ABSTRACT
Women living with human immunodeficiency virus (HIV) infection have a higher burden of premalignant lesion of the cervix. This may be influenced by their sociodemographic profile. To study the sociodemographic determinants of abnormal cervical cytology among HIV-positive women attending the adult HIV clinic in Nnamdi Azikiwe University Teaching Hospital Nnewi (NAUTH), Nnewi, Nigeria, the Pap smears of 110 HIV-positive women attending the adult HIV clinic at the hospital were evaluated for cytological abnormalities using the Bethesda system of classification. Data on sociodemographic factors were obtained with the aid of semi structured questionnaires. Epi info statistical package was used to analyze the data. Majority of the women were married (61.8%; n=68), traders (67.3%; n=74) and who had attained at least secondary education (85.5%; n=94). All of them were Christians. The mean age and parity were 37.7±9.5 years and 2.8±2.3, respectively. The mean CD4 count was 557.1± 26 cells/ml and 89.1% (n= 98) of the women were on highly active antiretroviral therapy (HAART). The prevalence of cervical cytological abnormalities among the studied women was 28.2% (n=31). The mean age (35.4 vs. 38.9 years; p<0.05) was significantly lower among women with positive cervical cytological abnormalities and the prevalence of cytological abnormalities was significantly high among women aged 25 to 29 years (c2=9.30, p=0.05), traders (c2=10.7, p=0.03) and the Anglicans (c2=6.7, p=0.04). The prevalence rate was also the highest among women who were para 0-1 (36.6%), unemployed (100.0%), with no formal education (33.3%), and those who were separated from their husbands (100.0%), but these were not statistically significant. The prevalence of cervical cytological abnormalities among the HIV positive women attending the HIV clinic in NAUTH was high. Younger age, being a trader and Anglican Christian denomination were significantly associated with increased risk of premalignant lesions of the cervix.
Key words: Cervical, cytological, premalignant lesions, human immunodeficiency virus (HIV) positive.
Cervical cancer is the commonest gynaecological cancer affecting women in the sub-Saharan Africa. In Nigeria, it accounts for majority of cancer related deaths and ill health among women (Bassey et al., 2007; Kyari et al., 2004; Uzoigwe and Seleye-Fubara, 2004; Obiechina et al., 2008). In our hospital, it is the commonest gynaecological cancer seen accounting for about 56% of all gynaecological malignancies managed in the hospital (Obiechina et al., 2008). This high burden of cervical cancer results from lack of organized screening program, widespread poverty, and ignorance prevalent in this resource constrained region of the world.
Cancer of the cervix is an AIDS defining condition (Clifford et al., 2006) and women living with HIV infection are known to have an increased prevalence of human papillomavirus (HPV) and an increased prevalence of high risk human papilloma virus (HR-HPV) (Freitas et al., 2015), and a greater likelihood of persistent infections (Beachler et al., 2015) when compared with their human immunodeficiency virus (HIV)-negative counterparts. This is as a result of immunosuppression. There is therefore an indication for routine cervical cancer screening among this population of women.
There have been conflicting reports about relationship between cervical cytological abnormalities and risk of HIV infection.
Kreitchmann et al. (2013) studied 898 women living with HIV infection and reported that age less than 30 years was significantly associated with increased risk of abnormal cervical cytology among the women. This was similar to the account of Musa et al. (2013) in Jos Nigeria who reported that age less than 30 years was significantly associated with the presence of high risk HPV DNA.
But in contrast, Liu et al. (2016) in their study of 1365 Tanzanian HIV positive women who had cervical cancer screening, reported that age more than 50 years was significantly associated with the occurrence of cervical cytological abnormalities. Similarly, Ononogbu et al. (2013) studied 2501 HIV positive women in Abuja, Nigeria and reported that increasing age and age >40 years were associated with reduced risk of developing premalignant lesions of the cervix among the women.
However, Obure et al., (2009) reported no influence of age, education, parity and age at sexual debut on the risk of abnormal Pap smear among Tanzanian HIV positive women. Only marital status and multiple sexual partners were significantly associated with an increased risk of cervical cytological abnormalities among the women.
In our environment, no study has elucidated the important association between sociodemographic profile and the risk of premalignant lesions of the cervix among the HIV positive women.
This study therefore, aimed at examining the relationship between sociodemographic profile and the risk of premalignant lesions of the cervix among HIV positive women accessing care in our hospital. The aim of this work was to determine the sociodemographic determinants for cervical cytological abnormalities among HIV infected women attending the adult HIV clinic in Nnamdi Azikiwe University Teaching Hospital Nnewi. The objectives include to 1) determine the sociodemographic characteristics of HIV positive women attending the HIV clinic in NAUTH who have cervical cytological abnormalities among HIV infected women; (2) to determine the statistical relationship between education, age, occupation and parity with cervical cytological abnormalities among HIV infected women attending the adult HIV clinic in NAUTH; (3) to make recommendations on screening for cervical cytological abnormalities among the women.
Null hypothesis
There is no relationship between sociodemographic characteristics and cervical cytological abnormalities among HIV positive women attending the HIV clinic in NAUTH.
Study design
This is a cross sectional study that was carried out among HIV-positive women who were attending the adult HIV clinic in Nnamdi Azikiwe University Teaching Hospital Nnewi.
Study area
Nnamdi Azikiwe University Teaching Hospital Nnewi is a tertiary health institution with a catchment area of the five states of the South East Geopolitical Region of Nigeria. These are Anambra, Enugu, Abia, Imo, and Ebonyi States. Referral was also received from some parts of Delta State of Nigeria. The HIV department operates three clinics, viz, the adult HIV clinic, the pediatric HIV clinic and the PMTCT clinic. The department is sponsored by Institute for Human Virology and offers free counseling, testing and treatment for all the clients. Clients were recruited from all the catchment areas and beyond.
Study population
The study population comprised 110 HIV positive women attending the HIV clinic in the hospital.
Inclusion criteria
All HIV positive women attending the clinic.
Exclusion criteria
Women with a history of cervical cancer, women who previously treated premalignant lesions of the cervix, and pregnant women.
Sample size
The minimum sample size was determined by using the statistical formula of Fisher for calculating sample size (Araoye, 2003).
N= Z2pq/d2
Where, N = minimum sample size for a statistically significant survey; Z = normal deviant at the portion of 95% confidence interval = 1.96; P = prevalence value of cervical cytological abnormalities among HIV positive women in Nnewi, Nigeria = 6.8% (Ugboaja and Monago, 2010); q = 1- p; d = margin of error acceptable or measure of precision = 0.05; N = 100; minimum sample size = 100; The sample size was adjusted to 110 to compensate for 10% attrition.
Therefore, 110 women were studied.
Data collection
Data on sociodemographic characteristics was obtained with semi-structured interviewer- administered questionnaires. Consecutive HIV-positive women attending the adult HIV clinic in Nnamdi Azikiwe University Teaching Hospital Nnewi were educated on the purpose, value and the nature of the study and their consent were sought.
Those that met the inclusion criteria and gave consent for the study were recruited and had the questionnaire administered to them by the researcher to obtain the following data; age, last menstrual period, parity, level of education, occupation, occupation of the husband and whether the patient was on highly active antiretroviral therapy (HAART) or not.
A proforma form was attached to the questionnaire to record the laboratory findings. The patients were assigned to social classes utilizing the method developed by Olusanya et al. (1985) which considers the educational level of the woman and the occupation of the husband.
Sample collection
After completion of the questionnaire, 5 ml of venous blood was obtained from the cubital fossa for measurement of CD4 count in the laboratory, while cervical smear was obtained for Pap smear screening. The Pap smear was collected with Ayre’s spatula and smeared evenly on a slide which was immersed instantly in 95% alcohol. The samples were read by trained cyto-pathologist.
Data analysis
Statistical analysis of the data collected was done with Epi-info statistical package, version 3.5.2(2008). Continuous variables were expressed as means and standard deviations and categorical variables as percentages. Statistical relationships between sociodemographic characteristics and cervical cytological abnormality explored with Pearson’s Chi square and Fischer exact tests. A p-value of <0.05 at 95% confidence interval was considered as statistically significant. Bivariate logistic regression analysis was used to examine the predictive value of age category on the occurrence of cervical cytological abnormality.
Ethical considerations
Ethical approval for the study was obtained from the ethical committee of the hospital and the study protocol was made to conform to the ethical guidelines of the declaration of Helsinki (1975). As much as possible, the rights of the patients were fully protected in this research work. Only women who gave consent were recruited for the study.
The patients were required to fill the informed consent form. As much as possible, confidentiality was maintained at all stages of the research work. Every participating patient had the right to privacy and could withdraw from the study at any time after counseling. Patients also had the right to anonymity.
Benefits to patients
The patients appreciated their status with respect to Pap smear cervical cytological screening for cancer of the cervix and those of them who had abnormalities were further evaluated and treated where necessary.
Hazards of the research
The research had no hazards on the patients.
Inducement to patients
There was no form of payment to the patients before or after the screening exercise.
Sources of funding for the research
The cost of the research was borne entirely by the researcher. Patients did not pay for the screening exercise.
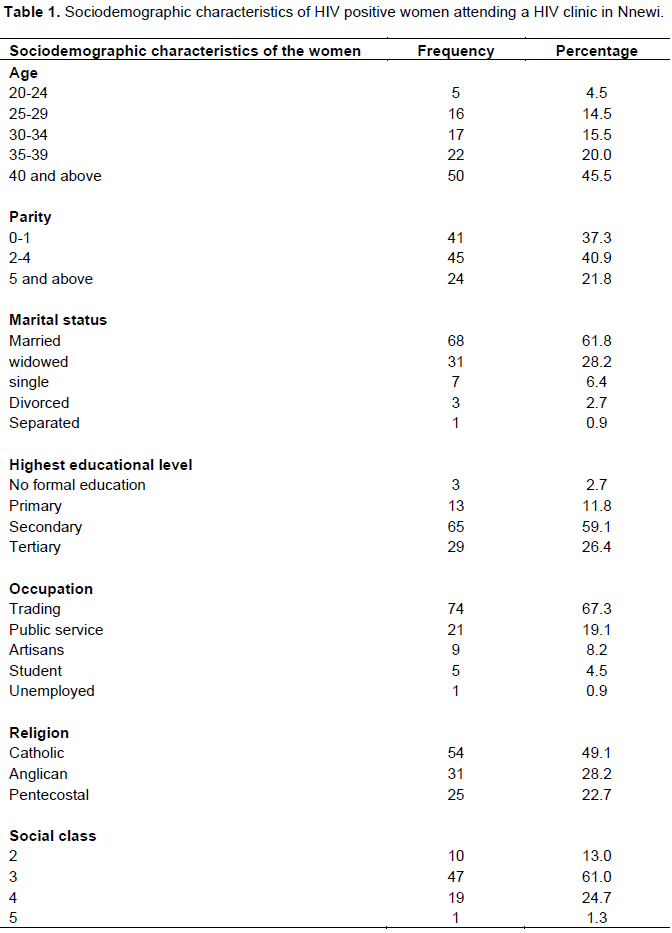
Sociodemographic characteristics of the women
As shown in Table 1, majority of the women were married (61.8%; n=68) and only 6.4% of them were single. They were mainly traders (67.3%; n=74) who had attained at least secondary education (85.5%; n=94) and all of them were Christians. The age of the women ranged from 20 to 61 years with a mean age of 37.7±9.5 years. The mean parity of the women was 2.8±2.3 2.8 and the modal parity group was 2 to 4 (multipara). Most of the women belonged to the low social class (classes 3 and 4) (85.7%, n=66). None of the women was smoking.
The mean age of coitache was 18.8±4 and 2.7% of the women had multiple sexual partners (>2 partners) in the 6 months preceding the study. The mean CD4 count was 557.1± 26 cells/ml and 89.1% (n= 98) of the women were on HAART
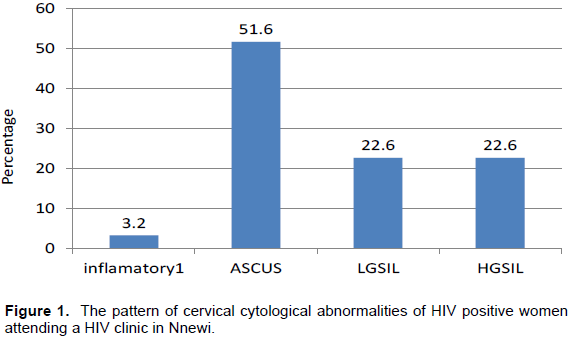
Prevalence and pattern of cervical cytological abnormalities among the women
Thirty one of the women had abnormal cervical cytological abnormalities giving a prevalence of 28.2%. Atypical squamous cells of undetermined significance (ASCUS) constituted the highest class of abnormality accounting for 51.6% (n=16) of all cases of abnormal cytology. Both low grade squamous intraepithelial lesion (LGSIL) and high grade squamous intraepithelial lesion (HGSIL) each constituted 22.6% (n=7) of all cases. This is as shown in Figure 1.
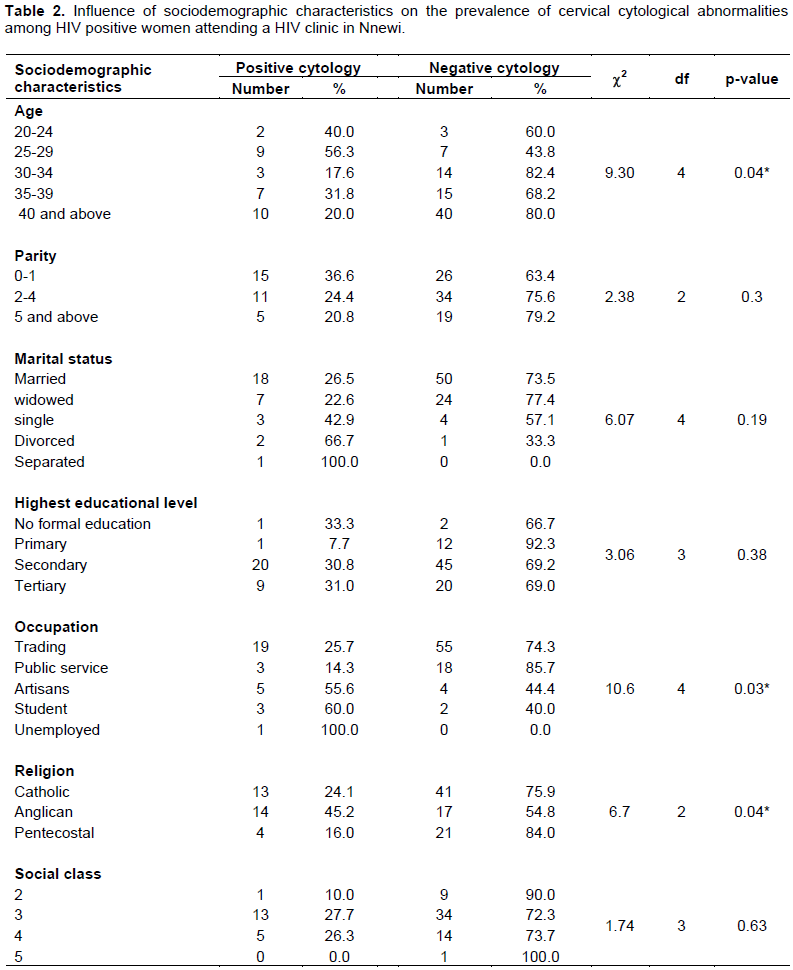
Influence of sociodemographic characteristics on the prevalence of cytological abnormalities among the women
Table 2 shows the influence of sociodemographic on the risk of cytological abnormalities among the women.
With respect to age, cervical cytological abnormality was significantly the highest among women aged 25 to 29 years (c2=9.30, p= 0.04). The mean age (35.4 vs. 38.9 years; p<0.05) was significantly lower among women with positive cervical cytological abnormalities.
The prevalence of cytological abnormalities was significantly the highest among the unemployed (c2=10.7, p=0.03).
The Anglican Christian denomination conferred a significant risk to the occurrence of cervical cytological abnormalities (c2=6.7, p=0.04). There was no significant relationship with marital status (c2=6.07, p=0.19) and educational level (µ2=3.06, p=0.38).
HIV infection is associated with an increased burden of premalignant and malignant lesions of the cervix. The prevalence of 28.2% as found in this study is high but comparable to 27% reported in UK by Hotonu et al. (2010) and 31.3% in Maiduguri, Northern Nigeria by Chama et al. (2005).
It is however lower than 68.3 and 43.7% prevalence rates reported in Jos, Nigeria by Agaba et al. (2009) and in Kenya by Mabeya et al. (2012). A lower rate of 12.6% was reported in Enugu by Dim et al. (2011).
These variations within the country may be attributable to different patients’ sociodemographic, cultural and sexual attributes. These include immunological status, use of antiretroviral drugs, and risky sexual behaviors.
This study found a significant association between lower age group and the risk of cervical cytological abnormalities among the women which was also seen during the bivariate analysis where age less than 30 years predicted the presence of the disease (OR=02). In addition, positive cytological abnormality was significantly associated with a lower mean age.
This association with a younger age had been reported by Musa et al. (2013) in Jos Nigeria, Kreitchman et al. (2013) and Koffi et al. (2010) in Central African Republic. This association may be derived from a more aggressive sexual activity by the younger women, as HPV infection which is the precursor for the premalignant lesions is a sexually transmitted infection. The younger women are more likely to involve in more risky sexual behavior including having more sexual partners.
Therefore, these women require closer surveillance and sensitization about healthy sexual habits including the need for consistent use of condoms and the need for regular screening for premalignant lesions.
However, the finding is in contrast to the reports of Liu et al. (2016) in Tanzanian and Ononogbu et al. (2013) in Abuja, Nigeria who found a significant association between increasing age and the risk of developing premalignant lesions of the cervix among the women.
Although there was no significant association of premalignant lesion with parity in this work, the rate was highest among the para 0-1 women and decreased as parity increased being lowest among the grandmultiparae. This is similar to the report of Lehtovirta et al. (2008) in Finland who noted that increasing parity decreased the risk of the disease. In their account, each pregnancy reduced the risk of the disease by 30%.
But Obure et al. (2009) reported no influence of parity on the risk of abnormal Pap smear among Tanzanian HIV positive women. In their account, only marital status and multiple sexual partners were significantly associated with an increased risk of cervical cytological abnormalities among the women.
These observed differences may relate to differing cultural and social attributes of the studied population.
With respect to occupation, this study found a significant association between high rates of abnormalities and being unemployed and also being in school. Women who are unemployed or in school will likely depend on their husbands or partners for their needs.
This may constitute a handicap in accessing reproductive health services, including screening for cervical cancer. Therefore, improving the socioeconomic status of the women infected with HIV should also be considered a priority for these women. This is specially so as societal stigmatization may limit the ability of women living with HIV/AIDS for social engagement and hence, wealth generation.
The prevalence of abnormal cervical cytology among the studied HIV positive women was high. Age less than 30 years and unemployment are the most important risk factors for the occurrence of the disease among the women. There is need to target this population of the women for cervical cancer screening while making efforts to improve the socioeconomic base of people living with HIV/AIDS.
The authors have not declared any conflict of interests.
REFERENCES
|
Agaba PA, Thacher TD, Ekwempu CC, Idoko JA (2009). Cervical dysplasia in Nigerian women infected with HIV. Int. J. Gynaecol. Obstet.107(2):99-102.
Crossref
|
|
|
|
Araoye MO (2003). Research methodology with statistics for health and social sciences. Ilorin: Nathadex Publisher. 115(9).
|
|
|
|
|
Bassey EA, Ekpo MD, Abasiasia A (2007). Female genital tract malignancies in Uyo, South-South, Nigeria. Niger. Post-grad. Med. J. 14(2):134-136.
|
|
|
|
|
Beachler DC, Sugar EA, Margolick JB, Weber KM, Strickler HD, Wiley DJ, Cranston RD, Burk RD, Minkoff H, Reddy S, Xiao W (2015). Risk factors for acquisition and clearance of oral human papillomavirus infection among HIV-infected and HIV-uninfected adults. Am. J. Epidemiol. 181(1):40-53.
Crossref
|
|
|
|
|
Chama CM, Nggada H, Gashau W (2005). Cervical dysplasia in HIV infected women in Maiduguri, Nigeria. J. Obstet. Gynaecol. 25(3):286-288.
Crossref
|
|
|
|
|
Clifford GM, Goncalves MA, Franceschi S (2006). Human papilloma-virus types among women infected with HIV: A meta-analysis. AIDS 20:2337-2344.
Crossref
|
|
|
|
|
Dim CC, Ezegwui HU, Ikeme AC, Nwagha UI, Onyedum CC (2011).Prevalence of cervical squamous intraepithelial lesions among HIV-positive women in Enugu, South-eastern Nigeria. J. Obstet. Gynaecol.31(8):759-762.
Crossref
|
|
|
|
|
Freitas BC, Suehiro TT, Consolaro ME, Silva VR (2015). HPV Infection and Cervical Abnormalities in HIV Positive Women in Different Regions of Brazil, a Middle-Income Country. Asian Pac. J. Cancer Prev. 16(18):8085-8091.
Crossref
|
|
|
|
|
Hotonu OE, Hussey J, Basta MS, Wadehra V, Cross P, Schmid ML (2010). An audit of cervical cytology in HIV-positive women. Cytopathology 21(2):116-119.
Crossref
|
|
|
|
|
Koffi B, Serdouma E, Mbolissa-Nguérékoudou W, Ngadjou-Kouchou-Fondjo M, Pengoussou-Gbatoumba V, Sépou A, Grésenguet G (2010). Cervical dysplasia in women with human immunodeficiency virus (HIV) in areas of high prevalence of infection. Gynecol. Obstet. Fertil. 38(10):576-580.
Crossref
|
|
|
|
|
Kreitchmann R, Bajotto H, Da Silva DA, Fuchs SC (2013). Squamous intraepithelial lesions in HIV-infected women: Prevalence, incidence, progression and regression. Arch. Gynecol. Obstet. 288(5):1107-1113.
Crossref
|
|
|
|
|
Kyari O, Nggada H, Mairiga A (2004). Malignant Tumours of the female genital tract in North Eastern Nigeria. East Afr. Med. J. 81(3):142-145
Crossref
|
|
|
|
|
Lehtovirta P, Paavonen J, Heikinheimo O (2008). Risk factors, diagnosis and prognosis of cervical intraepithelial neoplasia among HIV-infected women. Int. J. STD AIDS.19(1):37-41.
Crossref
|
|
|
|
|
Liu E, McCree R, Mtisi E, Fawzi WW, Aris E, Lema IA, Hertzmark E, Chalamilla G, Li N, Vermund SH, Spiegelman D (2016). Prevalence and risk factors of cervical squamous intraepithelial lesions among HIV-infected women in Dar es Salaam, Tanzania. Int. J. STD AIDS 27(3):219-225.
Crossref
|
|
|
|
|
Mabeya H, Khozaim K, Liu T, Orango O, Chumba D, Pisharodi L, Carter J, Cu-Uvin S (2012). Comparison of conventional cervical cytology versus visual inspection with acetic acid among human immunodeficiency virus –infected women in Western Kenya. J. Lower Genital Tract Dis. 16(2):92-97.
Crossref
|
|
|
|
|
Musa J, Taiwo B, Achenbach C, Olugbenga S, Berzins B, Sagay AS, Idoko JA, Kanki PJ, Murphy RL (2013). High-risk human papillomavirus among HIV-infected women with normal cervical cytology: a pilot study in Jos, Nigeria. Arch. Gynecol. Obstet. 288(6):1365-1370.
Crossref
|
|
|
|
|
Obiechina NJA, Ugboaja JO, Ezeama CO, Monago EN (2008). Pattern of primary gynaecological malignancies seen inNnamdi Azikiwe University Teaching Hospital, Nnewi; a ten-year review. Trop. J. Med. Res.12(2):47-49.
|
|
|
|
|
Obure J, Olola O, Swai B, Mlay P, Masenga G, Walmer D (2009). Prevalence and severity of cervical squamous intraepithelial lesion in a tertiary hospital in northern Tanzania. Tanzan. J. Health Res. 11(4):163-169.
|
|
|
|
|
Olusanya O, Okpere EE, Ezimokhai M (1985). The importance of social class in voluntary fertility control in a developing country. West Afr. J. Med. 4:205-212.
|
|
|
|
|
Ononogbu U, Almujtaba M, Modibbo F, Lawal I, Offiong R, Olaniyan O, Dakum P, Spiegelman D, Blattner W, Adebamowo C (2013). Cervical cancer risk factors among HIV-infected Nigerian women. BMC Public Health.13:582.
Crossref
|
|
|
|
|
Ugboaja JO, Monago EN (2010). The prevalence of cervical cytological abnormalities among HIV positive women in Nnewi, Nigeria. A paper presented at the 5th National conference on HIV/AIDS held in Abuja, Nigeria from 2nd to 5th May.
|
|
|
|
|
Uzoigwe SA, Seleye-Fubara D (2004). Cancers of the uterine cervix in Port-Harcourt, Rivers State; a 13 -year clinico-pathological review. Niger. J. Med. 13(2):110-113.
|
|