ABSTRACT
The objective of this study was to assess the demographic profile, severity of patient, co morbidity, length of stay (LOS) and management of community acquired pneumonia. The study was a prospective study and consist of 212 patients (>20 years of age) with community acquired pneumonia (CAP) hospitalized to the tertiary care hospital, situated in Karachi between 1st January, 2010 and 31st March, 2012. Information related to demography and socioeconomic condition (gender, age, education, occupation and household income) and clinical details includes, evaluating severity using pneumonia severity index (PSI) score, laboratory finding, initial antibiotics prescribed, and hospital stay were composed. Demographic, socioeconomic and clinical variables were analyzed using descriptive statistics which is presented as percentage, frequencies, range and means. 116 (54.7%) patients had less severe pneumonia; 60 (28.3%) patients had moderately severe CAP and 36 (16.98%) patients had severe pneumonia. Commonly prescribed monotherapy of antibiotics initially on hospitalization were intravenous ceftriaxone 36 (16.98%). We recommend prospective multicenter setting studies to analyze the prevalence and burden of CAP in Pakistan. Improved assessment and proper utilization of guidelines is mandatory in the management of patients admitted with CAP.
Key words: Community acquired pneumonia (CAP), length of stay (LOS), antibiotic and pneumonia severity index (PSI).
Community-acquired pneumonia (CAP) is considered to be the most growing disease of the modern world (Pletz et al., 2016). Lower respiratory tract infections are considered to be the greatest reason of death in terms of infectious disease and third most common cause of death overall (
Wunderink and
Waterer, 2014). In European Union, 1 per 1000 of their population is a victim of CAP while 68.8% individuals suffering from CAP required hospitalization (Blasi et al., 2013). In United States of America, the frequency of CAP is around 3 to 5 cases per 1000 individuals with mortality of 5.0 to 15.0% which were hospitalized. Hence, CAP is categorized as one of the infectious diseases that require sudden hospital attention in all countries of the world (Onyedum and Chukwuka, 2011). Around 1.9 million deaths per year are being caused by pneumonia (
Ramachandran et al., 2011). According to the study conducted in Karachi related to seasonal variation in incidence of community acquired pneumonia, it stated that an average of 77 cases per month of community acquired pneumonia were reported in hospitals in Karachi (Raza et al., 2012). The most populous and largest city of Pakistan is Karachi and it is ranked as the 7th most populous urban city in the world.
An estimated population of Karachi is over 23.5 million people as of 2013 (Karim and Afzal, 1995). Chlamydophila pneumoniae causes respiratory tract infections including pneumonia. It has been diagnosed in the last 15 years where C. pneumoniae is the pathogen that causes CAP (Chedid et al., 2007). Elderly individuals are more prone to CAP in comparison to younger individuals (Stupka et al., 2009). The treatment guideline available and used in our country is Pakistan chest society, used for the management of community acquired pneumonia in adults and include; Inpatient and non-ICU treatment.
(a) A β-lactam plus macrolide (Preferred β-lactam agents include ampicillin; 500 mg-1 gm tid/Benzyle Penicillin 1.2-2.4 Gm qds (600 mg = one million units), cefotaxime, ceftriaxone. (A respiratory fluoroquinolone should be used for penicillin allergic patients).
(b) A respiratory fluoroquinolone or a macrolide alone.
Due to increase in resistance rates it is recommended that empirical therapy with single agent can be used only for the treatment of carefully selected hospitalized patients with no severe disease (http://www.pakistanchestsociety.pk.).
This is a prospective study, consisting of 212 patients with CAP hospitalized to the public sector hospital between 1st January, 2010 and 31st March, 2012. The hospital is situated in Karachi, Pakistan, and has 1185 beds, which is a tertiary care center, an area with a population of approximately 23.5 million people as of 2013 (
http://tribune.com.pk, 2014). This hospital is one of the largest public hospitals in the city. The inclusion criteria consist of over 20 years of age, having been diagnosed with pneumonia (which has chest X-ray findings and presence of one or more symptoms). The exclusion criteria consist of HIV patients and pregnant women believe to have nosocomial pneumonia. The study design was accepted and supported by the Research Ethics Committee of the University, attached with the hospital.
On admission, the following demo-graphic parameters were retrieved that is gender, age, education, marital status, smoking habits and occupation. The patients were categorized based on pneumonia severity index (PSI) (Corrêa and Lundgren, 2009; Fine et al., 1997). This study received no funding support. The null hypothesis was that, there is no difference in socioeconomic and demographic proportions distribution of CAP. The collected data was examined by SPSS-15. Demographic and clinical variables were calculated by using descriptive statistics.
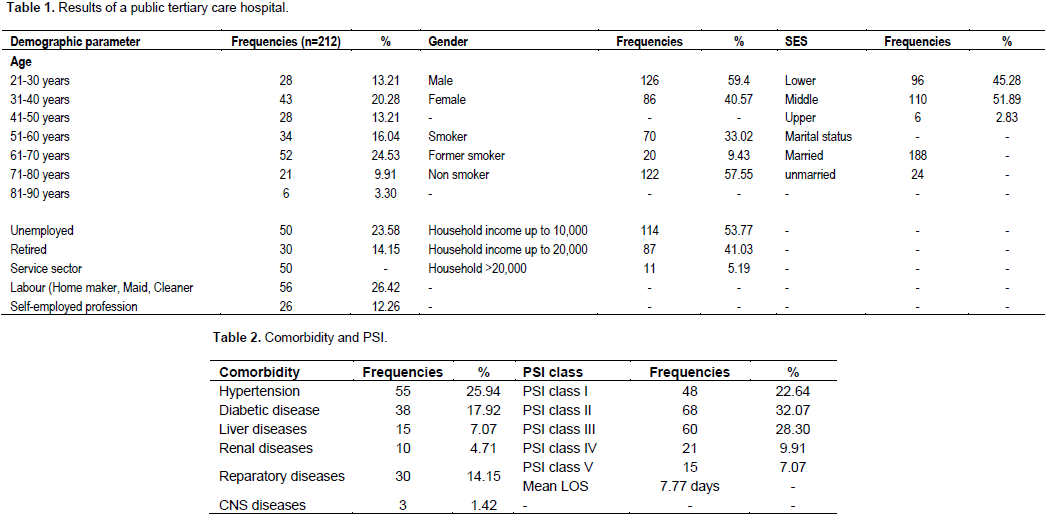
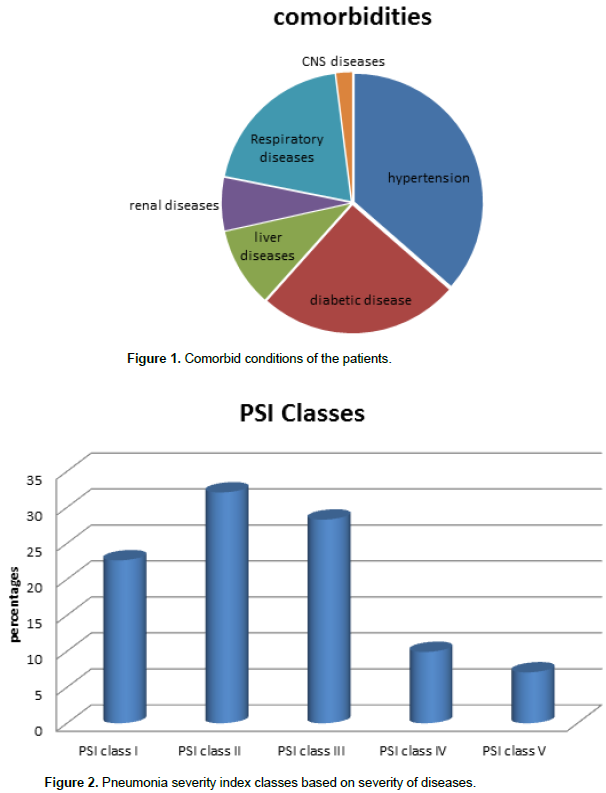
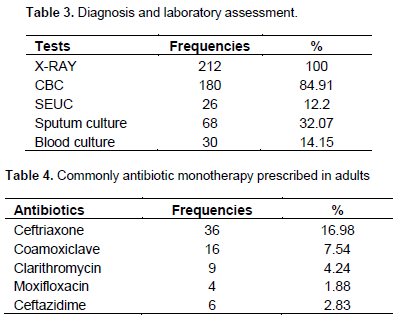
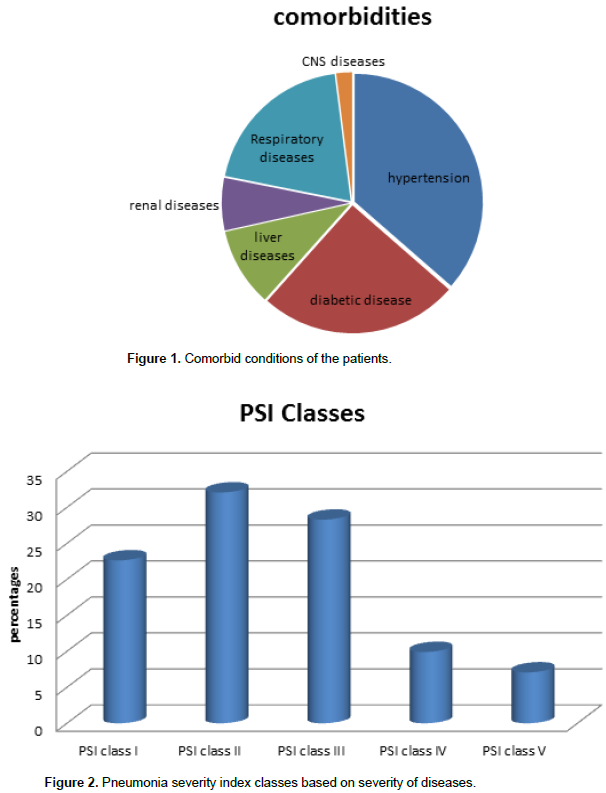
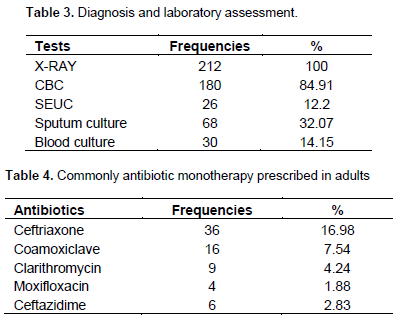
Table 1 summarizes the socioeconomic and demographic profile of the patients. Overall, 212 patients with CAP (mean age 52 years (range: 20 to 90 years), 126 (59.4%) male and 86 (40.57%) females were recruited in this study. Regarding occupation, 50(23.58%) was unemployed. In Table 2 it is summarized that at admission, 151(71.22%) were associated with comorbid condition, 55(25.94%) possess hypertension diseases and 38(17.92%) possess diabetic disease all these were the most commonly comorbid conditions. Mean length of stay in hospital was 7.77 days in patients hospitalized due to community acquired pneumonia. Most commonly occurring symptoms were cough, sputum production and breathlessness. 116 (54.7%) patients had less severe pneumonia, 60 (28.3%) had moderately severe CAP and 36 (16.98%) patients had severe pneumonia. Community acquired pneumonia (CAP) is a serious illness of respiratory system which is prevalent and occur both in developing and developed nations. Its frequency and severity change with different human demographic features (Figures 1 and 2).
Complete studies which analyze the profile, management and outcome of patients with CAP are not easily obtain in Pakistan and those that had been found, majorly focused on the etiological profile and were performed in children. The main findings were;
i. It was inspected that the frequency of CAP was inversely proportional to the socio-economic class. The lower class exhibits the highest frequency (53.77%) of CAP patients.
ii. Hospitalized cases were mainly the male patients with CAP.
iii. The frequency of patients with age 61 to 70 years comprised 24.53% of those hospitalized.
iv. The percentage of patient who was admitted with CAP and may not need admission at this center was 54.71% which had less severe pneumonia with PSI score of I and II.
v. it was found that comorbidity were frequent in patients with CAP and the hypertension was frequently found in 25.94% of those that were screened.
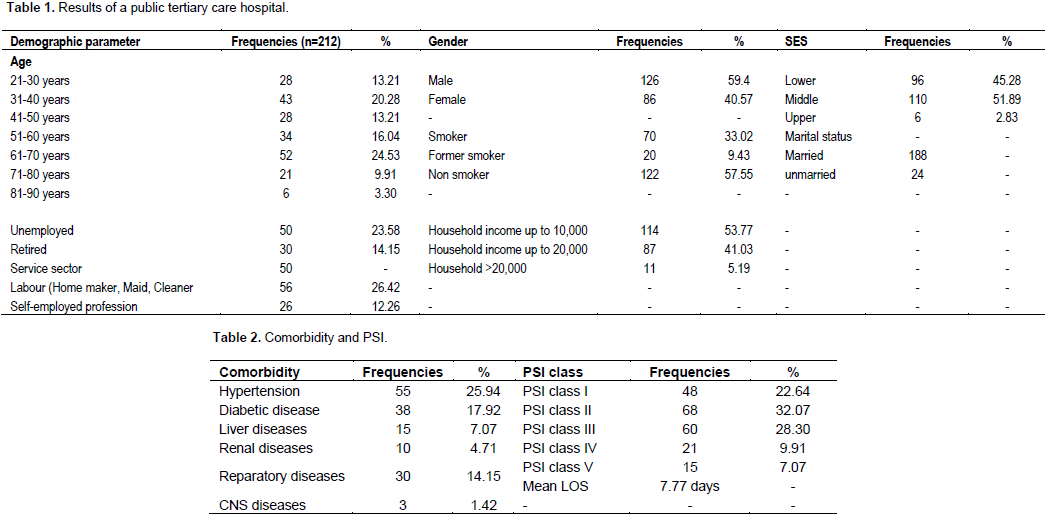
vi. X-rays and CBC were most commonly recommended in the laboratory and diagnostic tests. The most commonly prescribed antibiotic was ceftriaxone in admitted patient due to CAP (Tables 3 and 4).
The greater frequency of male were hospitalized with pneumonia as reported in previous studies by Sow et al. (1996), Fiberesima and Onwuchekwa, (2007) and Man et al. (2007). Older people were further affected with about 35% of them, being older than 65 years of age. This is not astonishing as, it exhibit that elderly people tend to have more attacks of severe CAP which have greater chance to be hospitalize during the cause of the disease. In the present study, the laboratory assessment was that x- ray were prescribed for 100% patients and sputum culture was prescribed for 32% patient, same result were reported in a study in which it is reported that 100% patents were recommended for chest X-rays and 31% were prescribed for sputum culture (Onyedum and Chukwuka, 2011). However 71.21% of the total number of patients had comorbidity illness associated with comorbid hypertension, diabetic disease, liver diseases, renal disease, respiratory disease, CNS diseases while 61(28.77%) patients were without comorbidity etc. This is higher than what was obtained in other study conducted in 2011 in Nigeria (Onyedum and Chukwuka, 2011) with comorbidity prevalence 38.8%.
The PSI categorization recommend that a large part of patients who could be treated as outpatients were admitted, this was particularly true for 54.71% patients, and were associated with PSI I or II. Inversely, the PSI classified 45.28% of CAP cases among the patients as cases for hospitalization. Generally patient was from very low income class, living low profile areas where opportunity to approach health care facilities can be examined poorly and the decision rates are examined as low. The teams who initially assess patients selected for admission in order to access the proper utilization of medications, as well as the upcoming clinical examination of patients, particularly the older individuals with chronic illness and similar pattern, were also found in other study conducted by Chedid et al. (2007). Frequently prescribed antibiotic at first on hospitalization was intravenous ceftriaxone alone (16.98%). To determine the evaluation of antibiotic, it is use in accordance to the criteria developed through the guideline of Pakistan chest society, for the management of community acquired pneumonia in adults for inpatient treatment. This study results showed that, only 16.98% patients were treated in accordance to this guideline. A wide variation exists in the treatment pattern of community acquired pneumonia in adults in this hospital setting.
Important consideration should be given to Severity assessment scores for CAP in the initial assessment of patients with CAP, to stop needless hospitalization. Majority of the patients tend to have co morbidities like diabetes mellitus and hypertension so, assessment of comorbidities should be done on priority bases. There is an urgent need to start the continuing medical education on institutional and national levels to make sure of the proper management of these cases.
REFERENCES
|
Blasi F, Garau J, Medina J, Ávila M, McBride K, Ostermann H (2013). Current management of patients hospitalized with community-acquired pneumonia across Europe: outcomes from REACH. Respiratory Res. 14(1):44.
Crossref
|
|
|
|
Chedid MB, Chedid MF, Ilha DO, Bozzetti MC, Chaves L, Griza D, Dalcin PR (2007). Community-acquired pneumonia by Chlamydophila pneumoniae: A clinical and incidence study in Brazil. Braz. J. Infect. Dis. 11(1):75-82.
Crossref
|
|
|
|
|
Corrêa Rde A, Lundgren FL (2009). Frare e Silva RL, Cardoso AP. Lemos AC, et al. Brazilian guidelines for community-acquired pneumonia in immunocompetent adults-2009. J. Bras. Pneumol. 35(6):574-601.
Crossref
|
|
|
|
|
Fiberesima FP, Onwuchekwa AC (2007). The prevalence of HIV and TB in acute CAP. Afr. J. Resp. Med. 3(1):23e6.
|
|
|
|
|
Fine MJ, Auble TE, Yealy DM, Hanusa BH, Weissfeld LA, Singer DE, Coley CM, Marrie TJ, Kapoor WN (1997). A prediction rule to identify low-risk patients with community-acquired pneumonia. New Engl. J. Med. 336(4):243-250.
Crossref
|
|
|
|
|
Karim MS, Afzal M (1995). Changing Demographic, Social, and Economic Conditions in Karachi City, 1959-94: A Preliminary Analysis [with Comments]. Pak. Dev. Rev. 34(4):1093-1106
|
|
|
|
|
Man SY, Lee N, Ip M, Antonio GE, Chau SS, Mak P, Graham CA, Zhang M, Lui G, Chan PK, Ahuja AT (2007). Prospective comparison of three predictive rules for assessing severity of community-acquired pneumonia in Hong Kong. Thorax 62(4):348-353.
Crossref
|
|
|
|
|
Onyedum CC, Chukwuka JC (2011). Admission profile and management of community acquired pneumonia in Nigeria-5 year experience in a tertiary hospital. Respiratory Med. 105:298-302.
Crossref
|
|
|
|
|
Pletz MW, Rohde GG, Welte T, Kolditz M, Ott S (2016). Advances in the prevention, management, and treatment of community-acquired pneumonia. F1000Research 5.
Crossref
|
|
|
|
|
Ramachandran P, Nedunchelian K, Vengatesan A, Suresh S (2012). Factors for mortality in community acquired pneumonia amoung children aged 1-59 months admitted in referral hospital. Available at:
View
|
|
|
|
|
Raza MZ, Ahmed A, Ahmed F, Ghani A, Rizvi N (2012). Seasonal incidence of community acquired pneumonia and its mortality in Karachi-A multi-centric hospital based study. Int. J. Environ. Sci. 3(2):885.
|
|
|
|
|
Sow O, Frechet M, Diallo AA, Soumah S, Conde MK, Diot P, Boissinot E, Lemarié E (1996). Community acquired pneumonia in adults: a study comparing clinical features and outcome in Africa (Republic of Guinea) and Europe (France). Thorax 51(4):385-388.
Crossref
|
|
|
|
|
Stupka JE, Mortensen EM, Anzueto A, Restrepo MI (2009). Community-acquired pneumonia in elderly patients. Aging Health 5(6):763-774.
Crossref
|
|
|
|
|
Wunderink RG, Waterer GW (2014). Community-acquired pneumonia. New Engl. J. Med. 370(6):543-551.
Crossref
|
|