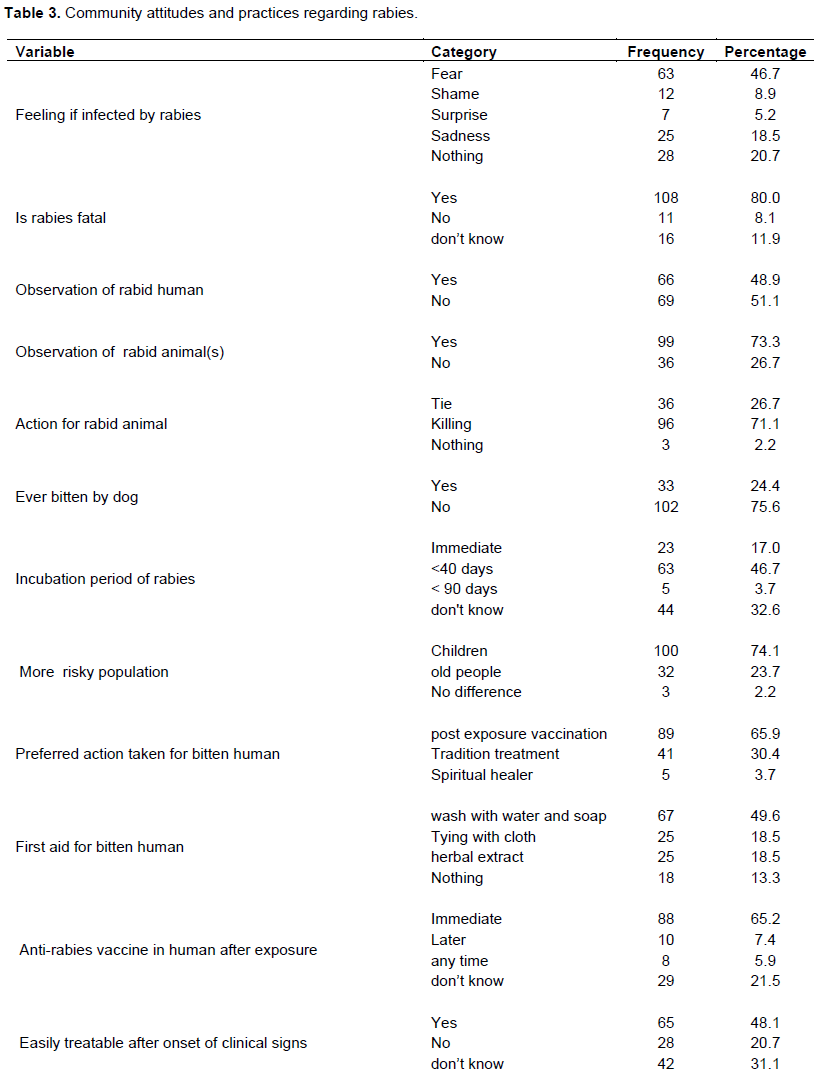
The result of the study revealed that majority of the respondents (80.0%) considered rabies as a fatal disease and almost half (46.7%) resported that they fear rabies. Regarding observation of rabid animal(s) and human(s), 73.3 and 48.9% of the participants observed rabid animal(s) and human(s), respectively. Furthermore, out of total interviewed participants 71.1% respondents replied killing as the preferred method for rabid animal(s) and 33 (24.4%) of respondents had experienced a dog bite at least once in their life. Regarding incubation period of rabies, the most frequently mentioned incubation period was less than 40 days (46.7%). Furthermore, children were mentioned by 100 (74.1%) of the respondent to be at higher risk than old people. Regarding the preferred action taken for bitten human, post exposure vaccination was responded by 89 (65.9%) of the participants whereas, traditional treatment was responded to by 41 (30.4%) of the participants. Moreover, 23.7% of the respondents were rural residents and 6.67% were urban residents (Figure 3). Moreover, 49.6% of the respondents reported that they would wash the wound using soap and water as a first aid for bitten human whereas, tying with cloth and application of herbal extract were reported by 18.5% of the respondents. 66.6% of the participant considered rabies not to be prevented by vaccination and 68.8% do not believe that eliminating stray dog or confining dog helps to prevent rabies. The respondent’s attitudes and practices towards rabies are summarized in Table 3.

Factors associated with knowledge, attitudes and practices (KAP)
The overall knowledge, attitudes and practices (KAP) revealed that 51.9% of the respondents had a good KAP, whereas 48.1% was found to have poor KAP score. Table 4 shows the multivariable logistic regression analysis output of community knowledge attitude and practice (KAP) in relation to socio-demographic characteristics. Multivariable analysis revealed that good KAP score was significantly associated with gender being higher in males than females (OR= 37.16, CI=4.7- 92.1, p= 0.001), in age group >46 years than 15- 30 years (OR=8.9, CI=1.6-47.2) in urban than rural residents (OR=4.35, CI=1.3-14.14 p= 0.014). Furthermore, the association of education level with KAP score revealed statically significant difference (P= 0.040). The respondent who were at secondary school education level were found to have 7.7 times more good KAP score than illiterate (OR=7.7, CI=1.05 - 56.64). Significantly higher overall knowledge on rabies was also found in dog owners than those who had no dog. Dog owners were found to have 2.9 times more good KAP score than those who had no dog (OR=2.9, CI=1.12-7.93, P=0.029). The participants who got training on rabies were found to have significantly higher good KAP score than non-trained participants. The odd of higher good KAP score in trained respondents was 3.37 times more likely than non- trained respondents (OR=3.37 CI=1.17-9.69, p=0.024).
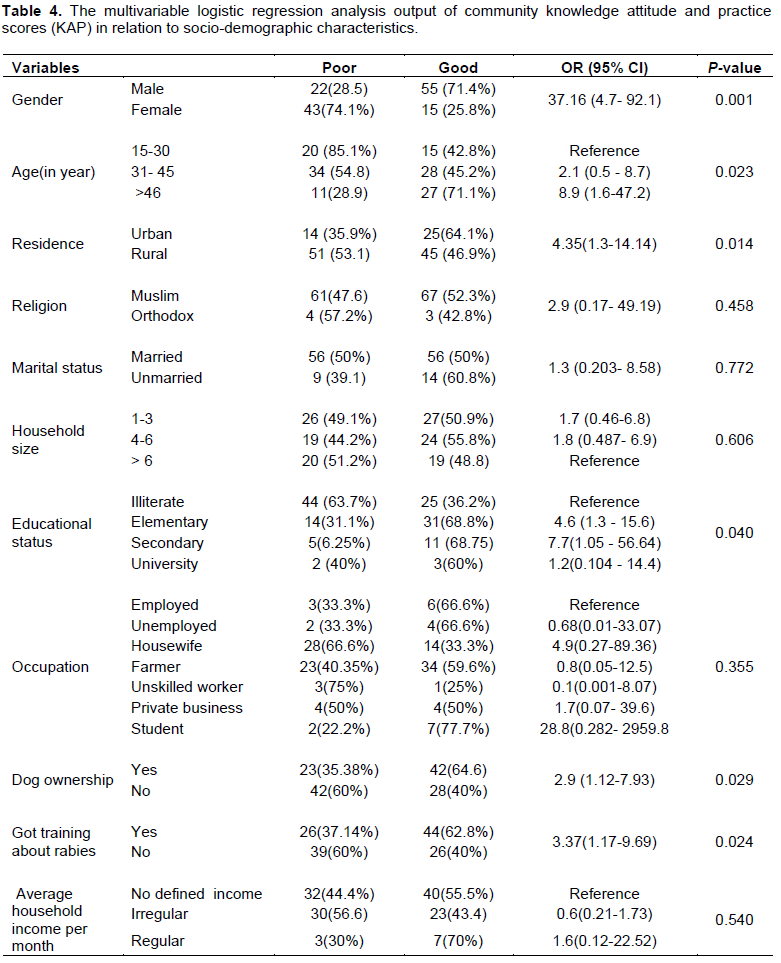
Insignificantly higher good KAP score was observed in Muslim respondent than orthodox (OR=2.9, CI=0.17- 49.19, P=0.458), in unmarried than married (OR=1.3, CI= 0.203- 8.58, P=0.772) and in respondent with household size of 4-6 than above 6 (OR=1.8, CI = 0.487- 6.9). Moreover, the occupation of the respondents were also found to be not significant (P= 0.355). The highest good KAP score was observed in students than those that were found to have 28.8 times more overall knowledge than employed (OR=28.8, CI=0.282- 2959.8). Regarding the the association of averege household income per month and KAP score of respondents, no statically significant difference was observed (p= 0.540) (Table 4).
This study revealed that community in Dedo district are familiar with general information on rabies as 100% of the respondent had heard about rabies. This is in agreement with study by Singh and Choudhary (2005) in rural community of Gujarat, India, Digafe et al. (2015) in Gondar Zuria District and Yalemebrat et al. (2016) in Debark district, North Gondar, Ethiopia who reported 98.6, 99.3 and 100% awareness about rabies, respectively. Besides, Serebe et al., (2016), Serebe et al. (2014) and Jemberu et al. (2013) also reported a high level of awareness on rabies from different areas of Ethiopia which agrees with the current finding. However, this finding was higher when compared with 68.7% in a survey of knowledge, attitudes and practices about animal bite and rabies in community in India (Ichhupujani et al., 2006), 83% in Addis Ababa residents (Ali et al., 2013).
In the current study, 40% respondents were found to have misunderstanding of the cause of rabies which was starvation and thirst. Similar to this finding, Guadu et al. (2014) reported similar misunderstanding from Bahir Dar town. However, this result is lower as compared to the result of study in and around Dessie town, Ethiopia which was 49.6% (Serebe et al., 2016) and in Debark District, North Gondar, Ethiopia (63.5%) (Yalemebrat et al., 2016). This could be due to awareness difference of the study area and this misperception could be explained by the opinion of asymptomatic rabies carrier dogs in which stressors like starvation and thirst might induce development of clinical rabies in the carrier dogs. But the idea of asymptomatic rabies carrier dogs by itself is a controversial issue (Wilde et al., 2009), and the association of stressors to the development of clinical rabies might be an implausible claim.
In this study, 57.0% respondents knew that rabies could affect human and other domestic animals which is in line with Yalemebrat et al. (2016). However, Guadu et al. (2014) reported a lower result (21.4%) from Bahir Dar town and higher result (71.9%) was also reported in the city of New York, USA (Eidson et al., 2004). The possible reason for this could be due to the availability of different host range, level of awareness and educational status of community.
In the current study, 49.6% of the respondents reported that they would wash the wound using soap and water as a first aid for bitten human(s). This result is lower when compared with study in Debark District (76.4%) (Yalemebrat et al., 2016) and higher as compared to the study conducted in Gondar zuria district (30.7%) (Digafe et al., 2015) and in a rural community of Gujarat, India (31.1%) (Singh and Choudhary, 2005). This difference could be associated with awareness level of the community. This treatment is cheap, readily available and feasible for all to apply. Washing of rabies-infected wounds with soap and water can increase survival by 50% (Radostits et al., 2007). In the current study, 65.9% participants prefer post exposure vaccination for bitten human(s) and 65.2% of the respondent replied that it should be given immediately after exposure. Similarly, the study in Bahar Dar town reported 55.7% response for immediate post exposure vaccination (Guadu et al., 2014). The World Health Organization (WHO) also recommends wound washing and vaccination immediately after contact with a suspected rabid animal which can prevent almost 100% of rabies deaths (WHO, 2013). Regarding incubation period of rabies, the most frequently mentioned incubation period was less than 40 days (46.7%). This misconception about the incubation period indicates that those who believe this incubation period do not seek post exposure prophylaxis once the perceived incubation period has passed. This is serious for rabies-infected individuals where mortality is 100% after development of clinical signs. The incubation period varies from 5 days to several years (usually 2 to 3 months; rarely more than 1 year) depending on the amount of virus in the inoculum, the density of motor endplates at the wound site and the proximity of virus entry to the central nervous system (WHO, 2013). Furthermore, children were mentioned by 100 (74.1%) of the respondents to be at higher risk than old people. This could be due to the fact that children are closely playing with dog at home and even in streets. In addition, elders are well aware of the danger of rabies and look for medical care than children (Aworth et al., 2011). The result of current study revealed that 66.6% participants do not believe in rabies prevention by vaccinating dog and 68.8% of them replied that rabies cannot be prevented by eliminating stray or confining dogs. This is serious knowledge deficiency and community deserves public awareness.
In this study, the overall knowledge, attitude and practice (KAP) score revealed that 51.9% of the respondents had a good KAP. This finding is lower when compared with the study by Guadu et al. (2014) who reported about 64.1% among the community of Bahir Dar town and Yalemebrat et al. (2016) who reported 60.3% in Debark District, North Gondar. This difference could be due to the difference in sample size and level of awareness of community about rabies in the study area.
During analysis of KAP with independent variables, multivariable analysis revealed that KAP score was significantly (p= 0.001) associated with gender being higher in males (71.4%) than females (25.8%). The same proportion of statistical difference on KAP score of male (53.4%) and female (10.75%) was reported in Bahirdar town by Guadu et al. (2014), in Addis Ababa (male, moderate (77.09%) and good (10.55%), female, moderate (73.62%), good (5.08%) (Ali et al., 2013), in Debark District in males (64.6%) in females (54.5%) (Yalemebrat et al., 2016). The statistical significant difference in KAP score between males and females might be due to increased activity of males in their daily life when compared with females and better chance of acquiring correct information about rabies.
Furthermore, the association of education level with overall knowledge about rabies revealed statically significant difference (P= 0.040). The respondent who were at secondary school education level were found to have 7.7 times more good KAP score about rabies than illiterate. This finding was also supported by a study conducted in Bahir Dar (Guadu et al., 2014), in Addis Ababa (Ali et al., 2013) and the studies conducted in Flagstaff, Arizona, USA (Andrea and Jesse, 2012). People with higher education tend to know more about rabies (Palamar et al., 2013), while illiterate persons tend to know less about rabies (Herbert et al., 2012). The possible explanation could be that educated person would have better information access and can easily understand the disease.
Moreover, significantly (P=0.029) higher good KAP score was also found in dog owners than those who had no dog. Dog owners were found to have 2.9 times more KAP score than those who had no dog. This finding is in agreement with Guadu et al. ( 2014) who found higher KAP score in dog owner than those who had no dogs. This may be associated with the adoption of dog owners with dog as it might help to know more about dog and dog disease and better chance of acquiring correct information on rabies.
Raising community awareness level has been mentioned as important tool to control rabies by many scholars (Eshetu et al., 2002; Wudu et al., 2013). In the study area, most of the participant had got training about rabies. In particular, Jimma University has been giving and had given the training through the program called “community based training program (CBTP).” In this study, the participants who got training on rabies were found to have significantly higher KAP score than non-trained participants (p=0.024). The odd of higher good KAP score on rabies in trained respondents were 3.37 times more likely than non-trained respondents. This supported the general fact that awareness creation has paramount role in prevention and control of rabies.
Conclusively, rabies was considered as the disease of both a veterinary and public health importance in the study area. All (100%) respondents had heard about rabies previously and 88.9% of respondents knew that rabies can be transmitted from animal to human. This is good knowledge. However, knowledge deficiency was observed regarding cause, mode of transition and incubation period of rabies. Increased knowledge is especially needed regarding rabies prevention by vaccination of dog, confining and eliminatiion of stray dogs. Furthermore, rabies awareness campaigns and education programs should focus on awareness community especially on first- aid treatments after a dog bite and how rabies is transmitted. Generally, the overall KAP score recorded in this study is an indication of low overall awareness level. Thus, close collaboration and integration of public health, veterinary sector and local authorities is a key element for preventing this fatal incurable disease.
The authors have not declared any conflict of interests.
REFERENCES
|
Abbas SS, Venkataramanan V, Pathak G, Kakkar M (2011). Rabies control initiative in Tamil Nadu, India: a test case for the 'One Health'approach. Int. Health 3(4):231-239.
Crossref
|
|
|
|
Ali A, Yimer EA, Sifer D (2013). A study on knowledge, attitude and practice of rabies among residents in Addis Ababa, Ethiopia. Ethiop. Vet. J. 17(2):19-35.
Crossref
|
|
|
|
|
Andrea M, Jesse D (2012). Community Survey after Rabies Outbreaks, Flagstaff, Arizona, USA. Emerg. Infect. Dis. 18(6):932-938.
|
|
|
|
|
Aworth M, Nwoshu C, Ajumobi O, Okewole P, Okolocha E, Akansi B. (2011). A retrospective study of Rabies cases Reported at Vom Chrisrian Hospital, Plateu State Nigeria, 2006-2010. Niger. J. Vet. 32:366-370.
|
|
|
|
|
Chernet B, Nejash A (2016). Review of Rabies preventions and control. Int. J. Life Sci. 4(2):293-301.
|
|
|
|
|
Cleaveland S, Beyer H, Hampson K, Haydon D, Lankester F, Lembo T, Meslin FX, Morters M, Mtema Z, Sambo M, Townsend S (2014).The changing landscape of rabies epidemiology and control. Onderstepoort J. Vet. Res. 81(2):1-8.
Crossref
|
|
|
|
|
Depani SJ, Kennedy N, Mallewa M and Molyneux EM (2012) Case report: Evidence of Rise in Rabies Cases in Southern Malawi–Better Preventative Measures Are Urgently Required. Malawi Med. J. 24(3):61-64.
|
|
|
|
|
Deressa A, Ali A, Beyene M, Newaye Selassie B, Yimer E, Hussen K (2010). The status of rabies in Ethiopia: A retrospective record review. Ethiop. J. Health Dev. 24(2):127-132.
Crossref
|
|
|
|
|
Digafe RT, Kifelew LG, Mechesso AF (2015). Knowledge, attitudes and practices towards rabies: questionnaire survey in rural household heads of Gondar Zuria District, Ethiopia. BMC Res. Notes 8(400):2-7.
Crossref
|
|
|
|
|
Eidson M, Kate S, Mary K, Charles T, Amy W (2004). Development and evaluation of bat rabies education materials. Evid Based Prev.Med. 1(2):85-91.
|
|
|
|
|
Eshetu Y, Bethelehem N, Girma T, Yared M, Yosef B, Badeg Z, Mekoro B, Abebe B (2002). Situation of rabies in Ethiopia: A retrospective study 1990-2000. Ethiop. J. Health Dev.16(1):105-112
|
|
|
|
|
Fekadu M (1997). Human rabies surveillance and control in Ethiopia. In: Proceedings of the Southern and Eastern Africa Rabies Group Meeting, Nairobi, Kenya.
|
|
|
|
|
Guadu T, Shite A, Chanie M, Bogale B, Fentahum T (2014). Assessment of knowledge, attitude and practices about rabies and associated factors: in the case of Bahir Dar town. Glob. Vet. 13(3):348-54.
|
|
|
|
|
Herbert M, Basha SR, Thangaraj S (2012). Community perception regarding rabies prevention and stray dog control in urban slums in India. J. Infect. Public health 5(6):374-380.
Crossref
|
|
|
|
|
Ichhupujani R, Chhabra M, Mittal V, Bhattacharya D, Lal S (2006). Knowledge, attitude and practices about animal bites and rabies in general community- A multi-centric study. J. Communicable Dis. 38(4):355-361.
|
|
|
|
|
Jackson AC (2010). Why does the prognosis remain so poor in human rabies?. Expert Rev. anti-infect. Ther. 8(6):623-625.
Crossref
|
|
|
|
|
Jemberu WT, Molla W, Almaw G, Alemu S (2013). Incidence of Rabies in Humans and Domestic Animals and People's Awareness in North Gondar Zone, Ethiopia. PLoS Negl. Trop. Dis. 7(5):e2216.
Crossref
|
|
|
|
|
Nilsson M (2014). Effect of rabies education programs on rabies awareness, attitudes towards dogs and animal welfare among children in Lilongwe, Malawi. P 26.
|
|
|
|
|
Palamar MB, Peterson MN, Deperno CS, Correa MT (2013). Assessing rabies knowledge and perceptions among ethnic minorities in Greensboro, North Carolina. J. Wildlife Manag. 77(7):1321-1326.
Crossref
|
|
|
|
|
Pankhrust R(1990). An introduction to the medical history of Ethiopia. The Red Sea Press. Inc. Trenton, New Jersey. pp. 93-101.
|
|
|
|
|
Permpalung N, Wongrakpanich S, Korpaisarn S, Tanratana P, Angsanakul J (2013).Trend of human rabies prophylaxis in developing countries: toward optimal rabies immunization. Vaccine 31(38):4079-4083.
Crossref
|
|
|
|
|
Radostits OM, Gay CC, Hinchcliff KW, Constable PD (2007). Veterinary medicine: a textbook of the diseases of cattle, horses, sheep, pigs and goats.10thed. London. Saunders. pp.1384-1394.
|
|
|
|
|
Rupprecht CE, Hanlon CA, Hemachudha T. (2002). Rabies re-examined. Lancet Infect. Dis. 2(6):327-343.
Crossref
|
|
|
|
|
Sambo M, Lembo T, Cleaveland S, Ferguson HM, Sikana L, Simon C, Urassa H, Hampson K (2014). Knowledge, attitudes and practices (KAP) about rabies prevention and control: a community survey in Tanzania. PLoS Negl. Trop. Dis. 8(12):e3310.
Crossref
|
|
|
|
|
Serebe SG, Tadesse KA, Yizengaw HA, Tamrat SM (2014). Study on community knowledge, attitude and practice of rabies in and nearby Gondar town, North West Ethiopia. J. Public Health Epidemiol. 6(12):429-435.
|
|
|
|
|
Serebe SG, Tadesse KA, Yizengaw HA, Tamrat SM (2016). Study on Community Knowledge, Attitude and Practice of Rabies in and Around Dessie City. J. Public Health Epidemiol. 6(12):429-435.
|
|
|
|
|
Singh SU, Choudhary SK (2005). Knowledge, attitude, behavior and practice study on dog-bites and its management in the context of prevention of rabies in a rural community of Gujarat. Indian J. Community Med. 30(3):81-83.
Crossref
|
|
|
|
|
Teklu GG, Hailu TG, Eshetu GR (2017) High Incidence of Human Rabies Exposure in Northwestern Tigray, Ethiopia: A Four-Year Retrospective Study. PLoS Negl. Trop. Dis. 11(1):e0005271.
Crossref
|
|
|
|
|
Tiembre I, Vroh BBJ, Kouassi P, Attoh-Touré H, Ekra KD, Diane A, Tagliante-Saracino J (2014). Knowledge, attitudes and practices of household heads regarding rabies in the Abobo district (Abidjan, Côte d'Ivoire) in 2008. Sante publique (Vandoeuvre-les-Nancy, France) 26(4):547-553.
|
|
|
|
|
Tschopp R, Bekele S, Aseffa A (2016). Dog demography, animal bite management and rabies knowledge-attitude and practices in the Awash Basin, Eastern Ethiopia. PLoS Negl. Trop. Dis. 10(2):e0004471.
Crossref
|
|
|
|
|
Wilde H, Shantavasinkul P, Hemachudha T, Tepsumethanon V (2009). New knowledge and new controversies in rabies. J. Infect. Dis. Antimicrob. Agent 26:63-74.
|
|
|
|
|
Williams ES, Barker IK (2001). Infectious Disease of Wild Animals. (3rd Ed.). Black well publishing company, USA. pp. 5-2.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2013). WHO Expert Consultation on Rabies: second report (No. 982). World Health Organization.
|
|
|
|
|
Wudu T, Wassie M, Gizat A, Sefinew A (2013). Incidence of rabies in humans and domestic Animals and People's Awareness in North Gondar Zone, Ethiopia. J. PLOS Negl. Trop. Dis. 7(5):2216.
Crossref
|
|
|
|
|
Yalemebrat N, Bekele T, Melaku M (2016). Assessment of public knowledge, attitude and practices towards rabies in Debark Woreda, North Gondar, Ethiopia. J. Vet. Med. Anim. Health 8(11):183-192.
|
|
|
|
|
Yimer E, Newayeselassie B, Teferra G, Mekonnen Y, Bogale Y, Zewde B, Beyene M, Bekele A (2002). Situation of rabies in Ethiopia: a retrospective study 1990-2000. Ethiopian J. Health Dev. 16(1):105-12.
Crossref
|
|



