Full Length Research Paper

ABSTRACT
Chlorine dioxide has been condemned as a dangerous poison and has been touted as a cure for COVID-19. This narrative review examines the controversy surrounding the use of aqueous chlorine dioxide by investigating evidence-based research articles, government documents, press reports, and the results of the first clinical trial utilizing chlorine dioxide as a treatment for COVID-19. Chlorine dioxide was found to be employed by numerous industries for antimicrobial and other uses. Aqueous chlorine dioxide was found to be safe when ingested in low doses, but when ingested in high doses, it can cause adverse hematologic and renal effects. Additionally, chlorine dioxide was found to be a strong and rapidly acting virucide with activity against a wide range of viruses. Results of the first clinical trial utilizing chlorine dioxide to treat COVID-19 are reviewed and this molecule is found to be a safe and effective treatment. A dispassionate review of the evidence-based research literature finds preliminary evidence supporting the opinion that aqueous chlorine dioxide may be a safe and effective treatment of COVID-19, and likely for other viral illnesses as well. Further studies are needed to confirm these findings and to explore potential uses of chlorine dioxide.
Key words: SARS-CoV-2, virucide, biocide, antimicrobial, oxidant, disinfectant, bleach, food additive, sterilant.
Abbreviation: ACE2, Angiotensin-converting enzyme 2; ClO2, chlorine dioxide; COVID-19, Corona Virus Disease – 2019; EPA, US Environmental Protection Agency; EUA, Emergency Use Authorization; FAERS, FDA Adverse Event Reporting System; FDA, US Food and Drug Administration; H3PO4, phosphoric acid; HCl, hydrochloric acid; HHS, US Department of Health and Human Services; LD50, the median lethal dose of a substance is the dose required to kill half the members of a tested population; MERS, middle east respiratory syndrome; mg/L, milligrams per liter; mmol/L, millimoles per liter; MMS, miracle mineral solution; NaClO2, sodium chlorite; ppm, parts per million; SARS, severe acute respiratory syndrome; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; T3, triiodothyronine; T4, thyroxine.INTRODUCTION
In December 2019, an outbreak of viral pneumonia occurred in Wuhan, China. The cause of these cases was determined to be a novel coronavirus related to other coronaviruses which previously caused outbreaks of Severe Acute Respiratory Syndrome [SARS] from 2002-2004 and Middle East Respiratory Syndrome [MERS] in 2012 (National Institutes of Health, 2020). This new coronavirus was named “severe acute respiratory syndrome coronavirus 2” [SARS-CoV-2] and the illness resulting from infection with this virus was termed Corona Virus Disease-19 or “COVID-19” (World Health Organization, 2020).
Although COVID-19 was initially viewed as a respiratory illness, subsequent investigations discovered this disease also can affect multiple other organ systems including cardiac, neurologic, renal, hepatic, gastrointestinal, and hematologic systems (Basilio, 2020; Rothan and Byrareddy, 2020).
Currently, the only US Food and Drug Administration [FDA] approved medication for COVID-19 in the US is remdesivir, an intravenous nucleotide prodrug of an adenosine analog. Remdesivir binds to the viral RNA- dependent RNA polymerase and inhibits viral replication through termination of RNA transcription (National Institutes of Health, 2021). This medicine has been shown to be superior to placebo in shortening the time to recovery in adults who were hospitalized with COVID-19 and had evidence of lower respiratory infection (Madsen, 2020). This medicine must be administered in a hospital or clinical setting capable of providing acute care comparable to inpatient hospital care.
Furthermore, only one vaccine has been approved to prevent COVID-19, although three vaccines have received emergency use authorization [EUA] from the FDA. The FDA issued EUAs on December 11, 2020 and December 18, 2020 for the Pfizer-BioNTech (FDA December 11, 2020) and Moderna (FDA, December 18, 2020) vaccines for the prevention of COVID-19 in the US. On February 27, 2021, the FDA issued an EUA for a third vaccine, Jansen [aka Johnson and Johnson] for the prevention of COVID-19 (FDA May 14, 2021).
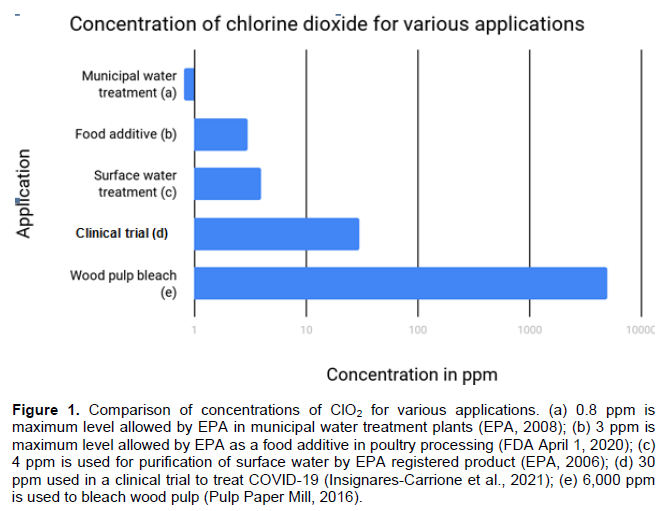
This situation has triggered a search for effective treatments and one potential treatment is chlorine dioxide [ClO2]. ClO2 is a simple molecule that is used for a wide variety of purposes including bleaching wood pulp (Pulp Paper Mill, 2016), purifying water (Calabrese et al., 1978), destroying microbes on food (FDA April 1, 2020), and sterilizing medical equipment (Rutala and Weber, 2008).
ClO2 is a strong oxidizing agent that rapidly and effectively destroys viruses (Alvarez and O’Brien, 1982; Junli et al., 1997; Ogata and Shibata, 2008; Sanekata et al., 2010; Wang et al., 2005) and based upon its potent virucidal activity, ClO2 has been suggested to help prevent the spread of coronavirus (Kály-Kullai et al., 2020). However, the use of ClO2 in humans has generated controversy due to the reported risks of this treatment, and the FDA has admonished people not to drink ClO2, describing it as “dangerous” and “bleach” (FDA August 12, 2019).
This raises the question, “Is chlorine dioxide a dangerous bleach, a safe water purifying agent, a food additive, a medical sterilant, or an effective treatment for COVID-19?”
METHODOLOGY
This is a narrative review exploring the potential benefits and risks of ClO2, as well as this molecule’s potential efficacy as a treatment for COVID-19. Thus, strict selection criteria were not applied for the selection of articles included in this manuscript. Rather, articles were chosen based upon how informative, comprehensive, and relevant they were to the theme of this article. Themes explored in this article include: Chemistry of ClO2, Historical uses of ClO2, Virucidal activity of ClO2, Safety of ClO2, Toxicity of ClO2, Efficacy of ClO2 as a treatment for COVID-19, and Controversies related to the use of ClO2.
Results of evidence-based research articles, government documents, and the first clinical trial utilizing ClO2 as a treatment for COVID-19 were reviewed for inclusion in this review.
RESULTS
Physical and chemical properties of ClO2 chemistry
Chlorine dioxide [ClO2] was first discovered by Sir Humphrey Davy in 1814 (Gray, 2014). ClO2 is a triatomic molecule consisting of one chlorine atom and two oxygen atoms (ChemicalSafetyFacts.org, 2020). ClO2 is a yellowish-green gas at standard conditions, but below 52°F. ClO2 is a liquid whereas above 52°F it turns into a gas (PubChem, 2018).
ClO2 is a very reactive compound. In the air, ClO2 is broken down quickly into chlorine gas and oxygen. In water, ClO2 undergoes photodecomposition to produce chlorate and chloride (Cl-) ions. ClO2 also undergoes decomposition under conditions of high temperature. These characteristics result in restriction of the storage and transportation of ClO2 (Department of Health and Human Services, 2004; Qi et al., 2020).
CIO2 gas is soluble in water and rapidly reacts with other compounds. Aqueous solutions of ClO2 have been reported to be stable at 25°C and a pH of 9 for a period of time before a rapid decomposition takes place and the concentration decreases. The stability of dissolved ClO2 depends on the pH and concentration of the solution (Medir and Giralt, 1982). The stability of ClO2 can be prolonged by incorporating it into a gel (Palcsó et al., 2019).
ClO2 can be synthesized from the reaction between NaClO2 [sodium chlorite] and an acid, such as hydrochloric acid [HCl] or phosphoric acid [H3PO4] (ChemicalSafetyFacts.org, 2020). ClO2 is highly soluble in water. When exposed to sunlight, it rapidly breaks down into chlorine gas and oxygen. In water, ClO2 quickly reacts to form chlorite ions (Department of Health and Human Services, 2004).
ClO2 has an odd number of electrons with 19 valence electrons. A single electron occupies the highest unoccupied molecular orbit, which renders the molecule a free radical and produces its reactive nature (Flesch et al., 2006). The single unpaired electron results in ClO2 being a strong oxidant, which allows it to accept an electron via oxidation-reduction reactions. This strong oxidizing potential has given rise to a wide variety of applications in a multitude of industries (Environmental Protection Agency, 2000).
Uses of chlorine dioxide
Products containing ClO2 are employed as bleach at high concentrations (Figure 1) (Pulp Paper Mill, 2016). The Environmental Protection Agency [EPA] first registered the aqueous form of ClO2 for use as a disinfectant and a sanitizer in 1967, and as a sterilant in 1988 (EPA, 2006). In May 2020, the EPA listed ClO2 as an approved hard surface disinfectant for use against SARS-CoV-2 (EPA, 2020).
ClO2 is also utilized as a water purifying agent. In Europe, this application began in the mid-19th century (Benarde et al., 1965). In the US, the EPA has approved ClO2 to purify drinking water (HHS, 2004). The Niagara Falls Water Treatment Plant in New York became the first municipal water treatment facility in the US to utilize ClO2 in 1944. In the 1950’s, ClO2 began replacing chlorine in water treatment plants because of its superior ability to reduce odors and unpleasant tastes in drinking water, along with its ability to destroy bacteria, viruses, and other harmful microorganisms without forming trihalomethanes, which are a byproduct of chlorine disinfection (HHS, 2004; Gray, 2014). Currently, ClO2 is used in about 5% of large water-treatment facilities in the US to purify water (Agency for Toxic Substances and Disease Registry, 2004; Gray, 2014). This includes over 500 public water treatment plants that use ClO2 full time and as many as 900 that use it either part time or seasonally (Ellenberger, 1999; Jonnalagadda and Nadupalli, 2014).
In addition to water purification, other applications for ClO2 include agricultural, commercial, medical, industrial, and residential uses. The agricultural industry utilizes ClO2 as a disinfectant of surfaces and equipment (EPA, 2006). The FDA has approved ClO2 for use by the food and beverage industries as a disinfectant and a bleaching agent for flour (FDA April 1, 2019; FDA April 21, 2019). A maximum concentration of 3 ppm is allowed when ClO2 is used as an antimicrobial agent in water used for poultry processing (FDA April 1, 2019) (Figure 1). The medical field uses ClO2 to sterilize equipment (EPA, 2006). Because ClO2 evaporates readily, it is present in both liquid and gas phase above the liquid, thus it may be able to reach microorganisms in areas that are otherwise difficult to reach. For use in the treatment of endodontic infections, it has been recommended that ClO2 be used in combination with other endodontic agents such as EDTA (Herczegh et al., 2019). The pulp, paper, and textile industries employ this product to remove colors (Jonnalagadda and Nadupalli, 2014). Residential uses include improving halitosis (Frascella et al., 2000; Loesche and Kazor, 2000) and controlling odors (Ogata and Shibata, 2009). Based on the fact that ClO2 evaporates readily, therefore it is present in both liquid and gas phase above the liquid, it may be able to reach the microorganisms in areas otherwise difficult to reach. Therefore, it is advised to use in combination with other endodontic agents which have soft tissue dissolving property such as NaOCl and smear layer and dentin removal capacity such as EDTA [Herczegh et al, 2019, https://doi.org/10.1016/j.jpba.2018.11.005].
The EPA has registered ClO2 as a pesticide [i.e. antimicrobial] due to its ability to eliminate microorganisms such as bacteria, viruses, and parasites from surface water, thereby rendering it safe to drink (EPA, 2006) (Figure 1). This application, at concentrations up to 4 ppm, is utilized by backpackers and emergency management personnel who obtain surface water from lakes or streams and purify it to create safe drinking water.
Based upon its safety, environmental friendliness, affordability, and ability to destroy a wide range of microorganisms, ClO2 has been termed the “ideal biocide” (Simpson et al., 1993) and a “universal antidote” (NASA, 1988).
Virucidal activity of chlorine dioxide
ClO2 acts as a potent, rapid virucide with activity against a wide range of viruses including Poliovirus, Adenovirus, Herpes simplex virus-1, Influenza virus, Measles virus, Mumps virus, and SARS-CoV (Alvarez and O’Brien, 1982; Junli et al., 1997; Ogata and Shibata, 2008; Sanekata et al., 2010; Wang et al., 2005). ClO2’s virucidal activity stems from its action as an oxidant (Wigginton et al., 2012). After coming in contact with a virus, chlorine dioxide rapidly oxidizes specific amino acids [primarily cysteine, tryptophan and tyrosine] in viral proteins, resulting in the loss of an electron from these amino acids (Fukayama et al., 1986). This redox reaction between ClO2 and the virus degrades the virus’s proteins, rendering it inactive and unable to infect host cells (Noss et al., 1986; Ogata, 2012; Wigginton et al., 2012).
Arguments for and against the use of chlorine dioxide to treat COVID-19
Arguments pertaining to the use of ClO2 to treat COVID-19 generally center around this compound’s safety, although questions of efficacy arise as well.
There are many ways to evaluate the safety of a product. One method involves assessing the adverse effects associated with the use of a product, and the second method is to examine the product’s lethality.
According to the EPA, oral ingestion of low doses of aqueous ClO2 in drinking water is not associated with significant adverse effects (EPA September, 2020). In fact, human studies have found no adverse effects in individuals who consume drinking water from municipal water treatment plants that use ClO2 as a disinfectant (Michael et al., 1981; Tuthill et al., 1982). Although one study (Kanitz et al., 1996) found an increased risk of several developmental effects in a community with drinking water that had been disinfected with ClO2, the EPA pointed out that this study suffers from numerous limitations that make it difficult to interpret the study’s findings (EPA September, 2020). The EPA has established a maximum limit for ClO2 of 0.8 mg/L [that is, 0.8 ppm] when used as a water purifying agent in municipal water treatment plants (Figure 1) (EPA, 2006). However, the EPA also approved a limit of 4 ppm for emergency drinking water, which involves disinfecting surface water in emergency situations (EPA April 29, 2020).
Similarly, no adverse effects have been found when low concentrations [0.04-0.15 mg/kg-day] of aqueous ClO2 are consumed in experimental studies. Short-term ingestion of ClO2 in a laboratory setting was assessed in two human studies by Lubbers et al. (1982) at the Ohio State University, College of Medicine. In the first study, a group of 10 healthy male adults drank two 500 mL portions of a ClO2 solution, 4 h apart. They drank the ClO2 solution every three days at steadily increasing concentrations, starting with 0.1 ppm and gradually increasing to 24.0 ppm (Lubbers et al., 1982). In the second study, a group of 10 adult males drank 500 mL of distilled water containing 5 ppm of ClO2 daily for 12 weeks. Neither study found any alterations in general health, vital signs, serum chemistry, hematologic parameters, or serum triiodothyronine [T3] or thyroxine [T4] (Lubbers et al., 1984).
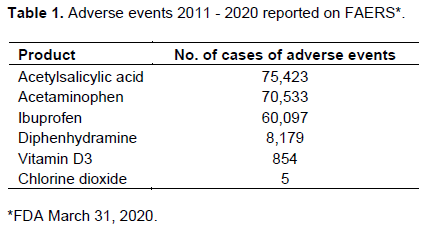
Although the ingestion of low doses of ClO2 is safe, high doses can be dangerous. As shown in Table 1, there have been 5 reports to the FDA Adverse Event Reporting System [FAERS] of adverse effects associated with the use of ClO2, and all 5 of these involved a product known as “Miracle Mineral Solution” or MMS.
MMS is a product that was developed by Jim Humble between 2001 and 2006. It is a solution of ~22 to 28% sodium chlorite in distilled water that its creator claimed can cure a wide range of maladies including malaria, HIV, autism, and cancer (FDA August 12, 2019; Humble, 2006). Although Humble strongly advocated the use of MMS for many years, he later retracted his claims, stating, “Today I say that MMS cures nothing!” (Galli et al., 2016).
The FDA has continued to warn against using MMS and similar products, stating “ingesting these products is the same as drinking bleach.” The FDA reports MMS “has caused serious and potentially life-threatening side effects” and describes reports of “severe vomiting, severe diarrhea, life-threatening low blood pressure caused by dehydration and acute liver failure after drinking these products” (FDA August 12, 2019).
Reports of adverse effects come from sources other than the FDA also. The Children’s Hospital of Philadelphia (2019) reported receiving 6 calls in 5 years related to MMS. The callers ranged in age from 3 to 48 years. One child experienced nausea and weakness following oral ingestion and the second experienced intestinal burns after being administered an enema that contained MMS.
Adverse effects were also described in a case report of a 41-year-old woman who developed Kikuchi-Fujimoto disease [histiocytic necrotizing lymphadenitis] after ingesting an unknown quantity of MMS in a glass of water that was given to her by a relative. She was admitted to a hospital 11 days after the onset of symptoms which included fever, left-sided lymphadenopathy, chills, rigors, and a dry cough. An excisional lymph node biopsy was performed, and histological findings were consistent with Kikuchi-Fujimoto disease. She was treated symptomatically with paracetamol 1 g every 6 h for 72 h and she defervesced 16 days after the initial onset of fever. Outpatient follow-up at 2 weeks found no recurrence of fever (Loh and Shafi, 2014).
Stories in the media have also described adverse effects and death in people who ingested MMS. Several news stories reported the case of a woman who was sailing with her husband in the south Pacific in August 2010 when she suddenly became ill after drinking MMS. This woman developed nausea, vomiting, diarrhea, abdominal pain, and felt faint, then lapsed into a coma and died (Galli et al., 2016; New Zealand Herald, 2016; Ono and Bartley, 2016). Autopsy results were inconclusive, however (Gibson, 2010).
A story in The New York Times reported the FDA had “received reports of at least 20 people affected by exposure to MMS, with at least seven deaths of people who had ingested Miracle Mineral Solution - two in 2018 and one each in 2017, 2014, 2013, 2011 and 2009” (Hauser, 2019). However, a review of the FDA’s Adverse Events Reporting System [FAERS] Public Dashboard indicates as of March 31, 2020, only 5 reports of adverse effects were received, one each in 2011, 2014, 2017, and no deaths were listed (FDA March 31, 2020).
High doses of ClO2 can cause adverse effects in formulations other than MMS. One of these adverse effects is methemoglobinemia. When ClO2 is added to water, chlorites are formed. High concentrations of chlorite ions oxidize hemoglobin to methemoglobin (Moore et al., 1978), and the ingestion of a high dose of ClO2 can result in methemoglobinemia. One example comes from the report of a 25-year-old male who ingested 10 g of sodium chlorite dissolved in 100 mL of water during a suicide attempt. He subsequently developed generalized cyanosis and respiratory distress and was found to be suffering from methemoglobinemia. He went on to develop an acute hemolytic crisis and disseminated intravascular coagulation. After being treated with continuous arterio-venous hemodialysis for 24 h, his methemoglobin decreased from 43.1 to 16.9%. However, he subsequently developed acute renal failure. Hemodialysis was continued for 4 weeks and after 3 months, renal function normalized (Lin and Lim, 1993). An important note is that individuals with glucose-6-phosphate deficiency [G-6-PD] may be at increased risk of forming methemoglobin following ingestion of ClO2 due to their reduced ability to detoxify hydrogen peroxide (Moore et al., 1978).
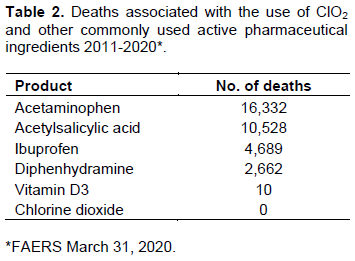
Another important factor when evaluating a product’s safety is lethality. One method of evaluating the lethality of a product is to track the number of deaths resulting from the use of the product. The risk of ingesting low doses of ClO2 has not been associated with any deaths. The HHS estimates as many as 12 million persons in the US consume ClO2 by drinking treated water (Department of Health and Human Services, 2004). Table 2 shows the number of deaths associated with the use of ClO2, as well as the number of deaths resulting from the use of other commonly used products, as reported to the FDA. The FDA lists no deaths resulting from the use of ClO2. Only 1 death was identified from a Google internet search. This involved the aforementioned case of the woman who died after ingesting MMS while sailing with her husband (Galli et al., 2016).
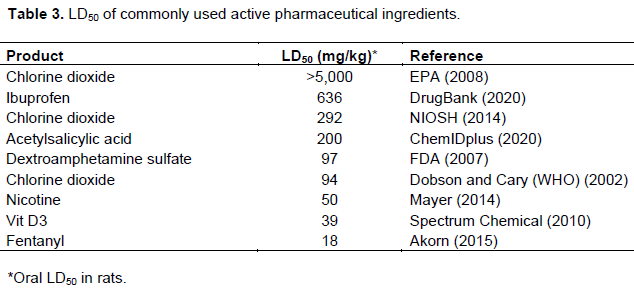
Another method for determining safety is to examine a product’s LD50. The LD50 of a substance is the dose required to kill half the members of a tested population. One commonly used test population is rats and the LD50 of ClO2 in rats, as well as commonly used over-the-counter products and prescription medicines, is listed in Table 3. The World Health Organization reported the LD50 for oral ClO2 as 94 mg/kg (Dobson and Cary, 2002), which falls between the LD50 of 50 mg/kg for nicotine (Mayer, 2014) and 97 mg/kg for dextroamphetamine (FDA, 2007). However, the National Institute for Occupational Safety and Health (NIOSH, 2014) reports the LD50 in rats as 292 mg/kg, which places it between aspirin and ibuprofen, and the US EPA (2008) lists the LD50 as >5,000 mg/kg.
Efficacy
ClO2 has been demonstrated to be an effective virucide, capable of rapidly and effectively eliminating a wide range of viruses both in vitro and in vivo (Junli et al., 1997; Ogata and Shibata, 2008; Sanekata et al., 2010; Wang et al., 2005). ClO2 has been demonstrated to destroy the SARS-CoV virus at a concentration of 2.19 mg/L in wastewater (Wang et al., 2005). Also, as previously noted, the EPA lists ClO2 as a disinfectant to destroy SARS-CoV-2 on hard surfaces (EPA June 17, 2020).
Ogata and Miura (2020) performed an in vitro experiment examining the effects of ClO2 on binding of the SARS-CoV-2 virus with angiotensin-converting enzyme 2 [ACE2], which is the primary receptor for the SARS-CoV-2 virus in the human body (Ali and Vijayan, 2020). The study found that treatment with 0.5 mmol/L ClO2 at room temperature for 5 min decreased binding to 1.9% of the control (Ogata and Miura, 2020). This suggests ClO2 might prevent binding of the SARS-CoV-2 virus to ACE2 in humans as well.
Insignares-Carrione et al. (2020) conducted a preliminary trial involving 104 patients in Ecuador utilizing ClO2 as a treatment for COVID-19. Patients in the trial were administered an aqueous solution of 30 ppm ClO2 in 1 L of water. This treatment was divided into 10 doses [that is, 100 ml each] and the doses were administered every hour and a half for 20 days. The investigators found that all symptoms of COVID-19 began to decrease on the first day of treatment and were significantly reduced by the 4th day of treatment.
An international multi-center study (Insignares-Carrione et al., 2021) was carried out from July 2020 through December 2020 involving 20 patients from Bolivia, Peru, and Ecuador. The treatment group [n=20] consisted of patients aged 18-80 years old, who tested positive for SARS-CoV-2 via RT-PCR and reported characteristic symptoms of COVID-19 [that is, fever, odynophagia, respiratory distress]. Exclusion criteria included COVID-19 RT-PCR negative, renal failure, congestive heart failure, and treatment with anticoagulants.
The treatment group received a loading dose of 1 L of water containing 30 ppm ClO2 that was drunk over a period of 2 h in 8 equally divided doses. Subsequently, patients in the treatment groups were administered 1 L of water containing 30 ppm ClO2 that was divided into 10 equal doses and was administered hourly. Treatment continued for 21 days.
The control group received anti-inflammatory treatment [ibuprofen at doses between 200 and 400 mg every 8 h], antibiotic [azithromycin 500 mg daily for 5 days], antihistamines [hydroxyzine 5 mg every 12 h], corticosteroids [methylprednisolone 40 mg every 12 h for 3 days, then 20 mg every 12 h for 3 days], and supportive measures.
The results of the study found a statistically significant reduction in symptoms in the treatment group compared with the control group. The authors recommended conducting randomized double-blind studies.
Another source of information regarding the possible efficacy of ClO2 against COVID-19 derives from statistics pertaining to cases and deaths from COVID-19 in Bolivia. In early August 2020, Bolivia approved ClO2 as a prevention and treatment for COVID-19. The number of cases of COVID-19 subsequently dropped 93% from August 20, 2020 to October 21, 2020 and daily deaths decreased 82% from a peak on September 3, 2020 to October 21, 2020. Although other factors may have played a role in the decline in cases and mortality during this time, the fact that cases and deaths dropped in Bolivia but not surrounding countries suggests ClO2 may have played a role in the progress seen in Bolivia (Insignares-Carrione et al., 2021).
DISCUSSION
This review finds that low concentrations of aqueous ClO2 are safe when ingested orally. Although reports of adverse effects and deaths associated with the use of ClO2 are rare in comparison to other commonly used products, these statistics may underestimate the risk of ingesting ClO2. The total number of cases of adverse effects and deaths is dependent upon the number of exposures, and the number of exposures may be much lower for ClO2 than for the other products listed. It has been estimated that 12 million people are exposed to ClO2 in drinking water (HHS, 2004), however this figure needs to be compared with the number of people who ingest acetaminophen, aspirin, and the other products listed in Tables 2 and 3 to obtain a more accurate assessment of the relative risk of ingesting these products.
Furthermore, the number of adverse effects and deaths listed by the FDA does not indicate the dose of the substances ingested. Dose is a critical factor in determining whether a therapeutic intervention functions as a treatment or a poison. While low doses of ClO2 do not cause adverse effects and are not lethal, high doses are associated with hematologic and renal complications. Also, while the LD50 of a substance is helpful in determining the relative safety or risk of a given treatment, the LD50 varies between species and therefore a lethal dose in rats may be different than the lethal dose in humans.
Despite uncertainty regarding the rate of adverse events and the need for studies exploring optimal dosing, data from initial human studies exploring low dose aqueous ClO2 as a treatment for COVID-19 suggest this agent reduces the severity of COVID-19 symptoms.
When examining the scientific rationale for determining whether or not to pursue a particular therapeutic intervention, it is important to assess the risk-benefit ratio. In the case of COVID-19, the biggest risk is death. The mortality ratio [that is, the number of reported deaths divided by the reported cases] for COVID-19 is currently estimated to be 2% and the total number of deaths resulting from COVID-19 worldwide currently exceeds 3.37 million as of May 21, 2021 (Johns, 2021).
The potential benefits of utilizing ClO2 include the destruction of the SARS-CoV-2 virus in the human body, the treatment of COVID-19 symptoms, and prevention of post-acute COVID-19 syndrome, or long-haulers syndrome. With the favorable aforementioned safety profile, it would appear that the beneifts of low dose aqueous ClO2 therapy far outweigh the risks.
CONCLUSION
Chlorine dioxide is a well-researched and widely used antimicrobial agent with strong virucidal activity. An examination of the scientific rationale for using aqueous ClO2 to treat COVID-19 suggests the key factor influencing the safety of this molecule is the dose. At low doses, ClO2 is safe and is not associated with adverse effects. However, at high doses it can cause hematologic and renal complications. As Parcelus aptly warned more than half a millennium ago: "Sola dosis facit venenum" or “the dose makes the poison.” As with warfarin, chemotherapeutic agents, and even aspirin, we must understand the safe therapeutic dosage range if we are to use a therapy effectively and avoid untoward events. This dictum applies to ClO2 as well.
Controlled, double blind studies examining the use of ClO2 as a prevention and treatment for COVID-19 are needed. A dispassionate assessment of the evidence-based risk-benefit ratio indicates a scientific rationale exists for the examination of ClO2 as a potential treatment for COVID-19. Hyperbolic press reports and alarmist statements that fail to discriminate between different formulations, concentrations, and doses of ClO2 only serve to increase confusion and impede scientific inquiry into the potential uses of this molecule as a therapeutic agent.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Agency for Toxic Substances and Disease Registry (September 2004). Toxicological profile: Chlorine dioxide and chlorite. |
|
|
Akorn (2015). SDS: Fentanyl Citrate Injection, USP CII. Safety Data Sheet. |
|
|
Ali A, Vijayan R (2020). Dynamics of the ACE2-SARS-CoV-2/SARS-CoV spike protein interface reveal unique mechanisms. Scientific Reports 10(1):1-12. |
|
|
Alvarez ME, O'Brien RT (1982). Mechanisms of inactivation of poliovirus by chlorine dioxide and iodine. Applied and Environmental Microbiology 44(5):1064-1071. |
|
|
Basilio P (2020). COVID-19: Damage found in multiple organ systems. MDLinx. |
|
|
Benarde MA, Israel BM, Olivieri VP, Granstrom ML (1965). Efficacy of chlorine dioxide as a bactericide. Applied Microbiology 13(5):776-780. |
|
|
Calabrese EJ, Moore GS, Tuthill RW (1978). The health effects of chlorine dioxide as a disinfectant in potable water: A literature survey. Journal of Environmental Health 41(1):26-31. |
|
|
ChemicalSafetyFacts.org. (2020). Chlorine dioxide. |
|
|
ChemIDplus (2020). Aspirin. |
|
|
Children's Hospital of Philadelphia (2019). Informatic: Bleach toxicity, with a focus on Miracle Mineral Solution (MMS). |
|
|
Department of Health and Human Services (2004). Toxicological profile for chlorine dioxide and chlorite. |
|
|
Dobson S, Cary R (2002). International Programme on Chemical Safety. Chlorine dioxide (gas). World Health Organization. |
|
|
DrugBank (2020). Ibuprofen. |
|
|
Ellenberger CS (1999). Water quality impacts of pure chlorine dioxide pretreatment at the Roanoke County (Virginia) water treatment plant (Doctoral dissertation, Virginia Tech). |
|
|
Environmental Protection Agency (2000). Toxicological review of chlorine dioxide and chlorite. |
|
|
Environmental Protection Agency (EPA) (2006). Reregistration eligibility decision (RED) for chlorine dioxide and sodium chlorite (Case 4023). |
|
|
Environmental Protection Agency (EPA) (2008). Acute Toxicity Review for EPA Reg. No.: 9150-11. |
|
|
Environmental Protection Agency (EPA) (2020). Emergency disinfection of drinking water. |
|
|
Environmental Protection Agency (EPA) (June 17, 2020). List N: Disinfectants for use against SARS-CoV-2 (COVID-19). |
|
|
Flesch R, Plenge J, Rühl E (2006). Core-level excitation and fragmentation of chlorine dioxide. International Journal of Mass Spectrometry 249:68-76. |
|
|
Food and Drug Administration (2007). Dexedrine. |
|
|
Food and Drug Administration (April 1, 2019). CFR - Code of Federal Regulations Title 21 - FDA. |
|
|
Food and Drug Administration (April 21, 2019). CFR - Code of Federal Regulations Title 21 - FDA. |
|
|
Food and Drug Administration (August 12, 2019). Danger: Don't drink Miracle Mineral Solution or similar products. |
|
|
Food and Drug Administration (March 31, 2020). FDA Adverse events reporting system (FAERS) public dashboard - Miracle Mineral Solution. |
|
|
Food and Drug Administration (April 1, 2020). CFR - Code of Federal Regulations Title 21 - FDA. |
|
|
Food and Drug Administration (December 11, 2020). FDA takes key action in fight against COVID-19 by issuing Emergency Use Authorization for first COVID-19 vaccine. |
|
|
Food and Drug Administration (December 18, 2020). FDA takes additional action in fight against COVID-19 by issuing Emergency Use Authorization for second COVID-19 vaccine. |
|
|
Food and Drug Administration (FDA)(2021). Janssen COVID-19 Vaccine. |
|
|
Frascella J, Gilbert RD, Fernandez P, Hendler J (2000). Efficacy of a chlorine dioxide-containing mouthrinse in oral malodor. Compendium of Continuing Education in Dentistry 21(3):241-244. |
|
|
Fukayama MY, Tan H, Wheeler WB, Wei CI (1986). Reactions of aqueous chlorine and chlorine dioxide with model food compounds. Environmental Health Perspectives 69:267-274. |
|
|
Galli C, Kreider R, Ross B, Ferran L (October 27, 2016). Husband says fringe church's 'miracle cure' killed his wife. ABC News. |
|
|
Galli C, Kreider R, Ross B (October 29, 2016). Fringe 'church' founder on MMS: It's no cure. ABC News. |
|
|
Gibson J. (2010). Death in paradise. The Sydney Morning Herald. |
|
|
Gray NF (2014). Chlorine dioxide. In Microbiology of Waterborne Diseases, 2nd ed, eds Percival SL, Yates MV, Williams DW, Chalmers RM, Gray NF. Academic Press, New York, pp. 591-598. |
|
|
Hauser C (August 13, 2019). Drinking bleach won't cure autism or cancer, F.D.A. says. The New York Times. |
|
|
Herczegh A, Barnabás P, Zsolt L, Romána Z (2019). Tracking of the degradation process of chlorhexidine digluconate and ethylenediaminetetraacetic acid in the presence of hyper-pure chlorine dioxide in endodontic disinfection. Journal of Pharmaceutical and Biomedical Analysis 164:360-364. |
|
|
Humble J (2006): Breakthrough: The Miracle Mineral Solution of the 21st Century, 4th ed. (Ebook). |
|
|
Insignares-Carrione E, Gómez BB, Kalcker AL (2020). Chlorine dioxide in COVID-19: Hypothesis about the possible mechanism of molecular action in SARS-CoV-2. Journal of Molecular and Genetic Medicine 14:5. |
|
|
Insignares-Carrione E, Blanca BG, Yohanny A, Patricia C, Maria SA, Martin ABAS, Gonzales CO (2021). Determination of the effectiveness of chlorine dioxide in the treatment of COVID 19. Journal of Molecular and Genetic Medicine 15:S1. |
|
|
Johns H (May 21, 2020). COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://coronavirus.jhu.edu/map.htmL |
|
|
Jonnalagadda SB, Nadupalli S (2014). Chlorine dioxide for bleaching, industrial applications and water treatment. Indian Chemical Engineer 56(2):123-136. |
|
|
Junli H, Li W, Nenqi R, Li LX, Fun SR, Guanle Y (1997). Disinfection effect of chlorine dioxide on viruses, algae and animal planktons in water. Water Research 31(3):455-460. |
|
|
Kály-Kullai K, Wittmann M, Noszticzius Z, Rosivall L (2020). Can chlorine dioxide prevent the spreading of coronavirus or other viral infections? Physiology International 107(1):1-11. |
|
|
Kanitz S, Franco Y, Patrone V, Caltabellotta M, Raffo E, Riggi C, Timitilli D, Ravera G (1996). Association between drinking water disinfection and somatic parameters at birth. Environmental Health Perspectives 104(5):516-520. |
|
|
Lin JL, Lim PS (1993). Acute sodium chlorite poisoning associated with renal failure. Renal Failure 15(5):645-648. |
|
|
Loesche WJ, Kazor C (2000). Microbiology and treatment of halitosis. Periodontology 28(1):256-279. |
|
|
Loh JM, Shafi H (2014). Kikuchi-Fujimoto disease presenting after consumption of 'Miracle Mineral Solution'(sodium chlorite). BMJ Case Reports bcr2014205832. |
|
|
Lubbers JR, Chauan S, Bianchine JR (1982). Controlled clinical evaluations of chlorine dioxide, chlorite and chlorate in man. Environmental Health Perspectives 46:57-62. |
|
|
Lubbers JR, Chauhan S, Miller JK, Bianchine JR (1984). The effects of chronic administration of chlorite to glucose-6-phosphate dehydrogenase deficient health adult male volunteers. Journal of Environmental Pathology, Toxicology, and Oncology 5:239-242. |
|
|
Madsen LW (2020). Remdesivir for the Treatment of Covid-19-Final Report. The New England Journal of Medicine 338(19):1813-1826. |
|
|
Mayer B (2014). How much nicotine kills a human? Tracing back the generally accepted lethal dose to dubious self-experiments in the nineteenth century. Archives of Toxicology 88(1):5-7. |
|
|
Medir M, Giralt F (1982). Stability of chlorine dioxide in aqueous solution. Water Research 16(9):1379-82. |
|
|
Michael GE, Miday RK, Bercz JP, Miller RG, Greathouse DG, Kraemer DF, Lucas JB (1981). Chlorine dioxide water disinfection: A prospective epidemiology study. Archives of Environmental Health 36(1):20-27. |
|
|
Moore GS, Calabrese EJ, DiNardi SR, Tuthill RW (1978). Potential health effects of chlorine dioxide as a disinfectant in potable water supplies. Medical Hypotheses 4(5):481-496. |
|
|
NASA (1988). A universal antidote. |
|
|
National Institute for Occupational Safety and Health (NIOSH) (2014). Chlorine dioxide. |
|
|
National Institutes of Health (March 3, 2020). Novel coronavirus structure reveals targets for vaccines and treatments. |
|
|
National Institutes of Health (April 21, 2021). Remdesivir. |
|
|
New Zealand Herald (2016). Man left devastated after wife dies 12 hours after 'drinking miracle remedy.' |
|
|
Noss CI, Hauchman FS, Olivieri VP (1986). Chlorine dioxide reactivity with proteins. Water Research 20(3):351-356. |
|
|
Ogata N (2012). Inactivation of influenza virus haemagglutinin by chlorine dioxide: oxidation of the conserved tryptophan 153 residue in the receptor-binding site. Journal of General Virology 93(12):2558-2563. |
|
|
Ogata N, Miura T (2020). Inhibition of the binding of spike protein of SARS-CoV-2 coronavirus to human angiotensin-converting enzyme 2 by chlorine dioxide. Annals of Pharmacology and Pharmaceutics 5(5):1195. |
|
|
Ogata N, Shibata T (2008). Protective effect of low-concentration chlorine dioxide gas against influenza A virus infection. Journal of General Virology 89(1):60-67. |
|
|
Ogata N, Shibata T (2009). Effect of chlorine dioxide gas of extremely low concentration on absenteeism of schoolchildren. International Journal of Medicine and Medical Science 1:288-289. |
|
|
Ono D, Bartley L (2016). Eyewitness News investigates unorthodox underworld of Genesis II Church. ABC7news. |
|
|
Palcsó B, Moldován Z, Süvegh K, Herczegh A, Zelkó R (2019). Chlorine dioxide-loaded poly (acrylic acid) gels for prolonged antimicrobial effect. Materials Science and Engineering: C(98):782-8. |
|
|
Pulp Paper Mill (2016). Chlorine dioxide bleaching. |
|
|
PubChem (2018). Chlorine dioxide. |
|
|
Qi M, Huang L, Xu X, Yi T, Xu H, Zhao H, Huang C, Wang S, Liu Y (2020). Synthesis of chlorine dioxide stable solution by combined reduction and its decomposition kinetics. Nordic Pulp & Paper Research Journal 35(3):342-352. |
|
|
Rothan HA, Byrareddy SN (2020). The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. Journal of Autoimmunity 109:102433. |
|
|
Rutala WA, Weber, DJ (2008). Guideline for disinfection and sterilization in healthcare facilities. Centers for Disease Control. |
|
|
Sanekata T, Fukuda T, Miura T, Morino H, Lee C, Maeda K, Araki K, Otake T, Kawahata T, Shibata T (2010). Evaluation of the antiviral activity of chlorine dioxide and sodium hypochlorite against feline calicivirus, human influenza virus, measles virus, canine distemper virus, human herpesvirus, human adenovirus, canine adenovirus and canine parvovirus. Biocontrol Science 15(2):45-49. |
|
|
Simpson GD, Miller RF, Laxton GD, Clements WR (1993). A focus on chlorine dioxide: The "ideal" biocide. In: Corrosion-National Association of Corrosion Engineers Annual Conference. |
|
|
Spectrum Chemical (June 2, 2010). Cholecalciferol material safety data sheet. |
|
|
Tuthill RW, Giusti RA, Moore GS, Calabrese EJ (1982). Health effects among newborns after prenatal exposure to ClO2-disinfected drinking water. Environmental Health Perspectives 46:39-45. |
|
|
Wang XW, Li JS, Jin M, Zhen B, Kong QX, Song N, Xiao WJ, Yin J, Wei W, Wang GJ, Si BY (2005). Study on the resistance of severe acute respiratory syndrome-associated coronavirus. Journal of Virological Methods 126(1-2):171-177. |
|
|
Wigginton KR, Pecson BM, Sigstam T, Bosshard F, Kohn T (2012). Virus inactivation mechanisms: impact of disinfectants on virus function and structural integrity. Environmental Science & Technology 46(21):12069-12078. |
|
|
World Health Organization (WHO) (2020). Naming the coronavirus disease (COVID-19) and the virus that causes it. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


