ABSTRACT
Pain is defined as any an unpleasant sensory and emotional experience associated with actual or potential tissue damage. Adequate postoperative pain management can reduce the patients‟ length of hospitalization and decrease postoperative complications. However, post-operative pain has not been satisfactorily relieved. Thus, the aim of this work is to assess professionals’ knowledge on post-operative pain management. Institutional based cross sectional study design was conducted. All health professionals who have worked in operation room, surgical ward, recovery room, and post anesthesia care unit were included. Data was entered into Epi info version 7 and transported to SPSS version 21 for analysis. Tables and narratives were used to determine descriptive statistics. A total of 52 participants were included in the study of which 59.6% were male. 69% of the respondents were found to be between the age of 20 and 23 years. Almost all patients in this study (94.23%) do not use pain assessment tools and 78.85% of the respondents do not know about multimodal analgesia. Approximately, one third of the respondents 32.69% mentioned that the drug is administered when the patient complain of pain. These showed that there is a knowledge gap on postoperative pain managements. Therefore, it was strongly recommended to improve professionals’ knowledge on postoperative pain management.
Key words: Pain, postoperative pain management, Asella Teaching Referral Hospital.
Abbreviation:
ATRH, Asella Teaching Referral Hospital; NRS, numeric rating scale; POP, postoperative pain; POPM, postoperative pain management; VRS, verbal rating scale; VAS, visual analogue scale.
Pain is a universal experience and it is the most frequent reason for people seeking health facility. Because perception and tolerance of pain vary widely from one person to another person, it is difficult to define and describe. Basically, pain is the way the brain defines information about specific feeling that the body is experiencing (Ojong et al., 2014). According to American Society of Anesthesiologists (Warfield and Kahn, 1995), postoperative pain is the type of acute pain that is present in a surgical patient because of a preexisting surgical procedure, or a combination of disease-related and procedure-related resources (Abdalrahim, 2009). Incidence of postoperative pain (POP) is found between 47 and 100%. Postoperative pain is classified as a serious public health problem both in the developed and in developing countries. In Africa, the issue of pain has been explored largely in relation to acquired immune deficiency syndrome (AIDS) and cancer, but pain from surgical procedures poses a far greater burden on the patient (Woldehaimanot et al., 2014).
Patient suffering from pain can develop an increase in the sympathetic response of the body with subsequent rises in heart rate, increase cardiac work, difficulty of breathing and inadequate oxygen consumption. In addition, prolonged postoperative pain can limit physical exercise and lead to venous stasis, an increased risk of deep vein thrombosis and consequently pulmonary embolism (Gallagher et al., 2004; American Society of Anesthesiologists Task Force on Acute Pain Management, 2004). Undertreated acute pain can progress to chronic pain which impairs an individual’s ability to carry out daily activities and diminish quality of life. Thus, undertreated pain has significant physical, psychological, and financial consequences; postoperative pain creates a healthcare challenge requiring knowledge in how to prescribe and administer drugs, assess and reassess pain, and a broad understanding of cultural and ethnic responses to pain and pain management (Grinstein-Cohen et al., 2009).The self-report of pain is the gold standard of pain assessment given the subjective nature of pain (Kizza, 2012).
The importance of postoperative pain management has been repeatedly demonstrated in the past two decades. Adequate postoperative pain management (POPM) can reduce the patients’ length of hospitalization and decrease postoperative complications (Suwanraj, 2010). However, research has consistently been demonstrated in pain management, pain which has not been satisfactorily relieved (Rejeh et al., 2008; Taylor et al., 2008), results to unnecessary suffering of a patient, increased complications and increased costs ((Rejeh et al., 2008; Windsor et al., 1996). Therefore, it is very important to assess knowledge level of health professional that helps to establish preventive strategies of postoperative pain in the local areas.
Study setting
This study employed a cross-sectional study design at Asella Teaching and Referral Hospital from 20 March, 2017 to 30 March, 2017. Asella Hospital is one of the government hospitals in Ethiopia in Asella town. Asella town is the administrative city of Arsi zone and is located at a distance of 175 km to the Eastern Addis Ababa, capital city of Ethiopia. The hospital has 9 wards. The hospital offers both graduate and undergraduate training including specialty like General Surgery and Gynecology.
Source population
All staff working in operating room, surgical ward, and post anesthesia care units in Asella Teaching and Referral Hospital.
Study population
Selected staff working in operating room, surgical ward, and post anesthesia care units in Asella Specialized Teaching Hospital from 20 May, 2017 to 30 May, 2017 were the study population.
Sample size determination and sampling technique
Census was used to include all selected staff working in operating room, surgical ward and post anesthesia care units in Asella Specialized Teaching HOSPITAL.
Data collection tools and procedure
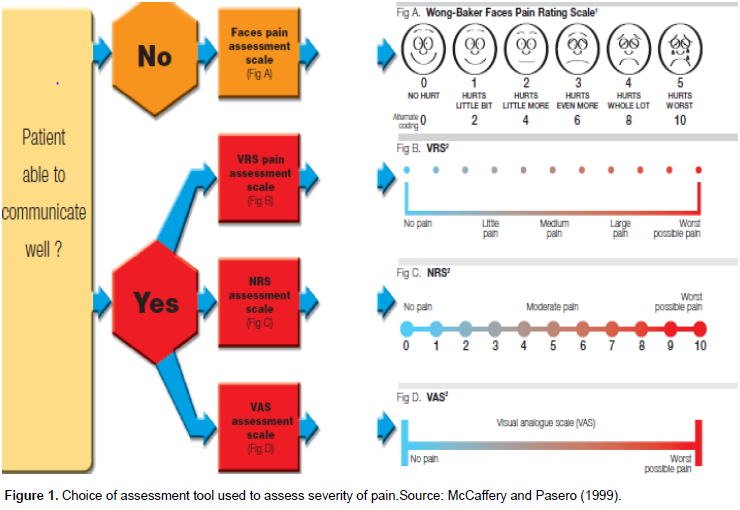
Data was collected using pretested structured questionnaires developed in English language. Two BSc anesthetists and one MSc holder anesthetist were involved as data collectors and supervisors, respectively. Patient’s charts were reviewed by data collectors. The respondents were assessed to determine whether they have used at least one of these assessment tools. Several pain scoring systems were available include Wong-Baker Faces Pain Rating Scale where the patients estimate impacts of pain as no hurts “as no pain” and worst hurt indicating “worst possible pain”; Verbal Rating Scale (VRS) where pain is rated as no pain, mild pain, moderate pain and severe pain; the Visual Analog Scale (VAS) where the individual scores the pain on a 10-cm line where the left anchor point is labeled “no pain” and the right anchor point is labeled “worst possible pain” or Numerical Rating Scale (NRS) where the patients estimate the pain as a number between 0 indicating “no pain” and 10 indicating “worst possible pain. The respondents were also assessed on whether pain intensity is recorded as frequently as once in 5 min during the initial phase when the initial dose of the drugs are being given in an incremental manner. Once adequate basal analgesia has been established, the frequency of assessment can be reduced to once every 2 h during the first 24 to 48 h and once every 4 h thereafter (Figure 1).
Data quality assurance, data analyzing and processing
Pretest was done on 5% of the sample population at Asella Teaching and Referral Hospital. Data collectors and supervisors were trained on each items included in the study tools. During data collection, regular supervision and follow up was made. Investigator cross checked for completeness and consistency of data on daily basis. The data was entered into epi info version 7 and was exported to SPSS version 21 computer program for analysis. Descriptive statistics was used to summarize data, tables and figures for display results.
Operational definition
Pain: Any unpleasant emotional experience that the patient has experienced. Postoperative pain: Pain that patient has experienced after surgery.
Pain management: Any attempt that is made to alleviate pain.
Multimodal analgesia: Administration of different drug with different route of administration.
Ethical consideration
Ethical clearance and approval was obtained from ethical review committee, Anesthesia Department, Arsi University. Permission to conduct was obtained from the hospital. Informed verbal consent was secured from every study participants. The obtained data was only used for study purpose. Confidentiality and anonymity were ensured.
Socio-demographics characteristics of respondents
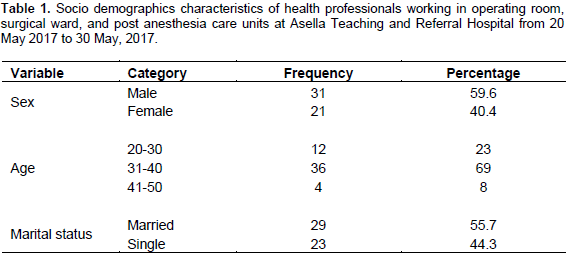
A total of 52 respondents were included into the study of which 59.6% were male. Majority of the respondents (69%) were between the age group of 20 and 23 years. The mean age of respondents was 32.27 ± SD (12.0298), minimum 20 and maximum 48 (Table 1).
Barriers to pain assessment
Barriers to pain assessment included lack of training on assessment tools (92.6%), lack of availability of assessment tools (88.3%), lack of familiarity with tools (84.7%), lack of protocols and guidelines on pain assessment and management (68.8%), and poor documentation of pain assessment (56.4%).
Knowledge about pain
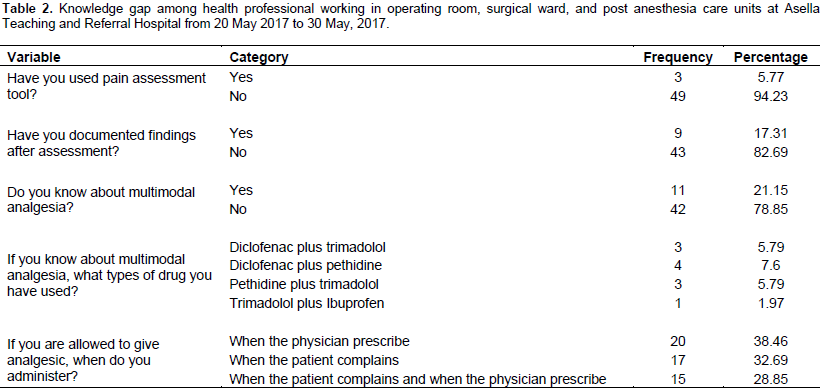
Majority (94.23%) of all respondents do not use pain assessment tools. Over four fifth (82.69%) of the participants have not documented findings after assessment. About 32.69% of respondents mentioned the patient as the most accurate ways of rating the pain intensity. The respondents were asked about what drugs should be given postoperatively, 78.85% of the respondents said that they do not know about multimodal analgesia. From these findings, it can be concluded that there is knowledge gap among health professional towards postoperative pain management (Table 2).
In this study, it was found that knowledge level of health professionals towards postoperative pain management was poor which is consistent with the study done to assess postoperative pain management and associated factors among nurses in five selected public hospitals in Addis Ababa (Hailemariam, 2015). In addition, the practice of postoperative pain management was lower than a study done in Bangladesh which showed that knowledge of health professionals towards postoperative pain management was good (Hossain et al., 2014). This may be due to difference in the type of professionals involved in the study as the study included all health professionals working in operating room, surgical ward, and post anesthesia care units of Asella Specialized Teaching Hospital.
The result of the present study also found that about 32.69% of respondents mentioned the patient as the most accurate ways of rating the pain intensity which was lower than the assessment of adult postoperative pain management practice among nurses working in Addis Ababa public hospitals (46.6%). This may be due to variation in resources available, professional knowledge and work experiences of health professional (Hailemariam, 2015). In this study, it was found out that pain rating records were not fully available in the hospital and the analgesics were prescribed when the physician orders or when the patient complains of pain. In Nigeria, pain assessment tools are available but with poor documentation (Kolawole and Fawole, 2003). However, the study done in Europe showed that there are very good documentation of assessed pain and written pain treatment guidelines and procedure existed (Ene et al., 2008; Rawal, 2016).
CONCLUSION AND RECOMMENDATIONS
Adequate postoperative pain management can reduce the patient’s length of hospitalization and decrease postoperative complications. However, in this study, it was found that there have been knowledge gap on post-operative pain managements as majorities of the respondents do not use pain assessment tools and multimodal analgesia. Therefore, providing a continuous education program on pain assessment, starting to use pain assessment tools, guidelines and protocols, and documenting assessment tools were recommended.
The authors have not declared any conflict of interests.
The authors would like to thank all respondents for their kind response during data collection. Then, they would like to thank all authors of the articles and on-line information for the valuable works read and cited in the paper.
REFERENCES
|
Abdalrahim MS (2009). Postoperative Pain Assessment and Management: The Effects of an Educational program on Jordanian nurses' practice, knowledge, and attitudes: Institute of Health and Care Sciences. Available at:
View
|
|
|
|
American Society of Anesthesiologists Task Force on Acute Pain Management (2004). Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 100(6):1573.
Crossref
|
|
|
|
|
Ene KW, Nordberg G, Bergh I, Johansson FG, Sjöström B (2008). Postoperative pain management–the influence of surgical ward nurses. J. Clin. Nurs. 17(15):2042-2050.
Crossref
|
|
|
|
|
Gallagher R, Hawley P, Yeomans W (2004). A survey of cancer pain management knowledge and attitudes of British Columbian physicians. Pain Res. Manag. 9(4):188-194.
Crossref
|
|
|
|
|
Grinstein-Cohen O, Sarid O, Attar D, Pilpel D, Elhayany A (2009). Improvements and difficulties in postoperative pain management. Orthopaedic Nurs. 28(5):232-239.
Crossref
|
|
|
|
|
Hailemariam E (2015). Assessment of postoperative pain management in Saint Paul's Hospital Millennium Medical College. Addis Ababa University Addis Ababa, Ethiopia. Available at:
View
|
|
|
|
|
Hossain S, Wiroonpanich W, Orapiriyakul R (2014). Nurses' knowledge and attitudes, and pain management practice of post-operative children in Bangladesh. Available at:
View
|
|
|
|
|
Kizza IB (2012). Nurses' Knowledge and Practices Related to Pain Assessment in Critically ill Patients at Mulago Hospital, Uganda. Muhimbili University of Health and Allied Sciences. Available at:
View
|
|
|
|
|
Kolawole I, Fawole A (2003). Postoperative pain management following caesarean section in University of Ilorin Teaching Hospital (UITH), Ilorin, Nigeria. West Afr. J. Med. 22(4):305-309.
|
|
|
|
|
McCaffery M, Pasero C (1999). Teaching patients to use a numerical pain-rating scale. AJN Am. J. Nurs. 99(12):22.
Crossref
|
|
|
|
|
Ojong IN, Ojong-Alasia MM, Nlumanze, FF (2014). Nurses' assessment and management of pain among surgical patients in secondary health facility in Calabar Metropolis, Cross River State, Nigeria. Eur. J. Exp. Biol. 4(1):315-320.
|
|
|
|
|
Rawal N (2016). Current issues in postoperative pain management. Eur. J. Anaesthesiol. 33(3):160-171.
Crossref
|
|
|
|
|
Rejeh N, Ahmadi F, Mohammadi E, Anoosheh M, Kazemnejad A (2008). Barriers to and facilitators of postâ€operative pain management in Iranian nursing: a qualitative research study. Int. Nurs. Rev. 55(4):468-475.
Crossref
|
|
|
|
|
Suwanraj M (2010). Current practice, perceived barriers, and perceived facilitators of Thai nurses on using the evidence-based practice on pain assessment and pain management in older adults: The University of Iowa. Available at:
View
|
|
|
|
|
Taylor AL, Gostin LO, Pagonis, KA (2008). Ensuring effective pain treatment: a national and global perspective. JAMA 299(1):89-91.
Crossref
|
|
|
|
|
Warfield C, Kahn C (1995). Acute Pain ManagementPrograms in US Hospitals and Experiences and Attitudes among US Adults. J. Am. Soc. Anesthesiol. 83(5):1090-1094.
Crossref
|
|
|
|
|
Windsor A, Glynn C, Mason D (1996). National provision of acute pain services. Anaesthesia 51(3):228-231.
Crossref
|
|
|
|
|
Woldehaimanot TE, Eshetie TC, Kerie, MW (2014). Postoperative pain management among surgically treated patients in an Ethiopian hospital. PloS one 9(7):e102835.
Crossref
|
|