Full Length Research Paper

ABSTRACT
Local production of hand hygiene products result in increased availability and compliance with hand hygiene in healthcare settings and significant cost saving to hospitals if effective and acceptable. The aim of this study was to compare the effectiveness, acceptability, and cost benefit of a locally produced hand sanitizer to commercial hand sanitizer products. This was a comparative cross sectional study carried out among students of the Faculty of Clinical Sciences, University of Uyo in July 2019. Three hand sanitizer products, one locally produced and two commercial hand sanitizer products were compared. Bacterial growth from swabs from the hands of sixty students collected before and after use of one of the three hand sanitizer products were compared to determine bacterial reduction. Participants also assessed the products by scoring the product on a questionnaire using a five-point scale. The cost per litre of hand sanitizer products was calculated and compared. The mean percentage reduction of bacterial colony-forming units (CFU) was highest for the locally produced hand sanitizer product. There was no significant difference between acceptability of products for the criteria assessed except colour for which the local product had higher acceptability score than other products. The locally produced hand sanitizer was much cheaper than the commercially products. The in-house produced hand sanitizer product provides higher bacterial reduction than commercial products, has good acceptability among users and provides significant cost savings to the hospital.
Key words: Hand sanitizer, hand hygiene, Nigeria, production.
INTRODUCTION
Hand hygiene is a general term referring to any action of hand cleansing (Nabavi et al., 2015). It has been long established that hospital acquired infections are transmitted by the hands of healthcare workers. Hand hygiene is an important component of the infection control “bundles” which have proven efficacy for the prevention of catheter-related infections, ventilator- associated pneumonias, and urinary catheter sepsis and is also associated with significant reductions in diarrhoea and respiratory illnesses (Godfrey and Schouten, 2014).
Although there is paucity of data on the burden of healthcare associated infections in Nigeria, it is clear that this is significant due to widespread nonexistence of basic infection control measures, understaffing, poor hygiene and sanitation, lack or shortage of basic equipment associated with low income countries (Nejad et al., 2011; World Health Organization, 2009). There are two main methods of hand hygiene: hand washing with soap and water and use of alcohol-based hand rub. Studies on the effectiveness of alcohol-based solutions for hand hygiene showed that alcohol-based hand rubs remove organisms more effectively, require less time, and irritate skin less often than hand washing with soap or other antiseptic agents and water (World Health Organization, 2009; Gupta et al., 2007). Introduction of alcohol-based hand rub in hospitals have been shown in studies around the world to lead to a sustained increase in healthcare workers’ compliance with hand hygiene (Pittet et al., 2004; Grayson et al., 2008).
In many low-income countries where access to hand washing facilities is limited due to infrastructural realities and where water sources are unreliable or insufficient, alcohol-based hand sanitizer offers a viable alternative. Evidences show that the introduction of alcohol-based hand sanitizer is associated with a higher hand-hygiene compliance rate (Budd et al., 2016; Erasmus et al., 2010). Improvements in hand hygiene compliance significantly reduce the transmission of pathogens in healthcare settings (World Health Organization, 2009). Following the introduction of an in-house produced alcohol hand rub in our hospital, this study was conducted to compare the effectiveness, acceptability, and cost benefit of a locally produced hand sanitizer to commercial hand sanitizer products.
MATERIALS AND METHODS
A quasi-experimental approach was used for this study. It was carried out among students of the Faculty of Clinical Sciences, University of Uyo in July 2019. Sixty medical students were selected from a class of 96 by consecutive recruitment of consenting students until the required sample was filled. Each student was randomly assigned to one hand sanitizer product by balloting and 3-4 ml of the selected sanitizer was used to disinfect their hands. Five minutes after, another swab was taken from their right hands.
Chemical composition of hand sanitizer products
Three hand sanitizers were evaluated; an in-house produced hand sanitizer designated ‘A’; a Nigeria made commercial hand sanitizer designated ‘B’; and a foreign produced commercial hand sanitizer designated ‘C’. Product ‘A’ was constituted based on WHO guide for local production and contained 80% ethanol as the active ingredient, glycerol, hydrogen peroxide, colourant, perfume, and carbomer thickener. Product ‘B’ contained 70% ethanol as the active ingredient with triethalonamine, propylene glycol, and carbomer. Product ‘C’ contained 62% ethanol as the active ingredient with isopropyl alcohol, glycerine, isopropyl myristate, propylene glycol, tocopheryl acetate, aminoethyl propranolol, and carbomer.
Antibacterial efficacy of hand sanitizers
Students without any prior instruction on the use of hand sanitizers were instructed to contaminate their hands by carrying out their normal daily activities. A swab was taken from the right hand of each student by rolling a swab stick moistened with Brain Heart Infusion (BHI) broth over their right hand palm and fingertips to provide a baseline for the testing. Each participant was asked to use 3ml of hand sanitizer to clean their hands. Another sterile swab stick moistened with sterile BHI broth was rolled over the right hand palm and fingertips of participants after using hand sanitizer and thereafter spread over a blood agar plate (Oxoid, UK) which was incubated aerobically overnight at 36°C. The number of colonies growing on each plate was counted and the mean number of colonies for participants using each hand sanitizer was calculated.
Acceptability perception
Each participant was asked to assess the hand sanitizer product used by scoring the product on a questionnaire using a five-point scale (from abnormal to normal) to rate colour (unpleasant/ pleasant), smell (unpleasant/pleasant), texture (sticky/not sticky), irritation (irritating/not irritating), drying (very much/not at all), ease of use (difficult/easy), speed of drying (slow/fast), and application (unpleasant/pleasant).
Cost analysis
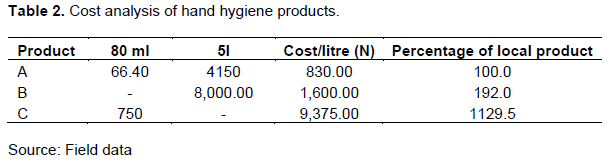
The cost per litre of the locally produced hand sanitizer was calculated by dividing the total cost of materials for production of one batch of sanitizer by number of litres produced while the cost of commercial hand sanitizer products was calculated by dividing the shelf price of a unit of product by the number of litres per unit of each product.
Data analysis
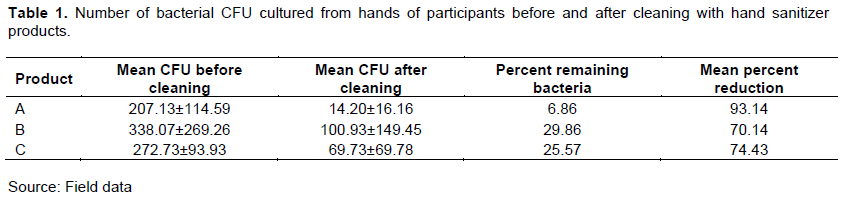
The percentage remaining bacteria was calculated by expressing the mean CFU after use as a percentage of the mean colony-forming units (CFU) before use of each handrub product.

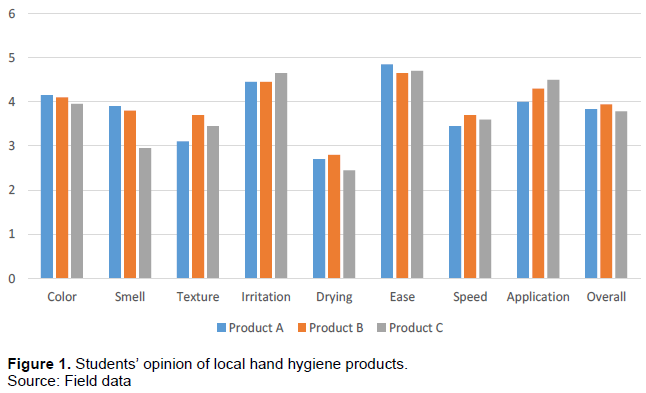
The acceptability perception scores given by each student for each criterion were added and the average score for each product was used to create a bar chart. ANOVA was used to test the difference between acceptability of products by criteria. Data analysis was carried out on Microsoft Excel and SPSS software.
Ethics
Participation in this study was voluntary and all participants gave informed consent to their inclusion in the study.
RESULTS
Antibacterial efficacy of hand sanitizers
There was no statistically significant difference between mean number of bacterial CFU on the hands of participants using the locally produced sanitizer and participants using other products. The mean bacterial loads on the hands of participants using each product before and after hand cleaning and the mean percentage reduction of bacterial CFU are shown in Table 1. The locally produced hand sanitizer had a significantly higher percentage reduction of CFU than the other products tested.
Acceptability of products
This is shown in Figures 1. Product A had highest average score for colour, smell and ease of use and lowest for texture, speed and application. There was no significant difference between products across the criteria except for colour.
Cost analysis
This is shown in Table 2. The unit cost of the commercial products were higher than the locally produced hand sanitizer by 192 and 1129% for products ‘B’ and ‘C’ respectively.
DISCUSSION
In line with its recommendation of use of alcohol-based hand rub for routine hand hygiene, the WHO published a guide for the local production of WHO-recommended hand rubs. These formulations are based on ethanol or isopropyl alcohol at final concentrations of 80 and 75%, respectively. Our product was based on this guide using ethanol as the active ingredient. This product also contains a carbomer thickening agent in addition to the recommended glycerol and hydrogen peroxide as humectant and for inactivation of bacterial spores in the solution respectively.
User acceptance is one of the most important criteria for selection of alcohol-based hand rub (Wolfensberger et al., 2015; Pittet et al., 2009). The acceptability of our product was comparable to that of the commercial products. We chose a pink colour for our product to help differentiate it from other lotions available in the hospital and this may explain why our product was most preferable in terms of colour. The commercial products used for this study were colourless. We also added some perfume to our product to improve its acceptability and this may have paid off as our product had the highest score for smell. Although colourants and fragrances may cause allergic reactions, their addition has not been shown to reduce the efficacy of the active ingredients (World Health Organization, 2009; Ophaswongse and Maibach, 1994).
Our in-house produced hand sanitizer containing 83% ethanol showed a higher bacterial reduction than other products with 62 and 70% ethanol. Although products with higher concentrations of alcohol are considered to be less effective than lower concentrations above 60%, (World Health Organization, 2009) other factors may also contribute to higher effectiveness of some products. The use of gels like Aloe Vera in commercial products may contribute to their lower efficacy in this study as many studies have shown (Kramer et al., 2002; Dharan et al., 2003; Ojajarvi, 1991). Our in-house product had a carbomer thickening agent but this was kept at a very low concentration.
The cost of our in-house sanitizer was significantly lower than that of commercial products. However, the salaries of Pharmacy staff involved in production was not factored in because they were also involved in production of other hospital lotions and materials and time spent on production of hand sanitizers was quite low. The cost per litre was N830 ($2.30) and is lower than those of locally produced hand sanitizers in Kenya, Mali, Bangladesh, Pakistan and Hong Kong which ranged from $0.30 - $0.50 per 100 ml of product, (World Health Organization, 2009) although these price estimates included personnel costs. At a time when the Nigerian economy is struggling and the exchange rate to the US dollar is unfavourable, imported hand sanitiser formulations are unattractive, further underscoring the need for locally-manufactured products as a viable option for hand hygiene (Kama-Kieghe, 2016).
One limitations of this study was our inability to perform a training on hand hygiene for our participants due to constraints in students’ schedules. Inability to standardize procedures among participants makes this study unable to meet the standard of a trial. Also funding constraints limited the size of our sample, species identification of bacterial isolates and detection of viruses and other organisms that could be carried on the hands of participants. Studies have shown efficacy of alcohol preparations on most viruses (Hulkower et al., 2011).
In conclusion, our study shows that this in-house produced hand sanitizer product provides higher bacterial reduction than commercial products, has good acceptability among users, and provides significant cost savings to the hospital.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors appreciate Dr. Samuel Ibok, Ms Susan Adie and Ms Sarah Akpan for their assistance in sample collection and processing.
REFERENCES
|
Budd A, Lukas S, Hogan U, Priscille K, Fann K, Hill P, Wong R. (2016). A case study and the lessons learned from in-house alcohol based hand sanitizer production in a district hospital in Rwanda. Journal of Service Science and Management 9(02):150. |
|
|
Dharan S, Hugonnet S, Sax H, Pittet D (2003). Comparison of waterless hand antisepsis agents at short application times: raising the flag of concern. Infection Control & Hospital Epidemiology 24(3):160-164. |
|
|
Erasmus V, Daha TJ, Brug H, Richardus JH, Behrendt M D, Vos MC, van Beeck EF (2010). Systematic review of studies on compliance with hand hygiene guidelines in hospital care. Infection Control and Hospital Epidemiology 31(3):283-294. |
|
|
Godfrey C, Schouten JT (2014). Infection Control Best Practices in Clinical Research in Resource-Limited Settings. Journal of acquired immune deficiency syndromes (1999) 65(0 1):S15 |
|
|
Grayson ML, Jarvie LJ, Martin R, Johnson PD, Jodoin M E, McMullan C, Kelly AM (2008). Significant reductions in methicillin?resistant Staphylococcus aureus bacteraemia and clinical isolates associated with a multisite, hand hygiene culture?change program and subsequent successful statewide roll?out. Medical Journal of Australia 188(11):633-640. |
|
|
Gupta C, Czubatyj AM, Briski LE, Malani AK (2007). Comparison of two alcohol-based surgical scrub solutions with an iodine-based scrub brush for presurgical antiseptic effectiveness in a community hospital. Journal of Hospital Infection 65(1):65-71. |
|
|
Hulkower RL, Casanova LM, Rutala WA, Weber DJ, Hill C, Carolina N (2011). Inactivation of surrogate coronaviruses on hard surfaces by health care germicides. American journal of infection control 39(5):401-407 |
|
|
Kama-Kieghe S (2016). Local Production of Alcohol Based Hand Rubs (ABHR) in Nigeria - The Way of the Future? [Internet]. Infection Control. tips. [cited 2018 Nov 19]. pp. 1-5. |
|
|
Kramer A, Rudolph P, Kampf G, Pittet D (2002). Limited efficacy of alcohol-based hand gels. The Lancet 359(9316):1489-1490. |
|
|
Nabavi M, Alavi-Moghaddam M, Gachkar L, Moeinian M.( 2015). Knowledge, Attitudes, and Practices Study on Hand Hygiene Among Imam Hossein Hospital's Residents in 2013. Iranian Red Crescent Medical Journal 17(10). |
|
|
Nejad SB, Allegranzi B, Syed SB, Ellis B, Pittet D (2011). Health-care-associated infection in Africa: a systematic review. Bulletin of the World Health Organization 89(10):757-765. |
|
|
Ojajärvi J (1991). Handwashing in Finland. Journal of Hospital Infection 18:35-40. |
|
|
Ophaswongse S, Maibach HI (1994). Alcohol dermatitis: allergic contact dermatitis and contact urticaria syndrome. Contact Dermatitis 30(1):1-6. |
|
|
Pittet D, Allegranzi B, Boyce J (2009). The World Health Organization Guidelines on Hand Hygiene in Health Care and their consensus recommendations. Infection Control & Hospital Epidemiology 30(7):611-622. |
|
|
Pittet D, Sax H, Hugonnet S, Harbarth S (2004). Cost implications of successful hand hygiene promotion. Infection Control & Hospital Epidemiology 25(3):264-266. |
|
|
Wolfensberger A, Durisch N, Mertin J, Ajdler-schaeffler E, Sax H (2015). Evaluating the tolerability and acceptability of an alcohol-based hand rub - real-life experience with the WHO protocol. Antimicrobial Resistance and Infection Control 4(1):1-7. |
|
|
World Health Organization (WHO) (2009). WHO guidelines on hand hygiene in health care. Geneva; 2009. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


