Full Length Research Paper

ABSTRACT
Spinal anesthesia is one of the routinely anesthetic procedures done in practice. Post spinal backache is one of the complications causing discomfort in patients, leading to rejection of its use for next operations. The aim of this work is to assess the prevalence and factors associated with backache after spinal anesthesia from October to January at Asella Teaching and Referral Hospital, Asella, Ethiopia, 2016. Institutional based cross-sectional study design was conducted. All patients who underwent spinal anesthesia at Asella Teaching and Referral Hospital were included. They were selected by systematic random sampling technique. Data were collected by two BSC anesthetists and supervised by one MSC anesthetist. Data were entered into SPSS version 20 program for analysis. Odd ratio and 95% confidence interval were computed. Multivariate logistic analysis was used to identify factors associated with post spinal backache. A total of 318 participants were included in our study. Findings from post-operative 1st, 2nd, 3rd days and 4th week showed 38.0, 29.9, 16.0 and 31.6% of the patients suffered backache respectively. Common factors associated with post spinal backache from multivariate logistic regression at postoperative 1st, 2nd, 3rd days and 4th week were history of previous backache and spinal anesthesia. Factors associated with post spinal backache from multivariate logistic regression at postoperative 4th week were needle size, 18 and 21 gauge needle size (AOR = 3.686, 95% CI: 0.398, 34.183 and AOR = 2.410, 95% CI: 0.430, 13.503). Our study confirmed that prevalence of post spinal backache at post-operative 1st , 2nd, 3rd days and 4th week data showed 38.0 ,29.9,16.0 and 31.6% of the patients respectively. We recommend use of lesser and less traumatic spinal needles, infiltration of injection site with local anesthetic and firm postoperative pain management.
Key words: Spinal anesthesia, postspinal back pain, risk factors.
INTRODUCTION
Back pain is a very common health problem worldwide and affects up to 84% of the world population in a lifetime with having a great effect on health care price (Hoy et al., 2010). Post spinal back ache happens in nearly 13% of those getting spinal anesthetic (Rhee et al., 2010).
Spinal anesthesia is one of regional anesthesia attained by injecting small volume of local anesthetic to subarachnoid space through spinal puncture. It is simple to perform, reliable, safe, prevents depressant effects of anesthetic agents and produces comprehensive analgesia (Campbell and Sultan, 2009).
Even if spinal anesthesia is frequently used in outpatients and many routine surgeries, it has problems during or after the procedure starting from patient discomfort and prolonged hospital admissions to life threating condition. Among the complications, post spinal backache is one of the communal complications causing dissatisfaction in patients and leading to refusal for future surgeries (Rhee et al., 2010).
Backache after spinal anesthesia usually occurs during the first two to six hours after the procedure, as the local anesthetists use wear off. For most people, back pain from a spinal block lasts only a few days. Rarely, pain may continue for some weeks and pain becomes permanent because of nerve injury during needle placement (Schwabe and Hopf, 2001; Brooks et al., 2002).
Back pain following surgical procedures may result from many causes. In rare situation it may be an indicator of threatening complications such as epidural abscess or hematoma after lumbar or epidural block (Cook et al., 2009).
The aim of the study was to identify prevalence and risk factors of post spinal backache, to provide a baseline data and preventive methods of backache after surgical procedures.
MATERIALS AND METHODS
Study design
Cross sectional study design was employed.
Study area and period
The study was conducted at Asella Teaching and Referral Hospital located in Arsi Zone, Asella. The hospital is found at a distance of 175 km to Southeast of Addis Ababa, the capital city of Ethiopia. ATRH gives services to more than 2.5 million populations around the area. It is one of the fourth government hospitals found in Arsi Zone. The hospital gives services for community and teaching purpose. Presently, it provides inpatient, outpatient and emergency services. The hospital delivers gynecologic, obstetric, surgical, reproductive health and other services. It has four operation rooms and average number of surgical procedures done under spinal anesthesia at the hospital is six per day. The study was conducted from November to January 2016.
Source population
Source population was all patients undergoing surgical procedures under spinal anesthesia at Asella Teaching and Referral Hospital, Asella, Ethiopia, 2016.
Study population
Selected patients who underwent surgical procedures under spinal anesthesia from November to January at Asella Teaching and Referral Hospital, Asella, Ethiopia, 2016 were the study population.
Exclusion
Exclusion criteria involve patients under 16 years of age and patients who took analgesics within 12 h prior to surgery.
Sample size and sampling procedures
Sample size determination
The sample size is calculated using the single population proportion formula,
Formula components were:
n= number of sample size; Z= desired 95% confidence; Z=1.96; p = percentage of incidence of back pain; q =1-p; for this study, we presumed maximum variability, hence p = 0.293; q = 1-p=1-0.526=0.707; d = absolute allowable error, 5% of sample size.
By expecting 29.3% of incidence of backpain from assessed patients at 95% confidence level, so n= (1.96)2x 0.293 x (1-0.293)/ (0.05)2=318. Thus, the actual sample size for the current study is 318.
Sampling procedure
Study participants were selected using systematic random sampling technique. Depending upon average values of previous surgical procedures per month (N=960) and our sample size (n=318), the value for sampling interval Kth was calculated as Kth=N/n = 960/318= 3. A random number 3 was chosen and then every 3rd new study patient was included. It continued till the required sample size was completed.
Data collection tools and procedures
Data were collected using structured questionnaires by chart review and patient interview. Data were collected by two BSC anesthesia professionals and supervised by one MSC anesthetist. Training was given for data collectors and supervisor. Regular supervision and follow up was made. The data collection process was supervised by a principal investigator. The data collection procedure was continued for 3 consecutive months.
Data quality assurance
After the pretest was done, data collectors and supervisor were trained on each item included in the study. After the data were composed and checked for completeness, they were arranged, categorized and summarized.
Data processing and analysis
Data were checked manually for completeness and entered into SPSS version 20 computer program for analysis. Descriptive statistics was used to explain in data, tables and figures. Bivariate and multivariate analysis was used to identify factors associated with post spinal back pain. All independent variables were analyzed using binary logistic regression with the dependent variable being post spinal back pain; those with a p-value of ≤ 0.2 were fitted to a multivariate logistic regression to check their association with the outcome variable. Odds ratio and 95% confidence interval were computed to identify associated factors.
Ethical considerations
Ethical clearance and approval were obtained from Institutional Review Committee, Asella Health Science College, Arsi University. Permission to conduct and consent was obtained from Asella Teaching and Referral Hospital. Informed verbal consent was secured from every study participants prior to the interview and after telling them about the objective of the study. Confidentiality and anonymity were secured.
RESULTS
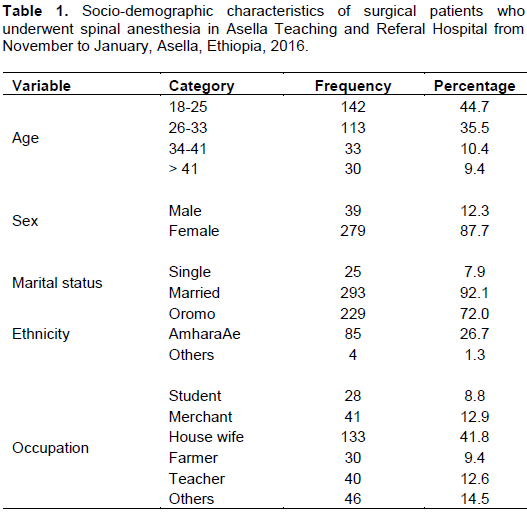
Total number of surgical patients included in the study was 318. Among them, the highest number 142(44.7%) belonged to the age group of 18-25 years. The mean age of respondents was 29.65 ±SD (11.642) (minimum 18 and maximum 76). 133 (41.8%) were House wives. 72% of the total participants were Oromo. Almost all (92.1%) of them were married. Majority (87.7%) of them were females (Table 1).
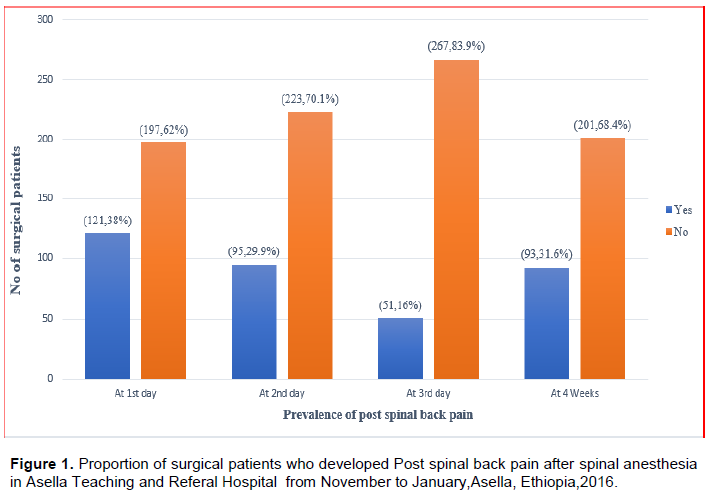
Prevalence of post spinal back pain
Postoperatively, 1st day data displayed 121(38%) of the study participants (n=318) experienced back pain but 62% of them showed no postop backache. 95(29.9%) of the respondents (n=318) experienced back pain on the second post-operative day. Post-operative 3rd day data displayed 51(16.0%) of the participants (n=318) experienced back pain. 93(31.6%) of the participants (n=294) experienced back pain at 4th week post- operative day and the rest 68.4% showed no backache (Figure 1).
Factors associated with post spinal back pain after surgical procedures in the study participants
Totally 318 participants were involved in our study. Among the 318 patients, 24 of them were lost to follow-up at the end of fourth week. A total of 294 participants were involved at the end of 4th week with response rate of 92.4% (Table 2).
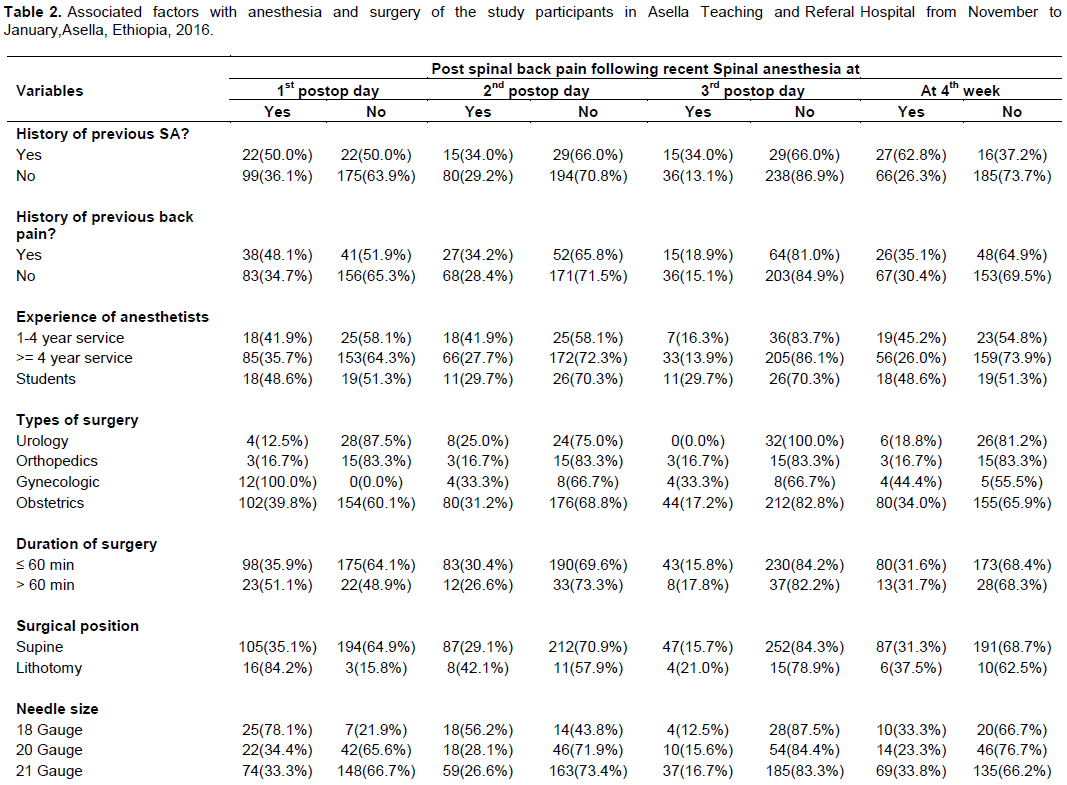
Among the participants, the highest percentage of backache (62.8%) happened at 4th week of postoperative day in patients who have history of previous spinal anesthesia and the least (34.0%) happened similarly at 2nd and 3rd postop days.
According to the experience of the anesthetists, the highest proportion of backache (48.6%) happened similarly at 1st and 4th week of postoperative day with anesthesia students and the lowest percentage of backache was at 3rd (13.9%) day with anesthetists having >=4 years experience.
Among the numerous types of surgical procedures involved in the study, the second highest percentage (39.8%) happened at 1st postoperative day in patients who underwent obstetric operation. The lowest incidence (12.5%) was on 1st postoperative day in patients who underwent urologic operation.
Postspinal backache was found to be more common with longer duration of surgery compared with short duration of surgery at 1st day (51.1 vs 35.9%) and Lithotomy position causes higher percentage (84.2%) of backache at 1st postoperative day than supine.
Among the participants whose sites of injection were infiltrated with local anesthetics, 36.7% of them developed backache in the 1st post-operative day. Use of 18 gauge needle size causes highest incidence (78.1%) of backache than 20 gauge (34.4%) needle at 1st day.
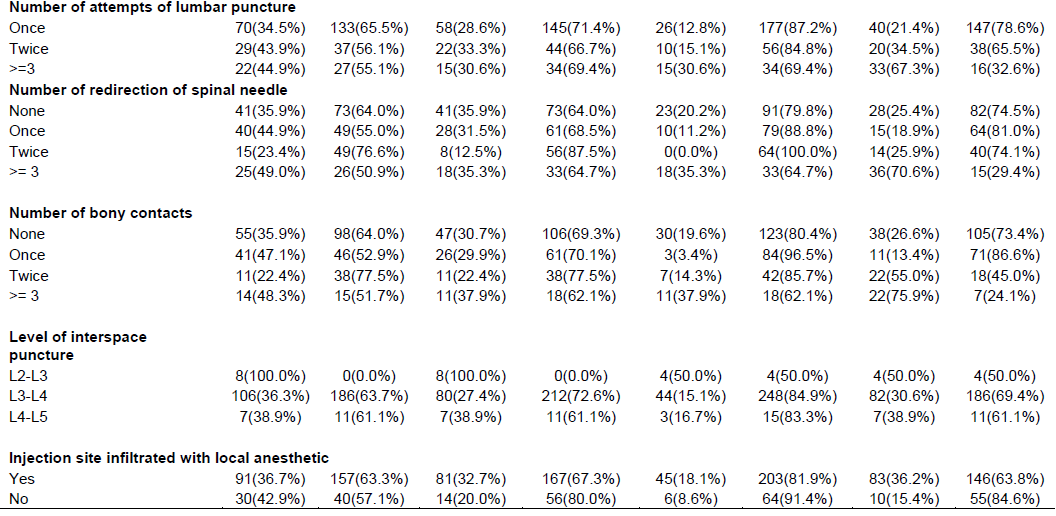
Number of attempts of lumbar puncture has direct relationship with incidence of post spinal backache. Attempt of lumbar puncture >=3 at 1st postoperative day and end of 4th week have postoperative incidence of 44.9 and 67.3% respectively.
Also number of bony contacts has direct relationship with incidence of post spinal backache. Bony contacts >=3 in the 1st day and at 4th week postoperative have the highest incidence of backache (48.3 and 75.9%) than < 3 times bony contacts.
Multivariate analysis of factors associated with post spinal back pain
38% of respondents experienced back pain on the first post-operative day. Multivariate analysis of associated factors showed that history of previous backache, history of previous spinal anesthesia, needle size and experience of the anesthetists displayed statistically substantial relevance with back pain (Table 3).
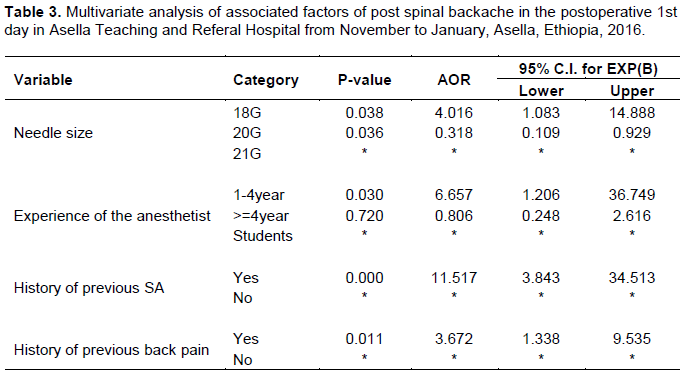
Patients with history of backache are 4 times more likely to develop post spinal backache than patients who do not have history of back pain at post-operative 1st day. (AOR = 3.672, 95% CI: 1.338, 9.535). History of previous spinal anesthesia was significantly associated with progress of post spinal backache. Patients who have history of previous spinal anesthesia were 11 times more likely to develop post spinal backache than patients who have no history of previous spinal anesthesia at post-operative 1st day (AOR = 11.517, 95% CI: 3.843, 34.513).
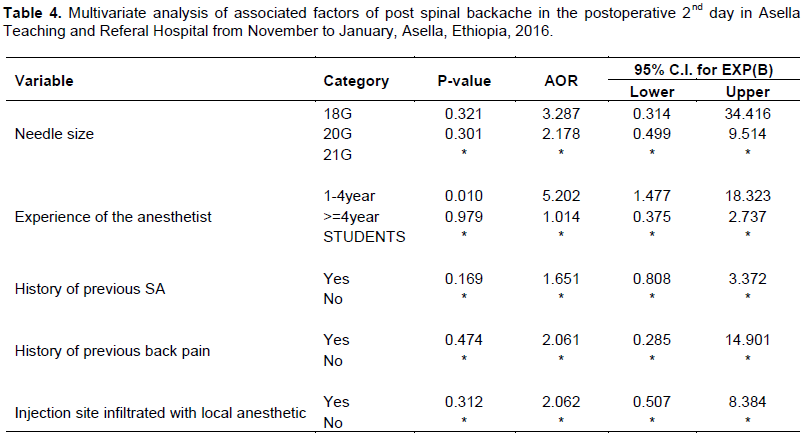
Patients who underwent surgery under spinal anesthesia with 18-gauge spinal needle was 4 times more likely to develop backache than with 20 and 21 gauges spinal needle at post-operative 1st day (AOR = 4.016, 95% CI: 1.083, 14.888). Spinal anesthesia that was given by anesthetist who have experience of 1-4 years was 7 times more likely for the development of backache than anesthetists who have >= 4-year experience at post-operative 1st day (AOR = 6.657, 95% CI: 1.206, 36.749). 29.9% of the respondents experienced back pain on the second post-operative day. Multivariate analysis of associated factors showed that history of previous backache, history of previous spinal anesthesia, needle size, infiltration of site with local anesthetics and experience of the anesthetists displayed statistically substantial relevance with back pain (Table 4).
Patients with history of backache are 4 times more likely to develop post spinal backache than patients who do not have history of back pain at post-operative 1st day. (AOR = 3.672, 95% CI: 1.338, 9.535). History of previous spinal anesthesia was significantly associated with progress of Post spinal backache. Patients who have history of previous spinal anesthesia were 11 times more likely to develop post spinal backache than patients who have no history of previous spinal anesthesia at post-operative 1st day (AOR = 11.517, 95% CI: 3.843, 34.513.
Patients who underwent surgery under spinal anesthesia with 18-gauge spinal needle was 4 times more likely to develop backache than with 20 and 21 gauge spinal needles at post-operative 1st day (AOR = 4.016, 95% CI: 1.083, 14.888). Spinal anesthesia that was given by anesthetists who have experience of 1-4 years was 7 times more likely for the development of backache than anesthetists who have >= 4-year experience (AOR = 6.657, 95% CI: 1.206, 36.749).
On the other hand, patients who underwent spinal with prior infiltration of the injection site with local anesthesia are 4 times less likely to develop than patients who underwent spinal anesthesia without infiltration of the injection site with local anesthesia at postoperative first day (AOR = 0.261, 95% CI: 0.138, 0.492). 16.0% of the respondents experienced back pain on the third post-operative day.
Multivariate analysis of associated factors showed that history of previous backache and history of previous spinal anesthesia displayed statistically significant relevance with backache (Table 5). Patients with history of backache are 3 times more likely to develop post spinal backache than patients who do not have history of back pain at post-operative 3rd day (AOR = 2.817, 95% CI: 1.036, 7.660). History of previous spinal anesthesia was also associated with progress of post spinal backache.
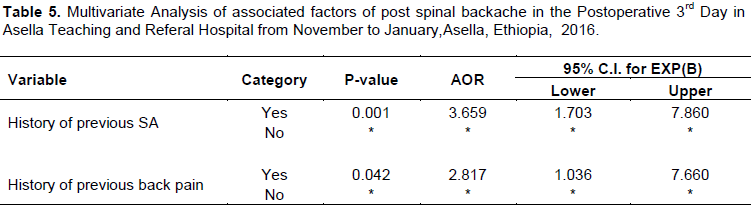
Patients who have history of previous spinal anesthesia were 4 times more likely to develop post spinal backache than patients who have no history of previous spinal anesthesia at post-operative 3rd day (AOR = 3.659, 95% CI: 1.703, 7.860). 31.6% of the respondents experienced back pain at 4th week post-operative day. Multivariate analysis of associated factors showed that history of previous backache, history of previous spinal anesthesia, needle size and infiltration of site with local anesthetics displayed statistically substantial relevance with backache (Table 6).
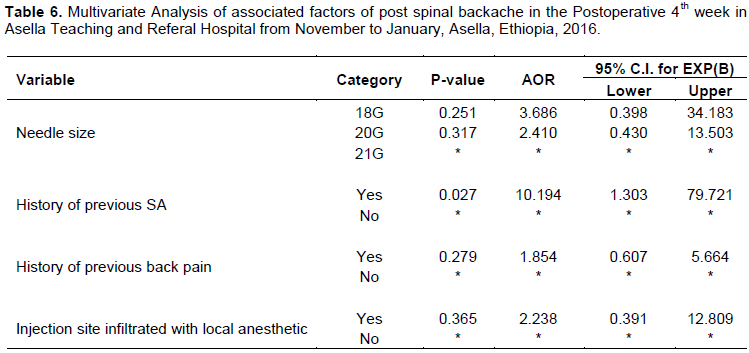
Patients with history of backache are 2 times more likely to develop post spinal backache than patients who do not have history of back pain at post-operative 4th week (AOR = 3.1.854, 95% CI: 0.607, 5.664). History of previous spinal anesthesia was significantly associated with progress of post spinal backache. Patients who have history of previous spinal anesthesia were 10 times more likely to develop post spinal backache than patients who have no history of previous spinal anesthesia at post-operative 4th week (AOR = 10.194, 95% CI: 1.303, 79.721).
Patients who underwent surgery under spinal anesthesia with 18-gauge spinal needle was 4 times more likely to develop backache than with 21-gauge spinal needles at post-operative 4th week (AOR = 3.686, 95% CI: 0.398, 34.183). Patients who underwent surgery under spinal anesthesia with 20-gauge spinal needle was 2 times more likely to develop backache than with 21-gauge spinal needles at post-operative 4th week (AOR = 2.410, 95% CI: 0.430, 13.503).
On the other hand, patients who underwent spinal anesthesia with prior infiltration of the injection site with local anesthesia are 2 times less likely to develop than patients who underwent spinal anesthesia without infiltration of the injection site with local anesthesia at postoperative 4th week (AOR = 2.238, 95% CI: 0.391, 12.809).
DISCUSSION
Post-operative back pain following spinal anesthesia has been shown to be a common complication of anesthesia and surgery. Reducing back pain incidence is mandatory to expand anesthetic outcomes.
In our study, prevalence of post spinal backache in the 1st day, 2nd day, 3rd day and at 4th week showed 38.0, 29.9, 16.0 and 31.6% of the participants suffered back pain respectively. This finding was high compared with study conducted in Turkey which displayed 29.3% of them suffered backache at 1st postoperative day and 5.2% of them experienced backache at 4th postoperative week, but no changes in postoperative back pain at 2nd day and 3rd day post-operatively (Tekgül et al., 2015). And our result was high than the study done in Iran as incidence of backache after spinal anesthesia was 12.2% at postoperative 4th week (Joudi et al., 2014). This variance may be due to use of lesser and less traumatic spinal gauge and harsh postoperative pain management. In our country, most of the patients get involved in their daily activity after being discharged from hospital; this may exacerbate the back pain. That is why at the 4th week the incidence becomes high.
In this study, number of attempts of lumbar puncture has direct relationship with incidence of post spinal backache. In Iran, 2010 a study was done on the incidence of backache after spinal anesthesia and its relationship with different factors in 176 patients; there was no significant change in the incidence of backache after spinal anesthesia where there was repeated attempts of dura (Eidy et al., 2010). This variance might be due to small quantity of patients or less attempts of spinal puncture.
Findings of our study explore conditions of spinal needle used during the procedures and backache after spinal anesthesia using 18 gauge,20 gauge and 21 gauge with postspinal backache incidence of 78.1,34.4 and 33.3% respectively. Similarly, comparative study done in Italy discovered that more patients administered spinal anesthesia with 22-gauge needle suffered backache in relation to those who were administered spinal anesthesia with 25-gauge needle (Pittoni et al., 1995). This similarity showed that needle size has significant association with post spinal backache. This studies finding displayed that in participants with previous history of back pain, nearly half (48.1%) of them develop backache or the back pain persists on the 1st postoperative day after current surgery. Similarly, Schwabe and Hopf studied that pre-existing back pain was the only variable associated with persistent back pain after 3 months of spinal anesthesia (Schwabe and Hopf, 2001).
Our study found history of previous spinal anesthesia as one of the common associated factors (50.0% at 1st postop day and 62.8% at 4th week) of post spinal back pain. And similarly, in orthopedic surgery, incidence of postoperative back pain at 1st, 2nd, 3rd days and 4th week was 16.7%. In a study conducted by Haghighi et al., it was said that history of previous spinal anesthesia is among the factors related with incidence of post spinal back pain, and in orthopedic surgery they found post-operative back pain incidence of 16, 9, and 35% in 1st day, week and month, respectively. The difference of results between these two studies can be attributed to the duration of surgery (Haghighi et al., 2012).
In this study, number of attempts of lumbar puncture was observed to have direct relationship with incidence of post spinal back pain. As incidence of back pain at 1st post-operative day with once vs. twice >=3 attempts were 34.5, 43.9 and 44.9%, respectively. Findings of certain studies shown in the past disclose that number of attempts taken of effective spinal anesthesia increases risk of trauma and possible back pain after surgical operation (Rafique and Taqi, 2011). Therefore, it is better to reduce number of attempts.
CONCLUSION
In our study, the prevalence of post spinal backache at postoperative 1st, 2nd, 3rd days and at 4th week data displayed 38.0, 29.9,16.0 and 31.6% of participants, respectively. History of previous backache, history of previous spinal anesthesia and needle size were the common factors differentiated in patients. Experience of the Anesthetists is the common factor in patients with backache on postoperative 1st and 2nd days. Also, infiltration of injection site with local anesthetic is a risk factor in patients with backache on 2nd day and at 4th week.
RECOMMENDATIONS
Awareness creation should be done about the problem for all health professionals managing patients after operation. Professionals have to inform patients that surgery under spinal anesthesia may cause backache which can be treated and managed. Use of smaller and less traumatic spinal needle size, infiltration of the injection site with local anesthetic prior to surgery and firm postoperative pain management rules should be given. Further study should be conducted with large sample size.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
We would like to thank all the staffs of Asella Teaching and Referral Hospital, Anesthesia Department for providing evidence.
REFERENCES
|
Brooks R, Oudekerk C, Olson R, Daniel C, Vacchiano C, Maye J (2002). The effect of spinal introducer needle use on postoperative back pain. AANA Journal 70(6):449-455. |
|
|
Campbell J, Sultan P (2009). Regional anaesthesia for caesarean section: a choice of three techniques. British Journal of Hospital Medicine 70(10):605-605. |
|
|
Cook T, Counsell D, Wildsmith J (2009). Major complications of central neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. British Journal of Anaesthesia 102(2):179-190. |
|
|
Eidy M, Ansari M, Hosseinzadeh H, Kolahdouzan K (2010). Incidence of back pain following spinal anesthesia and its relationship to various factors in 176 patients. Pakistan Journal of Medical Sciences 26:778-781. |
|
|
Haghighi M, Mardani KM, Mohammadzadeh A, Etehad H, Soleymanha M, Mirbolook A (2012). Evaluation of correlative factor of backache and headache after spinal anesthesia in orthopedic surgery. Journal of Guilan University of Medical Sciences 21(82):31-38. |
|
|
Hoy D, Brooks P, Blyth F, Buchbinder R (2010). The epidemiology of low back pain. Best Practice and Research Clinical Rheumatology 24(6):769-781. |
|
|
Joudi M, Fathi M, Amin DS, Ardabili AM, Akhondi M, Izanloo A (2014). The association of anesthetic method with developing back pain after lower extremity operations. Anesthesiology and Pain Medicine 4(5). |
|
|
Pittoni G, Toffoletto F, Calcarella G, Zanette G, Giron G (1995). Spinal anesthesia in outpatient knee surgery: 22-gauge versus 25-gauge Sprotte needle. Anesthesia and Analgesia 81(1):73-79. |
|
|
Rafique MK, Taqi A (2011). The causes, prevention and management of post spinal backache: an overview. Anaesthesia, Pain & Intensive Care 15(1):65-69. |
|
|
Rhee WJ, Chung CJ, Lim YH, Lee KH, Lee SC (2010). Factors in patient dissatisfaction and refusal regarding spinal anesthesia. Korean Journal of Anesthesiology 59(4):260-264. |
|
|
Schwabe K, Hopf HB (2001). Persistent back pain after spinal anaesthesia in the nonâ€obstetric setting: incidence and predisposing factors. British Journal of Anaesthesia 86(4):535-539. |
|
|
Tekgül ZT, PektaÅŸ S, Turan M, Karaman Y, Çakmak M, Gönüllü M (2015). Acute back pain following surgery under spinal anesthesia. Pain Practice 15(8):706-711. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


