Full Length Research Paper

ABSTRACT
One of the factors of male infertility is idiopathic oligospermia in which the causative factor is not known. A direct case control, two-centers, prospective, randomized controlled two-arm parallel group trial was carried out to investigate the safety and efficacy of trialed medicine in Shifa-ul-Mulk Memorial Hospital for Eastern Medicine at Madinat-ul-Hikmah, Hamdard University Karach-74600, Pakistan. An assessment was conducted on the coded herbal formula Spermox (Test drug) to treat idiopathic condition of oligospermia; the test drug spermox was compared with Fertilox (Control drug). The idiopathic pathogenic states of spontaneous origin were detected on 62 clinically diagnosed patients. The conclusive findings were significant as improvements were seen in clinical assessment and semen analyses parameters. The value of sperm count per milliliter in spermox was found more than 29 million in 26 patients (p 0-032). It revealed that Spermox is more effective in upgrading the semen quality and quantity when compared with Fertilox for the treatment of idiopathic oligospermia. This is clearly evident that Spermox (Test drug) possesses a more viable value for the treatment of idiopathic oligospermia in comparison to Fertilox (Control drug).
Key words: Oligospermia, herbal medicine, male infertility, prospective, multicentre, randomized, clinical trial.
INTRODUCTION
Oligospermia is the deficiency of spermatozoa in the semen and is the basic cause of male infertility. The qua-lity and quantity of semen having reduced sperm concentration display a marked abnormality in sperm morphology and motility and vitality (Dorland’s Medical Dictionary, 2007; Grimes and Lopez, 2007). The associated risk may be involved in producing condition, including age, infection of Chlamydia trachomatis, Y chromosome deletions due to aberration mitochondrial changes, chemical effects of environmental hazards and hormonal changes (Cavallini, 2006).
Although it is understood that in most cases of oligospermia and idiopathic form there is no direct medical or surgical involvement found to be curative. Despite the fact that it is comprehended that by and large of idiopathic oligospermia, there is no immediate therapeutic or surgical contribution discovered to be remedial at yet. However, the diverse therapeutic methodologies have been attempted. The treatment of idiopathic oligospermia and male infertility by using herbs and unani medicine have largely been undertaken and there are evidence where in natural medicine have proved useful in oligospermia. However, in the traditional medication, the following plants Asparagus racemosus, Mucuna pruriens, Asparagus adscendens, Withania somnifera, and Tribulus terrestris, etc., were used for stress treatment, anxiety, treat bacteria, retardation of the aging process and recovering men’s sexual disorders, and in some cases to address infertility and case of oligospermia (Chittendon, 1956; Hedrick, 1919). These plants were used in spermox for the determination of the spermogenic effect. Spermox is not a commercial product; it is formulated first time for this clinical trial, however, the ingredients of this product is already reported in literature for the said activity.
It has been previously reported that T. terrestris and W. somnifera have good results in oligospermia and male infertility for the improvement of sperm quantity and quality. So by taking advantage, the coded herbal formulation spermox contains a total of five ingredients in which A. adscendens, W. somnifera, A. recemosus, T. terrestris and M. pruriens for the treatment of semen abnormalities causing infertility in man.
A. racemosus were used in this study and it was observed that streptozotocin as well as alloxan induced hyperglycemic rats showed an overall reduced sexual performance. The deleterious effect was significantly ameliorated in animals treated with polysaccharide-rich fraction of A. racemosus. This study validates the traditional claim of using A. racemosus as an aphrodisiac herb for treating sexual dysfunction in males (Mayank et al., 2009).
The rhizomes of white musli (A. adscendens) is an aphrodisiac; its effect is to increase sperm count hence are commonly used for the rejuvenative function (Chopra et al., 1996). Study on W. somnifera concluded that it is a tonic and prescribed in spermatorrhoea. It provides energy and vigour to the body to fight against chronic diseases (Panda and Kar, 1998). T. terrestris was proven to be a spermogenic herb (Mutee et al., 2012). The therapeutic applications of M. pruriens were reported to regulate steroidogenesis and improve semen quality in infertile men (Shukla et al., 2009).
MATERIALS AND METHODS
This is a two-centers, prospective, randomized, open-label, active-controlled study. The trial was completed in July, 2009 to June, 2011. These studies were completed in Shifa Ul Mulk Memorial Hospital for Eastern Medicine, Hamdard University, Karachi and Alshifa Clinic Nazimabad. Only those participants selected who fulfilled inclusion criteria were used. A clinical trial protocol was filled by investigator at the start of treatment. After excluding withdrawal, the total patients who had finished test study were 62.
Semen samples were gathered in sterile tubes by masturbation after a sexual forbearance time of 3 to 5 days. Semen samples were instantly transformed for investigation. The tests were performed by World Health Organization rules standard semen quality parameters (WHO, 2010). The Data Monitoring Committee audited the unblinded information for patient from both centers. The patents received treatment consisted of 96 patients screened; 85 met eligibility criteria and 78 patients agree to participate: coded herbal formulation Spermox prescribed to 32 patients, and 30 were treated with Fertilox. Eight patients in test group and 8 in the control group were excluded from the study because of incomplete follow-up. In order to find out the restorative evaluations of trialed medicines, 62 patients were examined clinically and laboratory investigations were taken during the course of treatment.
Control drug (Fertilox) is a very costly medicine, not so potent and exert some side effects. In order to overcome this problem, there is a great need to find new medicinal agents that have good efficacy and less adverse effects. Herbal medicine could be choice to treat idiopathic oligospermia and considering this option, a formulation has been designed based on literature citation. Therefore, one of the good candidates could be a coded herbal formulation Spermox (Farone and Koenigsberg, 1995).
Patients were categorized in two groups. Group A on test drug (Spermox) and group B on control drug (Fertilox). The duration of study was six-month. Sample was taken randomly to avoid bias in clinical trial. For the correct diagnosis of Idiopathic oligospermia, we had strictly followed WHO criteria based on complete history and semen analysis findings. After treatment, the test was repeated to find out the difference in treatment. Ethical committee clearance for this study was obtained prior the start of clinical trial. All patients gave written, informed consent and the protocol approval was already taken from Ethics Committee of the Faculty of Eastern Medicine, Hamdard University, Karachi, Pakistan according to principles based on the Declaration of Helsinki.
Inclusion criteria
Cases suffering from idiopathic oligospermia were selected and registered. Patients aged 24 to 50 years were included. Cases that have no other disease on routine checkup interfering with the current matter were selected. Infertile patient having sperm count less than 20 Million/ml were the choice of management. Patients were residing in Karachi, Pakistan. All socio-economical classes were included. Fertility test of female were seen to exclude the female, so that ultimate diagnosis is referred.
Patients suffering from uncontrolled hypertension and diabetes mellitus and other chronic diseases were not allowed to participate. Patient having any sexual transmitted diseases were detected besides idiopathic oligospermia. Idiopathic oligospermia coexisted with any partner problem, that is, female factor was also not administered in the study.
Clinical assessment
The patients included in the trial were those reporting to outpatient unit. They were thoroughly examined for clinical signs and symptoms. Their laboratory reports were recorded. Consent of the patients was taken at the first examination, semen analysis was drawn for the estimation of sperm count and motility, and the standard clinical trial proforma was filled for registration. Different parameters, that is, age, duration, and other clinical sign and symptoms base line were studied and compared between two groups at base line and end of therapeutic applications.
Treatment assignment and follow-up
Sixty two patients consented to participate in the study. Pretreatment clinical and laboratory parameters for the treatment groups were noted. The two treatment groups were comparable in efficacy results and side effects of the medicine administered. The clinical analyses were performed in all cases and treatment duration was completed between July, 2009 and June, 2011.
Efficacy measurements
The efficacy measurements involving the two treatments, the herbal medicine and the conventional medicine, were compared. The efficacy was determined using the results of semen analysis.
Statistical analysis
Statistical analysis was performed with SPSS, using excel software and Chi squire test. The Chi squire was used for paired data. All differences were considered statistically significant by generating a ‘p-value’ from Chi squire test statistics. The result with ‘p-value’ less than 0.05 was defined as statistically significant. In ordered to validate the results, the statistical analysis was performed by Chi square; Fisher’s exact test was used to find out the level of significance and to confirm the efficacy of the treatment drugs both in test and control group as Spermox and Fertilox, respectively.
RESULTS
The present investigations were carried out for the verification and comparative analysis of efficacy of these medicines for low sperm count and motility. The therapeutic evaluations of these medicines were conducted on 62 patients at Shifa-ul-Mulk Memorial Hospital, for Eastern Medicine, Hamdard University, Karachi and Alshifa Clinic, Nazimabad. The patients that received treatment consisted of 96 patients screened; 85 met eligibility criteria and 78 patients agree to participate: coded herbal formulation Spermox prescribed to 32 patients, and 30 were treated with Fertilox. Eight patients in the test group and 10 in the control group were excluded from the study, because of incomplete follow-up. In order to find out the restorative evaluations of trialed medicines, 62 patients were examined clinically and laboratory investigations were taken during the course of treatment after excluding the failure cases.
Control drug (Fertilox) is a very costly medicine, not so potent and exert some side effects. In order to overcome this problem, there is a great need to find new medicinal agents that have good efficacy and less adverse effects. Herbal medicine could be the choice to treat idiopathic oligospermia and considering this option, a formulation has been designed based on literature citation. Therefore, one of the good candidates could be a coded herbal formulation Spermox.
It has been previously reported that T. terrestris, W. somnifera have good results in oligospermia and male infertility for the improvement of sperm quantity and quality. So by taking the advantage, the coded herbal formulation Spermox contains a total of 5 ingredients in which A. adscendens, W. somnifera, A. racemosus, T. terrestris and M. pruriens for the treatment of semen abnormalities causing infertility in man.
In ordered to validate the results, the statistical analysis was performed by Chi square and Fisher’s exact test to find out the level of significance and to confirm the efficacy of the treatment drugs both in test and control group as Spermox and Fertilox, respectively.
Patient characteristics
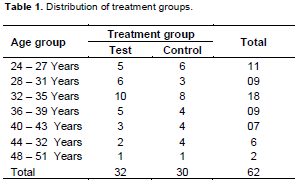
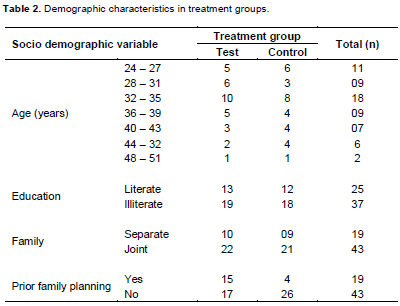
Total numbers of 32 patients were prescribed Spermox and Fertilox was prescribed to 30 patients as shown in Table 1. The age allocation of class interval was categorized as 24 to 50 years. The age distribution of 62 patients were recorded having 5 class intervals accordingly, 24 to 27, 28 to 31, 32 to 35, 36 to 39, 40 to 43, 44 to 32, and 48 to 51. It was observed from the data in Table 2 that infertility has a strong correlation with socioeconomic factors and this problem tends to worsened in illiterate population and the families were leading their life in stressful condition either due to joint family problems or other social factors.
Semen analysis
The normal range of semen quantity is 2 to 4 ml per ejaculation. The result depicted in Table 3 signifies no difference of treatment between two given medications as p value was calculated as 0.599 as shown in Table 3. The normal color of semen is grayish white to pale yellow and all patients of both groups were observed having normal color at base line and after treatment as well. Therefore, there was no change in semen color between test and control group. The range of sperm count is >20 millions/ml. It is a most common factor in oligospermic patients. After having the complete follow-up in test group out of 32 patients, 26 patients were recorded to be >20 millions/ml and only 6 patients were recorded to be <20 millions/ml. Whereas in the control group, out of 30 patients, 17 were recorded to be > 20 millions/ml and 13 patients were recorded to be <20 millions/ml. The Chi square test p value were calculated to be less than 0.05; it showed that there was a significant difference between these two drugs as shown in Table 3.
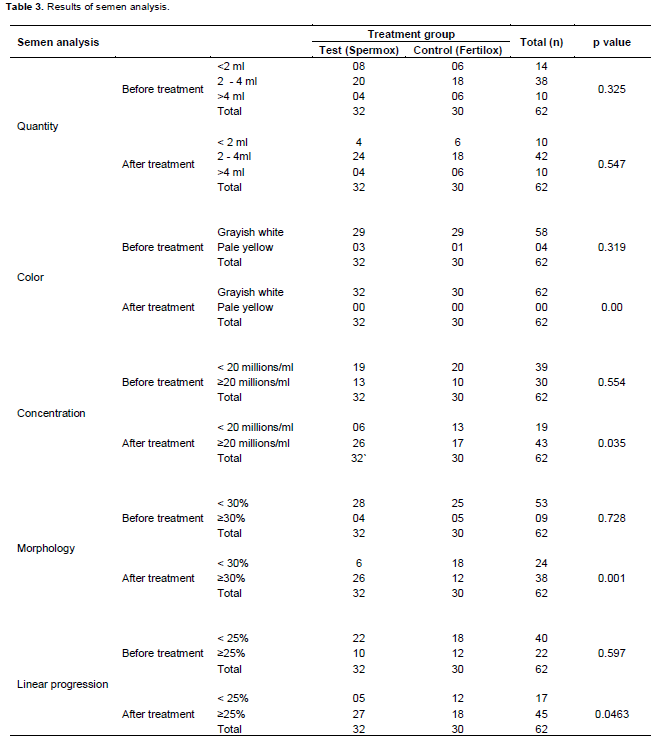
Similar results were seen in morphology and rapid linear progression of semen analysis where p values were 0.001 and 0.046. The range of normal morphology is >30%/ml. It is also a most common factor in oligospermic patients.
This study was under taken as clinical evaluation of effect of herbal medicine on quantity and quality and motility of sperm in oligospermia. An attempt has been made to explore the performance of herbal (test drug) and authentic allopathic (control) medicine so as to asses their efficacy.
All the patients enrolled in the study were valuable for safety. Side effects were defined as sign and symptoms that first occurred or became more severe during the course of treatment. Majority of adverse events were assessed as mild in severity and self-limiting in nature. Therefore, none of the patients withdrew from the study due to these adverse events. Side effects classified by the clinical exports were found to be drug related in patients administered Fertilox, such as nausea (5 patients), malaise (3 patients), headache (2 patients), and loss of appetite (4 patients), were the most observed drug related events among control recipients and no side effects were recorded in test treated recipients. No critical side effects recorded in any group, that is, hot flushes, psychological upset, hypertension, etc. It is because of the fact that plant drug selected for the treatment of male infertility does not contain any chemical agent that may trigger the adverse drug reaction response. This can be explained further that chemical components of the plant drugs altogether are low in the frequency of occurrence and even administered together in synergistic fashion exhibit pronounced type of effective response for curative action.
DISCUSSION
Generally, there are different causes of infertility such as lacks in discharge per ejaculate, sperm count (e.g., oligospermia, low sperm count, azoospermia, no sperm in the discharge), sperm motility, or sperm morphology. Therefore, with the diagnosis, one can always pinpoint the causes of infertility and on this basis treatment modalities can be planned. The beginning assessment of the male partner ought to be quick, noninvasive, and less expansive. A comparative approach will suffice to pick the treatment choices for the couple for the wanted result.
Medicinal plants were selected to form dosage designed to manufacture Spermox. The literature citation have been thoroughly searched that all these plants are utilized to combat infertility in male. Basically, Aspragus recemosu, M. pruriens, A. adscendens, W. somnifera, and T. terrestris, the first three plants directly act on sperm motility and increment of sperm counts and related factors, whereas Withnia sominfera is an immunity enhancer and Tribulus terresteris is spermogenic.
The semen investigation is the beginning stage in the assessment of male infertility and when discovered to be normal, endocrine anomalies are amazingly uncommon, and further hormonal assessment more often than not is superfluous. As a general manual for the conclusion of male subfertility, the WHO has given typical qualities for semen examination such as volume > 2 ml, density > 20 million/ml, motility > 50% forward progression, morphology > 30% normal forms, round cells > 5 million/ml, and white cells > 1 million/ml (WHO, 1992; Damani and Shaban, 2008).
On the treatment with Spemox, the normal range of semen quantity is 2 to 4 ml per ejaculation. The range of sperm count was found to be >20 millions/ml. In case of Spermox and test drugs of 32 patients, 26 patients were recorded >20 millions/ml, whereas in Fertilox control group, out of 30 patients, 17 were recorded >20 millions/ml affording p value less than 0.05. Similarly, of test and control drugs, results for morphology and rapid linear progression of semen analysis afforded p values of 0.001 and 0.046, and the range of normal morphology was determined as >30% per ml. All these parameters corroborate with the aforementioned semen results and clearly displayed that Spermox is comparatively superior than Fertilox in the management of idiopathic oligospermia. In addition, no side or untoward effects have been observed in case of Spermox and use of medicinal plants product have shown that oligospermia is possible with considerable success. A lot of studies have provided evidence that medicinal plants products may improve semen parameters, but again is not consistent and variation in the treatment may occur, therefore, better designed clinical trials is a need for the management of male infertility (Arcaniolo et al., 2014).
CONCLUSION
The finding from this study demonstrated the following salient clinical assessment; there was statistically significant difference when comparing the effectiveness of herbal treatment Spermox to Fertilox for the treatment of idiopathic oligospermia as described in the thesis. This is clearly evident that Spermox possesses a therapeutic value for the treatment of idiopathic oligospermia.
There was no untoward manifestation associated with the use of Spermox and this has found good acceptability by all treated patients. The principal objective on herbal medicine Spermox as compared to Fertilox is to determine whether these may represent a platform for the development of novel therapeutic. This is an exercise of applying modern techniques and clinical design to product that have been in use for centuries. The efficacy of herbal formulation is a characteristic of a complex mixture of chemical compounds present in different herbs used as multiple dosage form design.
The results from this research study have clearly revealed the evidence of efficacy of test drug Spermox as compared to Fertilox. This study outlines an approach to the scientific and clinical validation of traditional and conventional medicines, so in its ultimate dictate; this is a worthwhile exercise, since it leads to new class of therapeutics.
CONFLICT OF INTEREST
Authors have none to declare
REFERENCES
|
Arcaniolo D, Favilla V, Tiscione D, Pisano F, Bozzini G, Creta M, Gentile G, Menchini FF, Pavan N, Veneziano IA, Cai T (2014). Is there a place for nutritional supplements, in the treatment of idiopathic male infertility? Arch. Ital. Urol. Androl. 86(3):164-170. Crossref |
||||
|
Cavallini G (2006). Male idiopathic oligoasthenoteratozoospermia. Asian J. Androl. 8(2):143-157. Crossref |
||||
| Chittendon F (1956). RHS Dictionary of Plants plus Supplement. Comprehensive listing of species and how to grow them. Somewhat outdated, it has been replaces in 1992 by a new dictionary. | ||||
| Chopra RN, Nayar SL, Chopra LC (1996). Glossary of Indian medicinal plants. New Delhi: Council of Scientific and Industrial Research, 2002. | ||||
|
Damani MN, Master V, Meng MV, Burgess C, Turek P, Oates RD (2002). Postchemotherapy ejaculatory azoospermia: fatherhood with sperm from testis tissue with intracytoplasmic sperm injection. J. Clin. Oncol. 20(4):930-6. Crossref |
||||
| Dorland's Medical Dictionary for Health Consumers (2007). Dorland's Medical Dictionary: oligozoospermia. (n.d.). Available at: http://medical-dictionary.thefreedictionary.com/oligozoospermia | ||||
| Farone WA, Koenigsberg S (1995). US Patent 5,395,419, Treating with composition comprising metal peroxide intercalated with a source of simple phosphate ion. Google Patents. | ||||
|
Grimes DA, Lopez LM (2007). Oligozoospermia, azoospermia, and other semen-analysis terminology: the need for better science. Fertil. Steril. 88(6):1491-94. Crossref |
||||
| Hedrick UP (1919). Sturtevant's Edible Plants of the World, Dover Publications 1972 ISBN 0-486-20459-6. | ||||
|
Mayank T, Shilpi B, Dixit VK (2009). Effect of Asparagus racemosus on sexual dysfunction in hyperglycemic male rats. Pharm. Biol. 47(5):390-395. Crossref |
||||
|
Mutee AF, Salhimi SM, Ghazali FC, Aisha AF, Lim CP, Ibrahim K, Asmawi MZ (2012). Evaluation of anti-cancer activity of Acanthester planci extracts obtained by different methods of extraction. Pak. J. Pharm. Sci. 25(4):697-703. Pubmed |
||||
|
Panda S, Kar A (1998). Changes in thyroid hormone concentrations after administration of ashwagandha root extract to adult male mice. J. Pharm. Pharmacol. 50(9):1065-8. Crossref |
||||
|
Shukla KK, Mahdi AA, Ahmad MK, Shankhwar SN, Rajender S, Jaiswar SP (2009). Mucuna pruriens improves male fertility by its action on the hypothalamus-pituitary-gonadal axis. Fertil. Steril. 92(6):1934-40 Crossref |
||||
| WHO (2010) laboratory manual for the examination and processing of human semen. 5 edition. [Geneva]: World Health Organization. | ||||
| World Health Organization (1992). Laboratory Manual for the Examination of Human Semen and Sperm--Cervical Mucus Interaction. Cambridge, Cambridge University Press. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


