Full Length Research Paper

ABSTRACT
Atherogenic dyslipidemia worsens cardiovascular functions and supporting data concerning dyslipidemia among hypertensive patients in Ethiopian situation is very limited. The objective of this study was to assess factors associated with atherogenic dyslipidemia among hypertensive patients at Southern Ethiopia. A cross-sectional study was conducted on 238 hypertensive participants at Hawassa University comprehensive specialized hospital from September 2015 to June 2016. Systematic random sampling technique was used and written informed consent was obtained from each participant. Socio-demographic and other relevant data were collected by pre-structured questionnaires. In addition overnight fasting blood sample was collected from each study subjects for serum biochemicals determination. About 90.8% of patients had least one dyslipidemia, with the most frequent being hypertriglyceridemia (62.2%) and low high-density lipoprotein cholesterol (HDL-c, 60.9%). Being a female was significantly associated with dyslipidemia. The adjusted odds ratio (95% CI) was 2.1 (1.2-3.9; P=0.01) for hypercholesterolemia (TC), 2.4 (1.1-4.9; P=0.02) for raised low-density cholesterol (LDL-c) and 2.9 (1.6-5.4; P<0.0001) for low HDL-c. In addition, patients with hyperuricemia were more likely to develop hypercholesterolemia, hypertriglyceridemia, low HDL-c and raised TC/HDL-c when compared to patients with normouricemia. The adjusted odds ratio (95% CI) was 1.8 (1.1-3.1; P=0.047), 2.6 (1.4-4.8; P= 0.001), 2.7 (1.5-4.8; P=0.001) and 3.1 (1.7-5.4, P<0.0001), respectively. The prevalence of raised TC, LDL-c, triglycerides and low HDL-c were higher in hypertensive patients and these are an established atherogenic lipid profiles. Therefore, lipid profiles should be performed at the baseline of hypertension diagnosis prior to starting any anti-hypertensive agents and then periodically through treatment follow-up to manage any increasing trends.
Key words: Atherogenic dyslipidemia, hypertension, cardiovascular risks, Southern-Ethiopia.
Abbreviation: AOR, adjusted odds ratio; BMI, body mass index; BP, blood pressure; CI, confidence interval; CVD, cardiovascular diseases; CHD, coronary heart disease; COR, crude odds ratio; HDL-c, high density lipoprotein-cholesterol; TC, total cholesterol; LDL-c, low density lipoprotein-cholesterol; HTN, hypertension; WHO, World Health Organization; TG, Triglycerides; SPSS, Statistical package for Social Sciences; NCEP-ATP, National Cholesterol Education Program-Adult Treatment Panel; MetS, metabolic syndrome.
INTRODUCTION
Hypertension (HTN) is a disease that is characterized by raised blood pressure; and HTN is one of the main indicators of the cluster of clinical anomalies that characterize metabolic syndrome (MetS). About 30 to 40% of the hypertensive subjects develop MetS (Marchi-Alves et al., 2012). Dyslipidemia is the one, which causes atherosclerosis, and the atherosclerosis is linked with pathophysiologic as well as structural alteration in arteries, and it contributes to the progress of arterial hypertension and other risks (Oparil et al., 2003). In addition, atherogenic dyslipidemia consists of raised blood triglycerides (TGs) and apolipoprotein B (apoB), raised level of small low-density lipoprotein cholesterol (LDL-c) particles, and a reduced level of high-density lipoprotein cholesterol (HDL-c) (NCEP III, 2002). Besides, it is well known that cardiovascular disease (CVD) is associated with HTN and altered level of blood lipids (increased levels of LDL-c, total cholesterol (TC), and TGs) and low level of HDL-c (NCEP III, 2002; Jacobson et al., 2014; Mora et al., 2013). The frequent bunching of hypertension with atherosclerotic dyslipidemia, and other metabolic derangements in patients has been obviously proven to be synergistic and accelerating the development of atherosclerosis and CVD related morbidity and mortality (NCEP III, 2002). Moreover, several studies suggested that serum LDL-c, TGs, TC, apolipoprotein-B levels, TG/HDL-c, were strongly associated with serum hyperuricemia, while the HDL-c level was significantly and inversely associated with hyperuricemia (Peng et al., 2015, Lu et al., 2012, and Conen et al., 2004). This signifies that serum uric acid is a strong risk factor of coronary heart diseases (CHD) (Choi and Ford, 2007). Besides, older age and female gender was also risk factors of dyslipidemia except for low HDL-c (Yu et al., 2015).
Furthermore, urbanization, increased life expectancy, the effect of non-healthy diet and individuals’ lifestyle have a great impact on rising trend of CVD in developing as well as developed countries (Joshi et al., 2007). Nowadays, the increasing incidence of hypertension situation and atherogenic dyslipidemia in patients may worsen the health condition and predisposes to other non-communicable diseases. In addition, CVD related illnesses and diabetes are 21st century great temptations in most developing countries. However, data concerning dyslipidemia among hypertensive patients in Africa situation including Ethiopia is limited. Therefore, the present study aimed to assess factors associated with atherogenic dyslipidemia among hypertensive populations.
MATERIALS AND METHOD
Study setting and study population
This institution based cross sectional study was conducted at Hawassa University comprehensive specialized Hospital, Southern Nations Nationalities and Peoples Region (SNNPR) from September 2015 to June 2016. The Hospital was established in November 2006 and it provides teaching and health services for more than 15 million people of the south region and neighboring regions. Currently, the hospital has over 400 beds and gives different health services including students’ practical training. All hypertensive subjects age greater than or equal to18 years old who had a regular follow-up were eligible in the study. However, patients using lipid-altering drugs, pregnant women, and patients with confirmed diabetes, cardiac and renal failure were excluded from the study.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences. All the study subjects were well informed about the procedures of the study, the involvement was voluntary and written informed consent was obtained from each study participant prior to data collection.
Sample size and technique
The sample size was calculated based on single population proportion formula and the prevalence of 17.8% of combined dyslipidemia in hypertensive patients (Akintunde et al., 2010).
Based on the above-mentioned, formula, including with 10% non-response rate, the final sample size was calculated to be 248. To select participants from the study population, direct patients flow was checked for one week in the chronic diseases clinic including with patients’ logbook assessment. Thus, the trend showed that the average weekly hypertensive patients flow was about 80. Lastly, every fourth hypertensive patients were selected using systematic random sampling approach.
Data collection and measurements
Socio-demographic data and other important clinical information of the study participants were collected by trained nurses using pre-tested structured questionnaires. Hydrodynamic data (Systolic blood pressure and diastolic blood pressure) was measured from each subjects using automatic electronic sphygmomanometer (Omron). The accuracy of the measurment was sustained by measuring a minimum of two readings within 3-5 min differences after patients rested about 10-15 min in the clinic and finally the average blood pressure (BP) was taken and recorded Regarding anthropometric data, weight, height and waist circumference were measured based on WHO steps. By using weight and height, body mass index (BMI) was calculated for each individual as the weight (Kg) divided by the height square (m2) and classified based on international conventions (WHO, 2016). In addition, waist circumference (WC) of the individuals was measured at the navel using a non-stretched tape (to the nearest 0.1 cm) with standing position.
Overnight fasting 4-5 ml of venous blood sample was collected from each study subjects and then serum was obtained and analyzed for determination of lipid profile and uric acid using A25TM BioSystem Random Access chemistry analyzer in the Hawassa University Comprehensive specialized hospital laboratory. While, TC/HDL-c ratio was calculated from TC and HDL-c.
Definition of dyslipidemia
According to National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP-III,) Guideline, individuals should have at least one of the following lipid parameters abnormal to be categorized under the presence of dyslipidemia: TC ≥200 mg/dl, HDL-c (<40 mg/dl in men and <50mg/dl in women), LDL-c ≥ 130 mg/dl, TG ≥150mg/dl and TC/HDL-c ratio ≥5 (NCEP III, 2002) whereas hyperuricemia was assessed based on uric acid levels ≥7.2 mg/dl in males and ≥6.0 mg/dl in females (Sui et al., 2008).
Statistical analysis
All questionnaires were checked and entered into epidata version 3.1 Statistical Package for Social Sciences (SPSS version 20) was used for statistical analysis. Categorical variables were summarized as frequencies and percentages, while mean values and standard deviations were tabulated for normally distributed quantitative continuous variables. In addition, median values and interquartile range (IQR) were tabulated for skewed variables. Chi-square was used for categorical variables. Furthermore, bivariate and multivariate binary logistic regression analysis was used to evaluate study groups variations in the distribution of categorical variables. Finally, in all cases, alpha level was set at 0.05 at 95% confidence interval (CI) for statistical significance.
RESULTS
Socio-demographic and other features of the study participants
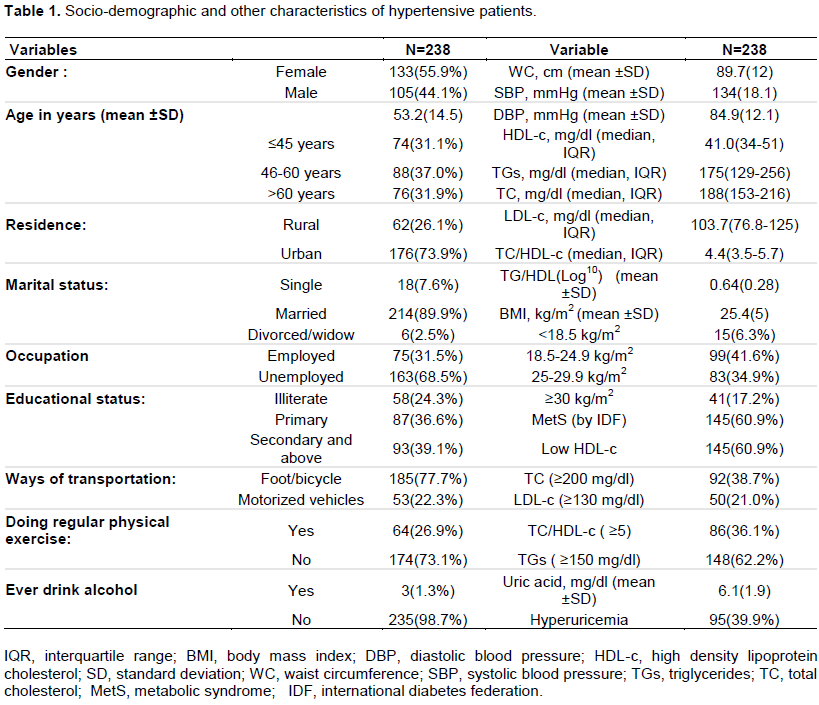
From 248 study subjects, about 238 participated in this study with 96% (238/248) response rate. Of whom, 44.1% (105/238) were men and 55.9% (133/238) were women with a mean age of 53.2 (±14.5) years. Majority, 226 (95%) of the patients had been using at least one anti-hypertensive agents. About 26.1, 7.6, and 24.4% of the study participants were rural residents, non-married and educationally unable to read and write, respectively. In addition, 17.2% of the study participants had BMI ≥ 30 Kg/m2 (obese). The prevalence of lipid derangements (TC ≥ 200 mg/dl, TGs ≥150 mg/dl, LDL-c ≥ 130 mg/dl and low HDL-c) was 38.7, 62.2, 21 and 60.9%, respectively. Further, 73.1% of the participants had no trends of doing regular physical exercises and 39.9% of the study subjects had hyperuricemia (Table 1).
Pattern of dyslipidemia in relation to different variables
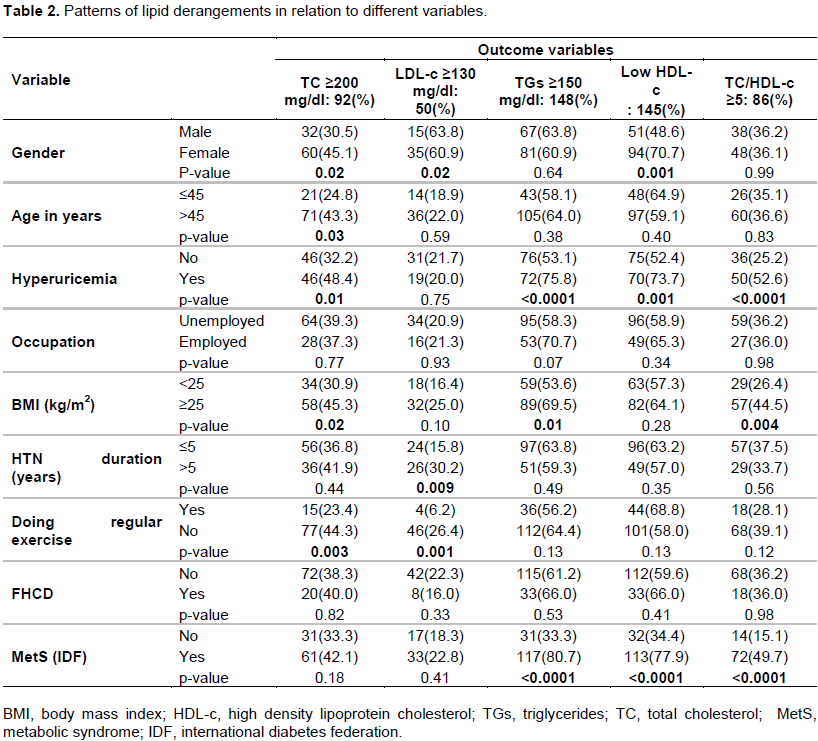
The prevalence of low HDL-c and TC ≥ 200 mg/ dl were significantly higher in females when compared to males, (45.1% vs. 30.5%, P=0.02) and low HDL-c (70.7% vs. 48.6%, P=0.001), respectively. The raised TC was significantly higher among patients older than >45 years when compared to ≤45 years (43.3% vs. 24.8 %; p=0.03), respectively. As well, raised TC, TGs and TC/HDL-c were significantly higher among patients with BMI ≥ 25 Kg/m2 (overweight to obese) when compared to patients with BMI<25 Kg/m2 (45.3% vs. 30.9%, p=0.02; 67.7% vs. 53.1%, p=0.01 and 44.5% vs. 26.4%, P=0.004), respectively. Moreover, patients who have no current history of performing of regular exercise had significantly raised TC and raised LDL-c (44.3% vs. 23.4%, P=0.003; and 26.4%vs. 6.2%, P= 0.001) when compared to those patients having experiences of performing regular physical exercise. Furthermore, the prevalence of hyperuricemia was 95 (39.9%) and abnormal levels of TC, TGs, HDL-c and TC/HDL-c were higher among patients with hyperuricemia (Table 2). About 90.8% of the study population had at least one lipid profile abnormal that is compatible with the diagnosis of dyslipidemia and 61.8% of the study participants had greater than or equal to two lipid profiles abnormal (dyslipidemia) (Figure 1).
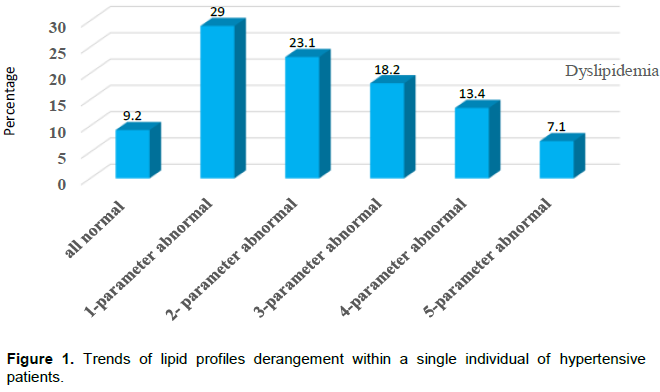
Patients with a single profile derangement: reduced HDL-c was 37 (15.5%), two-profile derangement: raised TG-HDL-c was 23 (11.8%), three-profile derangement: raised TG-HDL-TC/HDL was 28 (11.8%) and four profile derangement: raised TC-TG-HDL-TC/HDL-c was 16 (6.7%).
Factors associated with lipid derangements
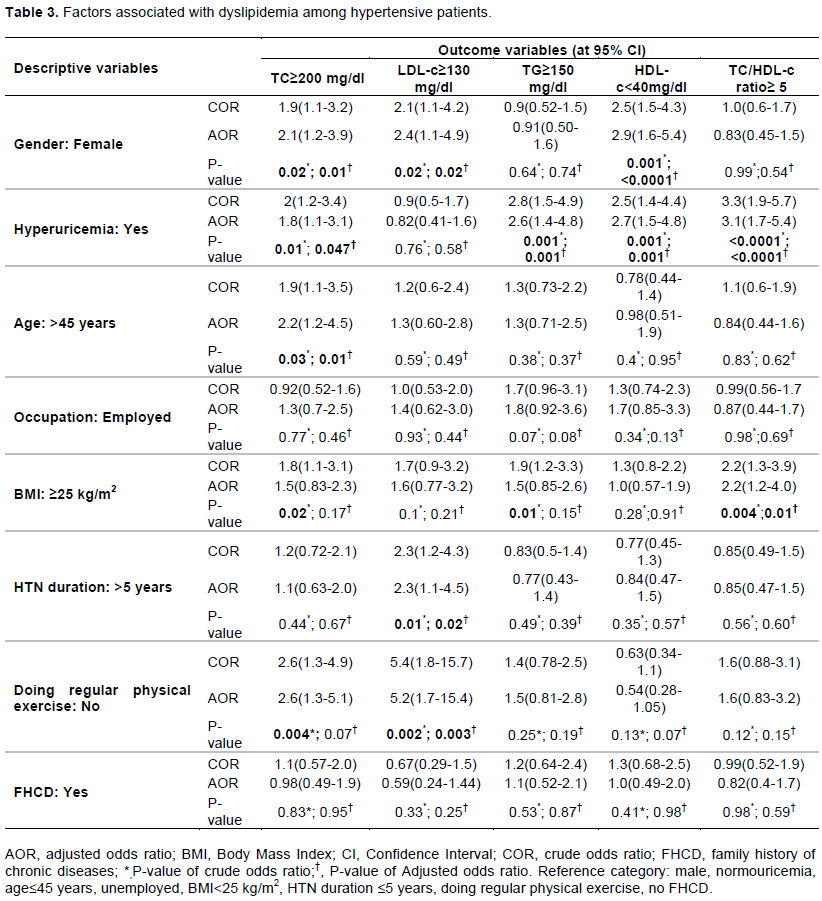
Bivariate analysis, model was applied to assess the independent risk factors for each lipid profile derangements. Being a female, the crude odds ratio [COR (95% CI): 1.9(1.1-3.2), P=0.02 for TC; 2.1(1.1-4.2), P=0.02 for LDL-c and 2.5(1.5-4.3), p=0.001 for HDL-c]. Hyperuricemia [COR (95% CI): 2.0(1.2-3.4, P=0.001) for TC: 2.8(1.5-4.9, P=0.001) for TGs; 2.5(1.4-4.4, P=0.001) for HDL-c; and 3.3(1.9-5.7, P<0.0001) for TC/HDL-c]. In addition, BMI and physical activity were significantly associated with TC, while the duration of HTN since its diagnosis and physical activity were significantly associated with LDL-c. However, multivariate analysis, was adjusted for independent factors and being a female, the adjusted odds ratio [AOR (95% CI): 2.1(1.2 3.9), P=0.01 for TC; 2.4(1.1-4.9), P=0.02 for LDL-c; and 2.9(1.6-5.4), P<0.0001 for HDL-c]. Hyperuricemia [AOR (95% CI): 1.8(1.1-3.1), P=0.047; for TC; 2.6(1.4-4.8), P=0.001 for HDL-c; and 3.1(1.7-5.4), P<0.0001 for TC/HDL-c].
In addition, experiences of performing physical exercise and the duration of HTN were significantly associated with LDL-c (Table 3).
DISCUSSION
We found that the prevalence of raised TC and low HDL-c were significantly higher in women when compared to men, and thus indicating the influence of gender in lipid derangement. In addition, we found that the prevalence of dyslipidemia (TC ≥ 200 mg/dl, TGs ≥150 mg/dl, LDL-c ≥130 mg/d l and low HDL-c) was 38.7, 62.2, 21 and 60.9%, respectively. Besides, the majority of hypertensive patients (90.8%) had at least one dyslipidemia and the mixed type of dyslipidemia (greater than or equal to two lipid profile derangements) was 61.8%. Moreover, female gender was associated with raised levels of TC, LDL-c and reduced HDL-c, while hyperuricemia was associated with abnormal level of TC, TGs, HDL-c and TC/HDL-c. Studies reported that the prevalence of dyslipidemia was 52.7% and 68.7% (Luo et al., 2014; Yu et al., 2015), respectively. In addition, Framingham Heart Study indicated that more than 80% of hypertensive patients had at least one additional cardiovascular disease risk factor and mainly these risk factors were atherogenic in nature. Also, frequently co-existence of hypertension and altered lipids cause a dyslipidemic hypertension (Kannel et al., 2000). This indicates the described lipid derangements (TC, LDL-c, HDL-c and TG) are atherogenic (NCEP 2002; Sudano et al., 2006), and suggest a possible risk for the increasing of cardiovascular diseases in a significant proportion among hypertensive patients in the near future.
In the present study, majority of hypertensive patients (90.8%) had at least one laboratory abnormality that is compatible with the diagnosis of dyslipidemia. Similarly, Pramiladevi et al. (2011) reported that the incidence of the overall forms of dyslipidemia was 90%. However, other two studies reported that low rate of dyslipidemia, was 50.8% (Osuji et al., 2012) and 41.2% (Iloh et al., 2012). Moreover, the altered levels of serum cholesterols are known to increase the risk of developing macrovascular complications such as coronary heart disease (CHD) and stroke (Albucher et al., 2000; Rader, 2002).
Our study indicated that the prevalence of raised TC was 38.7%. The finding is comparable with the rate reported by Osuji et al. (2012), which was 35.6%.
However, low prevalence was reported from a resource poor West-African setting (Iloh et al., 2012) and the rate in this study was 17.2%. The possible explanations for the variation could be genetic disparities between populations, ethnicity, and lifestyle, duration of hypertension and experiences of antihypertensive agents. Based on HDL-c cut off value, we found that the prevalence of reduced HDL-c was 60.9%. However, the low rate was reported from Nigeria (Osuji et al., 2012), and India (Akintunde et al., 2010), which was 21.6% and 47.9%, respectively. The differences may be attributed to the reality that only newly identified hypertensive participants were included in these two studies. The prevalence of raised LDL-c in our study was 21%. This rate is lower than the studies reported by Iloh et al. (2012) and Unniachan et al. (2014). The prevalence rate in these two studies was 23.8% and 86.2%, respectively. However, these studies used the cutoff >100 mg/dl; and this cutoff is lower than that of NCEP criteria (≥130) as used in our study.
The prevalence of raised TG in the present study was 62.2%. This is not in line with the prevalence reports of two Nigerian studies of (Osuji et al., 2012; Iloh et al., 2012) and North-west Ethiopia (Tachebele et al., 2014). The prevalence rate in these three studies was 6.4%, 14.8%, and 27.3%, respectively. However, there are suggestions that evidenced the magnitude of lipid derangements could show variation with the duration of treatment, across populations and settings.
We found that the prevalence of raised TC/HDL-c was 36.1%. This rate is lower and not in line with the prevalence reported by Pramiladevi et al. (2011), which was 50%. In addition, the variation possibly could be the small number of the study participants and the TC/HDL-c cutoff (>4.5) was used in this study; and the cutoff is lower than that of NCEP (≥5), as used in our study. Further, the increasing pattern of TC and decrement in HDL-c level in relation to age in both sex may have an impact to increase TC/HDL-c ratio.
According to O’Meara et al (2004) report, the prevalence of dyslipidemia was significantly higher among men when compared to women in both black and whites ethic groups. Conversely, our study indicated that female sex was significantly associated with dyslipidemia and this in line with the other report of studies (Yu et al., 2015; Choudhury et al., 2014). Furthermore, menopause age in women predisposes them to develop dyslipidemia as well as MetS, because HDL-c (good lipid) starts to decline following menopause and this consequences other lipid profiles derangement.
Several studies reported that BMI has a positive correlation with dyslipidemia (Iloh et al., 2012), and it is an independent risk factor of dyslipidemia (Yu et al., 2015); however, except TC/HDL-c our study indicates no association in between BMI and dyslipidemia after adjusting for confounding factors.
Hyperuricemia is significantly associated with raised TC, TGs, TC/HDL-c and low HDL-c in the current study. Similarly, studies reported that hyperuricemia was a significant predictor of dyslipidemia (Vekic et al., 2009; Peg et al., 2014). Besides, one study revealed that a significant correlation of uric acid with all components of MetS, as well as other risk factors in hypertensive patients (Papavasileiou et al., 2016). Furthermore, these depicted abnormal lipids highlight the complex interaction between serum uric acid and lipids, and this might have an impact on CVDs.
Furthermore, this study showed that physical activity was significantly associated with dyslipidemia. In consistent, several studies pointed out that the relation of increased physical activity with improved (lowered) the rate of cardiovascular risks, including with arterial blood pressure levels (Carnethon et al., 2003 and Hambrecht et al., 2000). However, one study forwarded that an acute physical exercise encourages the oxidative stress in untreated and mild hypertensive patients who have raised atherogenic lipids (Čaparević et al., 2009). In addition, the study highlights the requirement of pharmacological correction for those patients with atherogenic lipid profiles in order to prevent high peroxidation of lipids through severe exercise (Čaparević et al., 2009).
Limitation of the study
The study design was a cross-sectional that only approximates a single point in time. In addition, our study included only hypertensive patients and no control group, and this made the study not comprehensive. Regardless of these limitations, the study eventually increases evidence to the limited data situations.
CONCLUSION
Our study showed a high prevalence of dyslipidemia in hypertensive patients. Some of the non-modifiable risk factors like age, gender, and duration of hypertension were associated with dyslipidemia. In addition, some of the modifiable risk factors like BMI and experiences of physical exercise were significant with lipid derangements. This may indicate that a significant proportion of hypertensive patients are at risk of developing atherosclerosis and CVDs related morbidity and mortality.
Therefore, lipid profiles should be performed at baseline prior to receiving any anti-hypertensive agents and then periodically through treatment follow-up to manage any increasing trends.
In addition, National level of polices are required regarding awareness creation, life style modification and physical exercises. Furthermore, controlled cohort studies are also required to assess other risk factors of atherogenic dyslipidemia as well as cardiovascular risks including genetic variation.
CONFLICT OF INTERESTS
The authors declare that they have no conflict of interests.
ACKNOWLEDGEMENTS
We want to appreciate nurses for their endless support throughout data collection. In addition, we would like to acknowledge the Hawassa University for financial provision and hypertensive patients for their voluntary participation.
REFERENCES
|
Akintunde AA, Ayodele E, Akinwusi OP, Opadijo GO (2010). Dyslipidemia Among Newly Diagnosed Hypertensives: Pattern and Clinical Correlates. Journal of the National Medical Association 102:403-407. Crossref |
||||
|
Albucher JF, Ferrieres J, Ruidavets JB, Guiraud-Chaumeil B, Perret BP, Chollet F (2000). Serum lipids in young patients with ischaemic stroke: a case-control study. Journal of Neurology, Neurosurgery and Psychiatry 69(1):29-33. Crossref |
||||
| ÄŒaparević Z, Kostić N, Ćelić V, Ćosić Z, Marina Ä, Ilić S, PenÄić B (2009). Effects of acute exercise on atherogenic lipids in untreated mild hypertensive patients. Vojnosanitetski pregled 66(4):313-318. | ||||
|
Carnethon MR, Gidding SS, Nehgme R, Sidney S, Jacobs DR Jr, Liu K (2003). Cardiorespiratory fitness in young adulthood and the development of cardiovascular disease risk factors. JAMA 290(23):3092-3100. Crossref |
||||
|
Choi HK, Ford ES (2007). Prevalence of the metabolic syndrome in individuals with hyperuricemia. The American Journal of Medicine 120(5):442-447. Crossref |
||||
| Choudhury KN, Mainuddin AKM, Wahidzzaman M, Islam SMS (2014). Serum lipid profile and its association with hypertension in Bangladesh. Vascular Health and Risk Management 10:327-332. | ||||
|
Conen D, Wietlisbach V, Bovet P, Shamlaye C, Riesen W, Paccaud F, Burnier M (2004). Prevalence of hyperuricemia and relation of serum uric acid with cardiovascular risk factors in a developing country. BMC Public Health 4(1):1-9. Crossref |
||||
|
Hambrecht R, Wolf A, Gielen S, Linke A, Hofer J, Erbs S, Schoene N, Schuler G (2000). Effect of exercise on coronary endothelial function in patients with coronary artery disease. New England Journal of Medicine 342(7):454-460. Crossref |
||||
|
Iloh GP, Amadi AN, Njoku PU, Ofoedu JN, Awa-Madu J (2012). The magnitude of abdominal adiposity and atherogenic dyslipidemia among geriatric Nigerians with arterial hypertension in a rural hospital in South eastern Nigeria. Nigerian Journal of Clinical Practice 15:462-468. Crossref |
||||
|
Jacobson TA, Ito MK, Maki KC, Orringer CE, Bays HE, Jones PH, McKenney JM, Grundy SM, Gill EA, Wild RA, Wilson DP (2014). National Lipid Association recommendations for patient-centered management of dyslipidemia: part 1 - executive summary. Journal of clinical lipidology 8:473-488. Crossref |
||||
|
Joshi P, Islam S, Pais P, Reddy S, Dorairaj P, Kazmi K, Pandey MR, Haque S, Mendis S, Rangarajan S, Yusuf S (2007). Risk factors for early myocardial infarc¬tion in South Asians compared with individuals in other countries. JAMA 297(3):286-294. Crossref |
||||
|
Kannel WB (2000). Fifty years of Framingham study contributions to understanding hypertension. Journal of human hypertension 14:83-90. Crossref |
||||
|
Lu W, Song K, Wang Y, Zhang Q, Li W, Jiao H, Wang G, Huang G (2012). Relationship between serum uric acid and metabolic syndrome: an analysis by structural equation modeling. Journal of Clinical Lipidology 6(2):159-167. Crossref |
||||
|
Luo JY, Ma YT, Yu ZX, Yang YN, Xie X, Ma X, Liu F, Li XM, Chen BD (2014). Prevalence, awareness, treatment and control of dyslipidemia among adults in northwestern China: the cardiovascular risk survey. Lipids in Health and Disease 13:4. Crossref |
||||
|
Marchi-Alves LM, Rigotti AR, Nogueira MS, Cesarino CB, Godoy SD (2012). Metabolic syndrome components in arterial hypertension. Revista da Escola de Enfermagem da USP 46:1349-1354. Crossref |
||||
|
Mora S, Glynn RJ, Ridker PM (2013). High-density lipoprotein cholesterol, size, particle number, and residual vascular risk after potent statin therapy. Circulation 128(11):1189-97. Crossref |
||||
| National Cholesterol Education Program (NCEP) (2002). The third report of the National cholesterol education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation 106:3143-421. | ||||
|
O'meara JG, Kardia SL, Armon JJ, Brown CA, Boerwinkle E, Turner ST (2004). Ethnic and sex differences in the prevalence, Treatment, and control of dyslipidemia among Hypertensive adults in the genoa study. Archives of Internal Medicine 164:1313-1318. Crossref |
||||
|
Oparil S, Zaman MA, Calhoun DA (2003). Pathogenesis of hypertension. Annals of Internal Medicine 139(9):761-776. Crossref |
||||
|
Osuji CU, Omejua EG (2012). Prevalence and characteristics of the metabolic syndrome among newly diagnosed hypertensive patients. Indian Indian Journal of Endocrinology and Metabolism 16(Suppl1):S104. Crossref |
||||
|
Papavasileiou MV, Karamanou AG, Kalogeropoulos P, Moustakas G, Patsianis S, Pittaras A (2016). Uric acid blood levels and relationship with the components of metabolic syndrome in hypertensive patients. Journal of Human Hypertension 30:414-417. Crossref |
||||
|
Peng TC, Wang CC, Kao TW, Chan JY, Yang YH, Chang YW, Chen WL (2015). Relationship between Hyperuricemia and Lipid Profiles in US Adults. BioMed Research International, 2015:127596. Crossref |
||||
| Pramiladevi R, Gooranavar SM, Biradar SB, Baragundi MC, Kora SA, Narayan M (2011). Study of lipid profile in Hypertensive patients in rural Karnataka. Journal of Pharmaceutical and Biomedical Sciences 7(18):1-6. | ||||
|
Rader DJ (2002). High-density lipoproteins and atherosclerosis. American Journal of Cardiology 90(8):62-70 Crossref |
||||
|
Sudano I, Spieker LE, Noll G, Corti R, Weber R, Lüscher TF (2006). Cardiovascular disease in HIV infection. American Heart Journal 151(6):1147-1155. Crossref |
||||
|
Sui X, Church TS, Meriwether RA, Lobelo F, Blair SN (2008). Uric acid and the development of metabolic syndrome in women and men. Metabolism-Clinical and Experimental 57(6):845-852. Crossref |
||||
|
Tachebele B, Abebe M, Addis Z, Mesfin N (2014). Metabolic syndrome among hypertensivepatients at University of Gondar Hospital, North West Ethiopia. BMC Cardiovascular Disorders 14(1):177. Crossref |
||||
|
Unniachan S, Bash LD, Khovidhunkit W, Sri T, Vicaldo E, Ambegaonkar M (2014). Prevalence of lipid abnormalities and attainment of normal lipid levels among patients with dyslipidaemia: a pooled analysis of observational studies from five Asian countries. International Journal of Clinical Practice 68(8):1010-1019. Crossref |
||||
|
Vekic J, Jelic-Ivanovic Z, Spasojevic-Kalimanovska V, Memon L, Zeljkovic A, Bogavac-Stanojevic N, Spasic S (2009). High serum uric acid and low-grade inflammation are associated with smaller LDL and HDL particles. Atherosclerosis 203(1):236-242. Crossref |
||||
|
World Health Organization (WHO) (2016). Chronic diseases and health promotion: Stepwise approach to surveillance (STEPS). |
||||
|
Yu S, Guo X, Yang H, Zheng L, Sun Y (2015). Metabolic syndrome in hypertensive adults from rural Northeast China: an update. BMC Public Health 15:247. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


