Full Length Research Paper

ABSTRACT
Bacteraemia is a common cause of morbidity and mortality in children worldwide. Therefore, bacteraemia continues to be increasingly a serious health problem that needs an immediate attention and treatment. A retrospective hospital-based study was conducted on positive blood cultures collected from 804 children (aged less than 10 years) including both genders in a period between 2012 and 2013 in three different medical services center in Khartoum state, Sudan, out of 804 tested blood samples, among whom 226 isolates were recovered from blood cultures. The majority of the children with bacteraemia (77.4%) were found to be less than one year old (49.1% male and 50.9% female). The most frequent pathogen was found to be Staphylococcus aureus (33.6%), followed by Klebsiella pneumoniae. (30.5%), Pseudomonas aeruginosa (11.5%), Burkholderia cepacia (10.6%), Streptococcus spp., (7%), Escherichia coli (3.5%), Acinetobacter spp. (1.7%) and coagulase negative staphylococci (1.3%). This study shows the highest susceptibility rate of S. aureus to vancomycin (97.3%), and the lowest susceptibility rate (34.7%) was recorded for erythromycin. Staphylococcus aureus was the main etiological agent of bacteraemia in children, while the most isolates demonstrating susceptibility to vancomycin. Overall, erythromycin resistance was 65.3%. This information should be considered when empirical therapy is recommended for the treatment of children with bacteraemia. Most laboratories in Sudan use a single aerobic blood culture bottle for routine blood culture. So our recommendation is using aerobic in conjugation with anaerobic bottles in order to recover significantly more organisms.
Key words: Bacteraemia, children, antimicrobials, drug resistance, Sudan.
INTRODUCTION
Bacteraemia is a common cause of morbidity and mortality in children (Reimer et al., 1997) worldwide (Dawodu et al., 1997; Stoll et al., 1998; Bhutta and Yusuf, 1997; Orrett and Shurland, 2001). Therefore, bacteraemia continues to be a serious problem that needs immediate attention and treatment. For an accurate diagnosis and an appropriate choice of antimicrobials, blood culture, which usually takes a few days, is required. The empirical choice of antimicrobials for the treatment of bacteraemia is guided by an awareness of previous culture reports (Cisterna et al., 2001). The majority of the bacteraemia cases are caused by number of pathogens including Staphylococcus spp., Streptococcus spp., Enterobacter spp., Escherichia coli, Klebsiella pneumoniae and Pseudomonas spp. (Reimer et al., 1997). In a prospective five-year study on 344 clinically significant episodes of pediatric septicemia, the most common organisms were found to be Salmonella spp. (15.0%), ensuing by methicillin-resistant S. aureus. They have reported that Haemophilus influenzae accounted for 2.0% of all episodes (Cheng et al., 1991). Furthermore, another study has reported that among 408 bacterial strains, Salmonella spp. were the most commonly isolated (23%), followed by S. aureus and Acinetobacter moraxella (Gedebou et al., 1984). The most frequent etiologic agents of bacteraemia cases include Staphylococcus spp., Streptococcus spp., Enterobacter spp., E. coli, K. pneumoniae and Pseudomonas spp. (Reimer et al., 1997; Cisterna et al., 2001). We have conducted this study to facilitate the empiric treatment and management of children with bacteraemia. The purpose of this study is to determine the causative agents that accounts for bacteraemia among Sudanese children ≤ 10 years old and to assess their susceptibility to various groups of antimicrobial agents.
MATERIALS AND METHODS
A descriptive retrospective hospital based study was conducted on positive blood cultures taken from 804 children (aged less than 10 years) regardless of their genders, in a period between December, 2012 and December, 2013 in three different urban medical services center in Khartoum state including Soba University Hospital, Saed Abo Ella hospital and Ibrahim Malik hospital. Eligible patients had an axillary temperature of less than 39°C and a white blood cell (WBC) count of less than 5000/mm3 or less than 15,000/mm3. Exclusion criteria were a clearly identifiable infection apparent on physical examination (for example pneumonia, urinary tract infection, meningitis, osteomyelitis, septic arthritis), immunisation within the preceding 48 h and treatment with antibiotics within the preceding 7 days).
The selection include in-patients and out-patients. Patients with the clinical suspicion to suffer from bacteraemia were included if blood culture analysis was requested by the responsible physician. Patients older than 10 years and patients with unavailable laboratory parameter results were excluded. Patients with a potential blood culture contaminant and those with missing or inaccurate identification to the species level were excluded from further analysis. Sampling process, culturing, bacterial identification and susceptibility testing for antimicrobials were as follows: the blood specimens had been taken for culture after sterilizing the skin with 70% alcohol and then with 10% povidone iodine solution. One to three milliliters venous blood was taken from the patient and inoculated into an aerobic blood culture bottle that contained 50 ml of Tryptose phosphate broth and 0.02% polyanethol sulfonate (liquid). All cultures were checked daily for cloudiness, haemolysis, and gas production. Sepsis was defined according to the recommendations of Bone et al. (1992).
Organisms were identified via standard microbiological techniques; culture was incubated at 37°C for 24 h prior to the isolation and identification of the bacteria. Based on the Gram-staining, characteristics of the bacterial growth in the blood culture bottle was sub-cultured onto MacConkey agar, chocolate blood agar, and blood agar plates. Bacteria which have been isolated from colonies were further characterized by special biochemical methods; analytical profile index (API 20E) was used for gram negative bacilli, and susceptibility testing was evaluated using the disc diffusion methods according to the guidelines of the National Committee for Clinical Laboratory Standards (NCCLS) (Standards NCfCL (2007). The following antibiotics and concentrations (in brackets) were used: amikacin (30 μg), ampicillin (10 μg), amoxicillin–clavulanic acid (AMC) (20/10 μg), cefotaxime (30 μg), tetracycline (30 μg), erythromycin (15 μg), cefuroxime (30 μg), meropenem (10 μg), ceftriaxone (30 μg), ceftazidime (30 μg), vancomycin (30 μg), gentamicin (10 μg), ciprofloxacin (5 μg), co-trimoxazole (trimethoprim–sulfamethoxazole) (1.25/23.75 μg), cephalexin (30 μg), cefazolin (30 μg), clindamycin (2 μg) and oxacillin (1 μg).
The data were collected from the clinical microbiology laboratory records which was filled in a prepared data sheet and included micro-organisms isolated from blood culture and antibacterial susceptibility data. The hospitals were informed for the purpose of the study and its objectives, before taking their permission, with protections of their records. Permission to carry out the study was taken from the Scientific Research Committee, Khartoum University. Minimum inhibitory concentrations (MICs) were done according to NCCLS guidance and interpretative criteria (2001). Statistical analysis was done using the Chi-squared test. Staphylococcus aureus (ATCC 25923), Pseudomonas aeruginosa (ATCC 49189) and one of Escherichia coli (ATCC 25922), were included to establish the validity of the experiment.
RESULTS
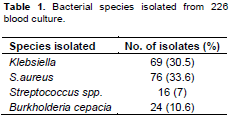
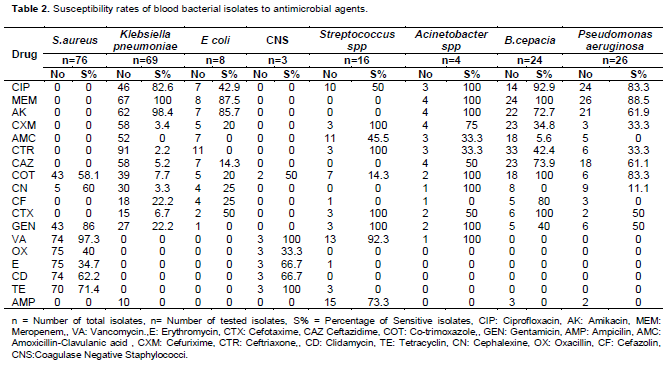
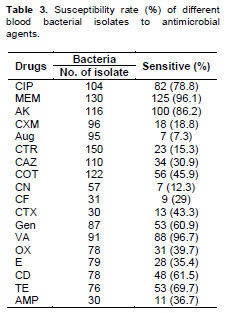
During the study period (2012 to 2013), a total of 226 out of 804 blood samples of selected children less than 10 years of age (49.1% male and 50.9% female) which gave a positive blood culture was analyzed. No significant difference showed between male and female inflicted with bacteraemia. Results have shown that most of bacteraemia cases (77.4%) were observed among children less than 12 months old, among whom (65.9%) were less than one month old. Only (17.3%) were observed in children aged between 3 to 10 years. There is a significant increase of bacteraemia in children aged one year or less (P = 0.001). The majority of the isolated pathogens were S. aureus (33.6%), followed by Klebsiella spp. (30.5%), Pseudomonas spp. (11.5%), Burkholderia cepacia (10.6%), Streptococcus spp. (7%), E. coli (3.5%), Acinetobacter spp. (1.7%) and coagulase negative staphylococci (1.3%) (Table 1). The antimicrobial susceptibility of bacteraemia isolates for 18 selected antimicrobial agents used in this study are summarized in Table 2. The highest susceptibility rate of S. aureus was to vancomycin (97.3%), whereas the lowest susceptibility rate was to erythromycin (34.7%). The highest susceptibility rates of other isolates to meropenem were Klebsiella spp. (100%), Acinetobacter spp. (100%), Burkholderia cepacia (100%), E. coli (87.5%) and Pseudomonas spp. (88.5%). However, vancomycin was detected to give the highest susceptibility rate of 96.7% to a variety of bacteraemia isolates; amoxicillin plus clavulanic acid have exhibited the lowest susceptibility rate of 7.3% (Table 3).
DISCUSSION
Blood for culturing is a routine procedure for investigating the cause of suspected infection in the majority of patients attending an emergency department(unit). Isolation of a true pathogen from blood culture ultimately warrants and augur well treatment with an appropriate antibiotic. This study provides information regarding the main etiological agents that cause bacteraemia in children of both inpatients and outpatient and its antimicrobial susceptibility patterns. S. aureus was reported to have emerged as a major cause (33.6%). These results are in accordance with other studies that have pointed out S. aureus as the most common bacteria isolated from blood of children (Nimri and Batchoun, 2004; Mohammad, 2010). The second most common organism causing bacteraemia in this study was Klebsiella spp. (30.5%). Similar results were reported in Jordan (Standards NCfCL, 2001). In another studies conducted elsewhere, E. coli was the most common organism (70%) (Berkley et al., 2005). In this study, the occurrence of Pseudomonas spp. Streptococcus spp. E. coli and Acinetobacter spp. were 11.5, 7, 3.5 and 1.7%, respectively. Different occurrence of these blood isolates were reported in different exhaustive literature (Mohammad, 2010; Joshi et al., 2000). Nonetheless, Pseudomonas spp. was the most common cause of neonatal sepsis in Karachi, Pakistan (Bhutta and Yusuf, 1997).
Burkholderia cepacia has the potential to cause fatal infections in hospital, and multidrug resistance makes them a serious threat in hospital settings. B. cepacia has been reported from blood stream infections (Aaron et al., 2000). In this study, B. cepacia reported for 10.6%. Coagulase negative Staphylococci encountered for 1.3%. Other studies reported coagulase negative staphylococci as the most common bacteria isolated from infant with bacteraemia (Sabui et al., 1999). The most effective antimicrobial agent against S. aureus which has been demonstrated in this study was vancomycin (97.3%), followed by gentamicin (86%). Similar results for vancomycin were reported in Jordan (Mohammad, 2010; El-Nasser, 2009). However, another author reported high susceptibility rates of S. aureus, reaching 59.5% to gentamicin (Blomberg et al., 2007). From our study we observed resistance rate of S. aureus to erythromycin (65.3%) which was higher than documented resistance rate of 33.1% conducted elsewhere (Delialioglu et al., 2005). However, the highest susceptibility rate (100%) to meropenem observed in this study was for Klebsiella. Similar results have been reported in the literature (Endtz et al., 1997). Whereas the highest resistance rate (100%) to ampicillin observed in this study was for Klebsiella, similarly low susceptibility rate (0%) of Klebsiella to ampicillin has been reported in Jordan (Mohammad, 2010).
CONCLUSION AND RECOMMENDATION
Our study shows that S. aureus is the main causative agent of bacteraemia in children. Treatment of bacteraemia is compromised by antimicrobial resistance. Accordingly, this study is important in order to facilitate the empirical treatment of children with bacteraemia. Most laboratories in Sudan use a single aerobic blood culture bottle for routine blood culture. So our recommendation is using aerobic in conjugation with anaerobic bottles in order to recover significantly more organisms. Further studies are needed to help authorities to formulate antimicrobial prescription policies.
CONFLICT OF INTEREST
Authors have none to declare.
ACKNOWLEDGEMENTS
We thank all the participants in this study for generously helping us in this research.
REFERENCES
|
Aaron SD, Ferris W, Henry DA, Speert DP, Macdonald NE (2000). Multiple combination bactericidal antibiotic testing for patients with cystic fibrosis infected with Burkholderia cepacia. Am. J. Respir. Crit. Care Med. 161(4 Pt 1):1206-12. Crossref |
||||
|
Berkley JA, Lowe BS, Mwangi I, Williams T, Bauni E, Mwarumba S, Ngetsa C, Slack MP, Njenga S, Hart CA, Maitland K, English M, Marsh K, Scott JA (2005). Bacteremia among children admitted to a rural hospital in Kenya. New Engl. J. Med. 352(1):39-47. Crossref |
||||
|
Bhutta ZA, Yusuf K (1997). Neonatal sepsis in Karachi: factors determining outcome and mortality. J. Trop. Pediatr. 43(2):65-70. Crossref |
||||
|
Blomberg B, Manji KP, Urassa WK, Tamim BS, Mwakagile DS, Jureen R, Msangi V, Tellevik MG, Holberg-Petersen M, Harthug S, Maselle SY, Langeland N (2007). Antimicrobial resistance predicts death in Tanzanian children with bloodstream infections: a prospective cohort study. BMC Infect. Dis. 7:43. Crossref |
||||
|
Bone RC, Sprung CL, Sibbald WJ (1992). Definitions for sepsis and organ failure. Crit. Care Med. 20(6):724-6. Crossref |
||||
|
Cheng AF, Fok TF, Duthie R, French GL (1991). A five-year prospective study of septicaemia in hospitalized children in Hong Kong. J. Trop. Med. Hyg. 94(5):295-303. Pubmed |
||||
| Cisterna R CV, Gomez E, Busto C, Atutxa I, Ezpeleta C (2001). Community-acquired bacteraemia. Spanish J. Chemother. 14:369-82. | ||||
|
Dawodu A, al Umran K, Twum-Danso K (1997). A case control study of neonatal sepsis: experience from Saudi Arabia. J. Trop. Pediatr. 43(2):84-8. Crossref |
||||
|
Delialioglu N, Aslan G, Ozturk C, Baki V, Sen S, Emekdas G (2005). Inducible clindamycin resistance in staphylococci isolated from clinical samples. Jpn J. infect. Dis. 58(2):104-6 Pubmed |
||||
| El-Nasser ZAF (2009). Prevalence and pattern of antimicrobial susceptibility of methicillin-resistant and methicillin-sensetive staphylococcus aureus in north Jordan. Jordan Med. J. 43:15-20. | ||||
|
Endtz HP, van Dijk WC, Verbrugh HA (1997). Comparative in-vitro activity of meropenem against selected pathogens from hospitalized patients in The Netherlands. MASTIN Study Group. J. Antimicrob. Chemother. 39(2):149-56. Crossref |
||||
|
Gedebou M, Tassew A, Azene G (1984). Blood culture isolates from an Addis Ababa hospital. Frequency and antibiotic sensitivities. East Afr. Med. J. 61(3):190-6. PMid:6479073 |
||||
|
Joshi SG, Ghole VS, Niphadkar KB (2000). Neonatal gram-negative bacteremia. Indian J. Pediatr. 67(1):27-32. Crossref |
||||
|
Mohammad A (2010). Bacteremia among Jordanian children at Princess Rahmah Hospital: Pathogens and antimicrobial susceptibility patterns. Iran. J. Microbiol. 2(1):22-6. Pubmed |
||||
|
Nimri LF, Batchoun R (2004). Community-acquired bacteraemia in a rural area: predominant bacterial species and antibiotic resistance. J. Med. Microbiol. 53(Pt 10):1045-9. Crossref |
||||
|
Orrett FA, Shurland SM (2001). Neonatal sepsis and mortality in a regional hospital in Trinidad: aetiology and risk factors. Ann. Trop. Paediatr. 21(1):20-5. Crossref |
||||
|
Reimer LG, Wilson ML, Weinstein MP (1997). Update on detection of bacteremia and fungemia. Clin. Microbiol. Rev. 10(3):444-65. Pubmed |
||||
|
Sabui T, Tudehope DI, Tilse M (1999). Clinical significance of quantitative blood cultures in newborn infants. J. Paediatr. Child Health 35(6):578-81. Crossref |
||||
|
Standards NCfCL (2001). Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically. Approved standards. In: NCCLS, editor. Pa, USA: Wayne. Standards NCfCL (2007). Performance standards for antimicrobial susceptibility tests. Approved standards. In: NCCLS, editor. 7th ed PA, USA: Wayne. p 10. |
||||
Stoll BJ, Holman RC, Schuchat A (1998). Decline in sepsis-associated neonatal and infant deaths in the United States, 1979 through 1994. Pediatrics 102(2):e18.
Crossref
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


