Full Length Research Paper

ABSTRACT
Overall, twenty of the world’s adult populations live with hypertension. Blood pressure determination forms an integral part of anesthesiologist’s evaluation of the patient prior to and during surgery. 25% of surgical patients have hypertension preoperatively. There are several risks related to untreated preoperative hypertension in perioperative and postoperative phase. The objective of this study was to determine the prevalence of preoperative hypertension and its intraoperative anaesthesia management among patients undergoing elective surgery at Hawassa University Comprehensive Specialized Hospital from March 20 to May 30, 2018. Institutional based cross-sectional study was employed. 423 patients that came for elective surgery at Hawassa University Comprehensive and Specialized Hospital from March 20 to May 30, 2018 were included in the study. The findings of this study showed that out of 423 patients studied, 232 (54.8%) and 191 (45.2%) were males and females, respectively, with the highest percentage (36.6) in age group 20 to 29 years, 6.9% were hypertensive, 11 (37.9%) of the hypertensive patients had abdominal procedures, 6 (20.6%) orthopedic procedures, 5 (17.3%) gynecological procedures, 5 (17.3%) undergone other type of surgical procedures (like neurological, plastic) and 2 (6.9%) thyroidectomy and ENT procedures. Beta Blockers were the most commonly used type of preoperative premedication for hypertensive patients. Majority of patients have had their procedure with general anaesthesia. Half was induced by thiopental and followed by propofol.
Key words: Pre-operative, hypertension, anesthetic management, elective surgery.
INTRODUCTION
Hypertension is defined as a sustained high blood pressure with a systolic blood pressure (SBP) >140 or diastolic blood pressure (DBP)>90 mmHg. Stage-1 hypertension is defined as SBP 140 to 159 mmHg and/or DBP 90 to 99 mmHg. Stage-2 hypertension is defined as SBP>160 SBP>180 or DBP>110 mmHg.
Prehypertension is defined as SBP 120 to 139 mmHg or DBP of 80 to 89 mmHg (Chobanian et al., 2003; United Nations, 2011).
It is the most important modifiable risk factor for cardiovascular, cerebrovascular and renal disease. The Comparative Risk Assessment Collaborating Group has identified hypertension as the leading global risk factor for mortality and as the third leading risk factor for disease burden (Ezzati et al., 2002; Kearney et al., 2004). Researchers have estimated that raised blood pressure currently kills nine million people every year (Aronson et al., 2007; Law et al., 2009).
Intraoperative hemodynamic abnormalities are associated with perioperative and postoperative cardiovascular events (cardiac death, myocardial infarction or stroke).
Hypertensive emergencies complicated by evidence of impending or progressive target organ dysfunction) require immediate BP reduction to prevent or limit the end-organ damage. Examples of hypertensive emergencies include hypertensive encephalopathy, intracerebral haemorrhage, subarachnoid haemorrhage, acute stroke, hypertension-induced acute renal dysfunction, hypertension associated unstable angina, acute myocardial infarction, acute coronary heart failure, and acute aortic dissection.
This study aimed to assess the prevalence of preoperative hypertension and its intraoperative anaesthesia management among patients undergoing elective surgery at Hawassa University Comprehensive and Specialized Hospital, Southern Ethiopia.
Statement of the problem
Preoperative hypertension is commonly encountered in patients that undergo surgery. While attempts have been made to standardize the method to characterize the intraoperative hemodynamics, these methods still vary widely.
In addition, there is a lack of consensus concerning treatment thresholds and appropriate therapeutic targets, making absolute recommendations about treatment difficult.
Blood pressure determination forms an integral part of anesthesiologist evaluation of patients’ condition prior to and during surgery. Despite this reliance on blood pressure, data are not available which indicate changes in blood pressure occurring pre-anesthetically in hospitalized patients. Since the majority of elective surgical patients have only had single blood pressure determination made prior to arrival in the operating room, the question invariably arises as to the importance, if any, which should be attached to differences between pre- anaesthetic blood pressure recording and those recording previously obtained (Aronson et al., 2007).
If a patient is truly found to have elevated blood pressure preoperatively, the possible risk from this can be considered in two phases: the anaesthetics and the postoperative periods. It is not unusual for a patient undergoing anaesthesia to have a fall in blood pressure during induction, followed by a pressure response and tachycardia with intubation, stabilization of blood pressure and heart rate during anaesthesia, and another rise during awakening and extubating. Thus, it is important to the blood pressure status of a patient undergoing any operation (Aronson et al., 2007).
Acuteintra operative acute blood pressure elevations of over 20% during surgery are considered a hypertensive emergency and chronic hypertensive patients are more likely to have labile hemodynamic during a procedure. Even small blood pressure elevations during surgery can result in increased risk of postoperative mortality and renal failure, especially during cardiovascular procedures.
In Ethiopia context, limited studies were carried out regarding the prevalence and associated factors of preoperative hypertension and its management. This study was conducted to assess the prevalence of preoperative hypertension among the patients that undergone elastic surgery at Hawassa University Comprehensive and Specialized Hospital, Southern Ethiopia.
LITERATURE REVIEW
The magnitude of the problem
Approximately 20% of the world’s adults are estimated to have hypertension. The prevalence dramatically increases in patients older than 60 years. In many countries, 50% of individuals in this age group have hypertension. Worldwide, approximately 1 billion people have hypertension, contributing to more than 7.1 million deaths per year. National health surveys in various countries have shown a high prevalence of poor control of hypertension.
The report of World Health Organization showed that prevalence of hypertension is 22% in Canada, of which 16% is controlled; 26.3% in Egypt, of which 8% is controlled; and 13.6% in China, of which 3% is controlled. The reported prevalence of hypertension varies around the world, with the lowest prevalence in rural India (3.4% in men and 6.8% in women) and the highest prevalence in Poland (68.9% in men and 72.5% in women). Hypertension is an important public health challenge worldwide because of its high prevalence and a concomitant increase in the risk of disease (Law et al., 2009; WHO, 2015).
Approximately 40% of adults aged 25 and above were diagnosed with hypertension globally in 2008; the number rose from 600 million in 1980 to 1 billion in 2008. The increasing prevalence of hypertension is attributed to population growth, ageing and behavioural risk factors, such as unhealthy diet, harmful use of alcohol, lack of physical activity, excess weight and exposure to persistent stress (WHO, 2015).
In high-income countries, numerous studies have been conducted to estimate the prevalence of hypertension. In some countries, national studies have provided estimates of the prevalence of hypertension. In sub-Saharan Africa (SSA) countries like Ethiopia, published information on the prevalence of hypertension is sparse. Studies done in Ethiopia, Kenya, Nigeria and Tanzania, reported a prevalence of hypertension ranging from 10.1% in Southern Ethiopia to 23.7% in Tanzania (WHO, 2015; Shishani et al., 2013). Previous reports from Ethiopia on the prevalence of hypertension were as high as 31.5 and 28.9% among males and females, respectively in Addis Ababa (Law et al., 2009) and 28.3% from Gondar (Van et al., 2006).
A retrospective observational study done in Kathmandu University in 2011, showed that the total prevalence of hypertension in the preoperative phase was 10.16%. Among them, 64.9% were male and 35.1% female. Maximum prevalence was found in the age group 50 to 59 years (26.6%). Among the cases detected, the highest percentage (52%) was patients with newly diagnosed hypertension and among those on medications, 61.1% were using calcium channel blockers (Awoke et al., 2012).
Induction of anaesthesia is accomplished with incremental doses of thiopental (8 mg/kg) followed by succinylcholine unless contraindications exist. Etomidate or propofol may also be used. Esmolol is particularly effective in blunting the increases in heart rate and blood pressure during laryngoscopy and intubation and is used liberally during the induction period. Blood pressure responses during and after endotracheal intubation are unpredictable in this patient population, and the clinician must be prepared for immediate treatment of extremes in blood pressure. The preference is to use short-acting drugs, such as phenylephrine (50 to 100 μg) for hypotension and sodium nitroprusside (5 to 25 μg) for hypertension. Patients with poorly controlled hypertension (diastolic blood pressure >100 mm Hg) require special care. These patients often have intravascular volume depletion and may have significant hypotension with induction. Administration of fluids intravenously (5 ml/kg), careful titration of anaesthetics, and immediate treatment of hypotension are especially important (Sapkata et al., 2011; Lemba et al., 2012).
Anaesthesia is maintained with 50% nitrous oxide in oxygen and low-dose (less than one-half MAC) potent inhaled anaesthetics. Isoflurane may be preferred because fewer ischemic electroencephalographic (EEG) changes occur during carotid occlusion when compared with halothane or enflurane (Law et al., 2009).
Angiotensin-receptor antagonists were prescribed for 49% of patients followed by diuretics (41%), calcium-channel antagonists (39%), ACE inhibitors (25%), and beta-blockers (25%) (Law et al., 2009).
The risk factors associated with the problem
Common predictors of perioperative hypertension are the previous history of hypertension, especially a diastolic blood pressure greater than 110 mm Hg and the type of surgery.
In 2004, two recent retrospective case-control studies in Britain examined the risk factors for cardiovascular death within 30 days of anaesthesia in elective surgery. The controls were matched for age, the same operation and same surgeon, but did not die. For the elective patients, a diagnosis of hypertension was a risk factor; but there were no differences between admission blood pressures between cases and controls. While both studies suggest there is no association between admission blood pressure and perioperative outcome, they were both limited by the fact that most of the patients had stage 1 or 2 hypertension with few patients showing blood pressures in the stage 3 range. Analysis of more recent data does not show an association between hypertension and 30 days of cardiac mortality. This may reflect either change in standards of perioperative care, perioperative drug therapies and monitoring or improvement in the standard of care of the hypertensive patient in the community leading to fewer patients exhibiting the complications of end-organ damage (Reich et al., 2002).
Isolated systolic hypertension (ISH), which accounts for the majority of hypertensive patients aged over 60 years, is a new focus of interest in Britain. As a corollary of the increase in systolic and pulse pressure, there is an increased cardiovascular risk. Early studies used a standard definition of hypertension (diastolic pressure >95 mm Hg) and it is clear from the data that many of the patients had significant ISH. Similarly, later studies of the association of admission blood pressure and complications have focused on older patients.
Therefore, it is likely that the majority of poorly controlled hypertensive in these studies had ISH. A recent study has examined the association between ISH and cardiovascular complications in patients undergoing cardiac surgery. This was a prospective study of over 2000 patients who were classified according to their preoperative blood pressure: normal; ISH (systolic >140 mm Hg); diastolic hypertension (diastolic >90 mm Hg); or a combination of the two. After adjusting for other confounding risk factors, ISH was associated with a small but significant increase in the likelihood of perioperative morbidity but not mortality.
A recent update in Britain has re-examined data from 30 studies published between 1978 and 2001 involving 13,666 patients. The outcome was assessed in terms of major cardiovascular complications including myocardial infarction and cardiac death. Most of the individual odds ratios were not significantly different from unity (Williams et al., 2008).
MATERIALS AND METHODS
Study area
The study was conducted at Hawassa University Comprehensive and Specialized Hospital (HUSCH) which is found in Hawassa City, of South Nation, Nationalities and People’s Regional State, Southern Ethiopia. It is 276 km from Addis Ababa. The hospital gives surgical, medical, gynaecological, obstetrical, paediatrics, urological, orthopaedic, ophthalmological, and other services. It has ten operation rooms, six of them are for emergency and elective surgical, gynaecological, paediatrics and neurological, two for ophthalmological surgery and the other two for obstetric surgery.
Study design
Institutional based cross-sectional study was employed.
Study population
All patients who had elective surgery in HUCSH from March 20 to May 30, 2018 were included in the study.
Inclusion criteria
All patients who had elective surgery at HUCSH with the study period.
Exclusion criteria
Patients who were critically ill, those patients cannot provide a response to the data collector during the data collection time due to their illness. Neurological surgery [almost all are Emergency cases], ophthalmology surgery [all are pediatric case], pediatrics surgery [age less than 15], and patients below 20 years of age.
Sampling size determination and sampling procedure
The sample size was determined by using a single population proportion formula. To determine minimum sample size, the study considered a 50% prevalence of preoperative hypertension at 95% confidence interval and maximum discrepancy of ±5% between the sample and the underlining population. There is similar study conducted in the area and the same study is also limited in the country. Taking into consideration a 10% non-response rate and the final sample size was 423. In order to reach the calculated sample size for the study, all patients under gone elective surgery in study period were interviewed.
Data collection instruments
The questionnaire was prepared in English language and translated to local language to make the data collection easier and understood by respondents. Before the actual data collection pretest was conducted on the 5% of sample size in another Government Hospital located in the city. The contents of the questionnaire were modified based on the result of the pretest.
Data collection and data collectors
Data were collected by trained data collectors. Data collectors were well informed about the study to provide a sufficient information or informed consent for respondents to get reliable data. On-site supervision was carried out to supervise and check the completeness, accuracy and consistency and corrective measures was taken when needed.
RESULTS
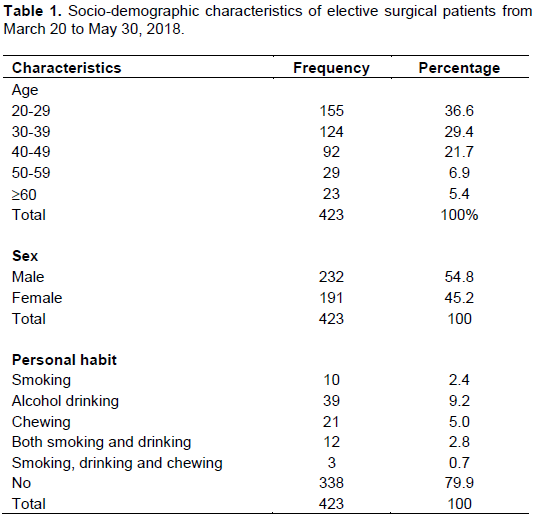
Socio-demographic characteristics of respondents
A total of 423 patients participated in the study. Participants’ ages ranged from 20 to 84 years. 232 (54.8%) of the participants were males and 191 (45.2%) were females. Concerning personal habit of respondents, 9.2% of respondents were drinking alcohol currently, 5.0% had a past or present history of chewing chat and 2.4% had a history of smoking cigarette (Table 1).
Risk factors, stage of hypertension and procedures done
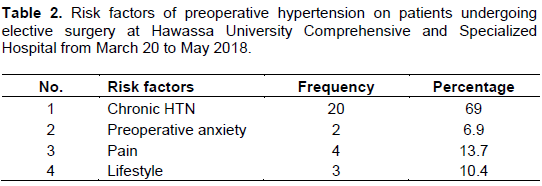
From preoperatively hypertensive patients, 69% were found to be due to chronic hypertension and other factors like preoperative anxiety, pain and lifestyle accounts for 6.9, 13.7, and 10.3%, respectively.
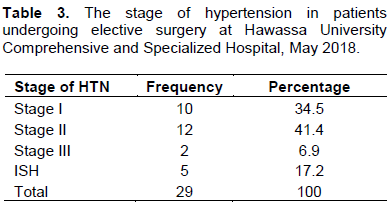
Among patients who were hypertensive preoperatively, stage-2 (41.4%) hypertension was the commonest followed by stage 1 (34.5%) and stage-3 accounts for about 6.9% (Table 3). Regarding their stage of hypertension and premedication, patients who had a stage-3 hypertension all had premedication. 66.7 and 92.3% of stage-1 and stage-2, respectively (Table 2).
Among the patients who undergone elective surgery, about 12 (41.4%) of them had stage-2 hypertension, followed by stage-1, which accounts for 10 (34.5) of the participants (Table 3).
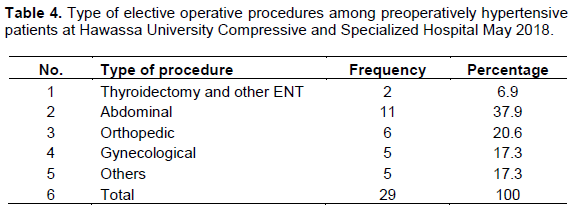
The procedures done for preoperatively hypertensive patients were abdominal, orthopaedic, gynaecological, and ENT, with abdominal procedures, accounting for 37.9% and orthopaedic, thyroidectomy and gynecologic procedures constituting 6, 2, and 5%, respectively (Table 4).
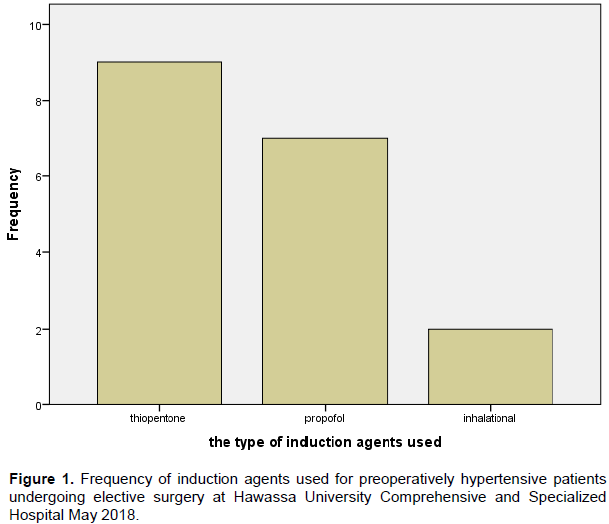
Among patients undergone their procedure on general anaesthesia, 50% were induced by thiopental, 38.9% were induced by propofol and 11.1% were by inhalational anaesthetics (Figure 1).
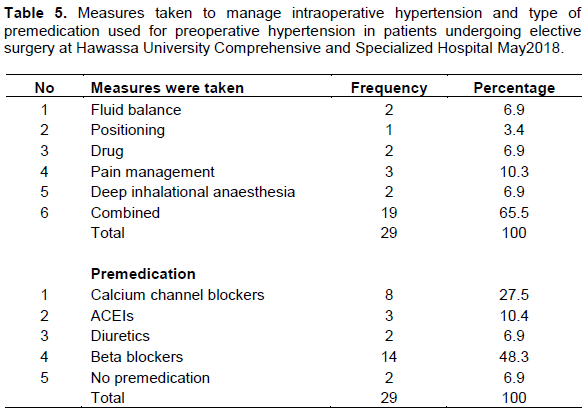
The most commonly used type of preoperative pre-medication used for preoperatively hypertensive patients were beta blockers and calcium channel blockers which accounted for 48.3 and 27.5%, respectively (Table 5).
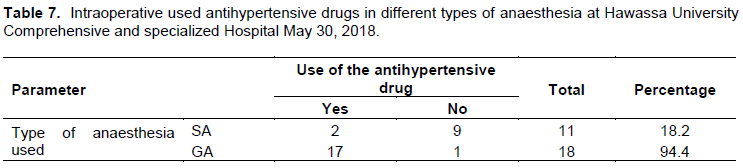
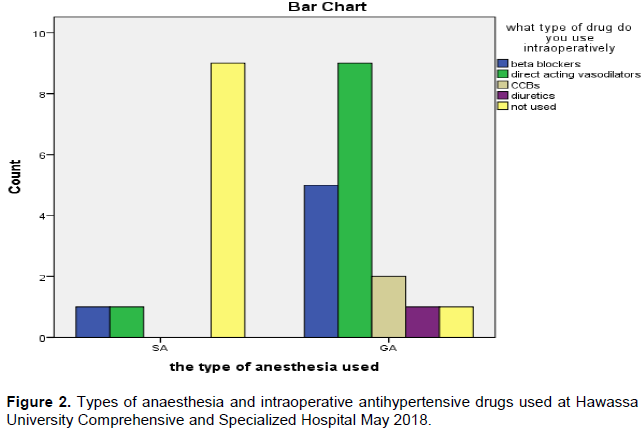
Patients (62.1%) undergone their procedure with general anesthesia (GA). 94.4% were given antihypertensive drugs intraoperative and 37.9% had the surgery with spinal anesthesia (SA) and only 18.2% of them given intraoperative antihypertensive agents. Commonly used antihypertensive drug in the intraoperative period for patients who were given general anaesthesia was direct-acting vasodilators (50%) followed by beta-blockers (27.8%) and in case of spinal anaesthesia, both direct acting vasodilators and beta blockers were used equally (9%).
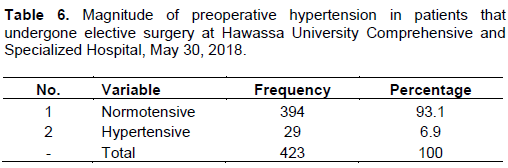
Majority of the total number of patients (93.1%) were in the category of normative in their preoperative hypertension classification, while the rest of them were under the category of Hypertensive (Tables 6 and 7 and Figure 2).
DISCUSSION
The result showed that 6.9% of patients were hypertensive which is consistent with a study done in Kathmandu University on 2011 (10.16%) (Van et al., 2006). And a study done in China 13.6% (Law et al., 2009). However, the finding of this study was lower than the study done in Canada where 22% of the patients were hypertensive (Law et al., 2009), USA in 2008 (30%) 9.13 and Egypt 26% (United Nations, 2011; Law et al., 2009).
The finding of this study was similar to the study done in Ethiopia in general population which is 10.1% in Southern Ethiopia. In contrast, it is lower as compared with the study done in Addis Ababa which was 31.5% in males and 28.8 in females (Law et al., 2009) and Gonder 28.3% (Van et al., 2006). This may be due to the different lifestyles among these populations.
From this study, males seemed predominantly more affected than females with the ratio being 1.6:1 which is consistent with the study done in Kathmandu University on 2011 but coinciding with that of worldwide data 2007 (Van et al., 2006).
Among preoperatively hypertensive patients, 69% were found to be chronically hypertensive and they were on medication, 13.7% were found to have increased blood pressure due to pain and 10.4% were hypertensive secondary to their lifestyle whereas the remaining 6.9% had anxiety as a risk factor for increased blood pressure.
Amongst the 29 hypertensive patients, 11 (37.9%) under underwent abdominal procedures, 6 (20.6%) undergone orthopedics procedures and 5 (17.3%) undergone gynecological procedures, 5 (17.3%) undergone other type of surgical procedures (like neurological, plastic,...) and around 2 (6.9%) undergone thyroidectomy and ENT procedures. Out of 29 hypertensive patients, 10 (34.5%) were at stage-1, 12 (41.4%) were at stage-2, 2 (6.9%) were at stage-3 and
the remaining 5 (17.2%) were ISH.
Patients (62.1%) had their procedure with GA out of which 94.4% were given antihypertensive drugs intraoperative and 37.9% have undergone the surgery with SA and only 18.2% of them were given intraoperative antihypertensive agents. The possible reason for this is the drugs used for spinal anaesthesia decrease the blood pressure because they have a vasodilative effect so that the need for intraoperative antihypertensive medication decreases when spinal anaesthesia is used. If general anaesthesia is used there are drugs and techniques that exacerbate hypertension, so that intraoperative antihypertensive drugs are used mostly.
About 50 and 38.9% of patients who were hypertensive and undergone surgery by general anaesthesia was induced by thiopental and propofol, respectively and ketamine was not used as an induction agent for hypertensive patients. Since it has the sympathomimetic effect it causes a marked increase in blood pressure especially in hypertensive patients is the possible explanation for not using ketamine as an induction agent for hypertensive patients.
CONCLUSION
The total hypertensive patients in the preoperative period were 6.9% and the most preoperatively used anti-hypertensive drug was beta blockers (48.3%) followed by calcium channel blockers (CCBs; 27.5%). Majority of the patients with preoperative hypertension were chronically hypertensive, which accounts for 69%. Majority of the patients with preoperative hypertension underwent the abdominal procedure. Majority of the patients had their procedure with GA. Knowing the prevalence will help in proper preoperative optimization of the hypertensive patients and also help in decreasing the incidence of postoperative complications.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors would like to thank the administrative body of the hospital for allowing them to conduct this study. They also like to thank the study participants for their valuable information and volunteer participation in this study.
REFERENCES
|
Aronson S, Fontes ML, Miao Y, Mangano DT (2007). Risk index for preoperative renal dysfunction/failure: critical dependence on pulse pressure hypertension. Circulation 15:733-742. |
|
|
Awoke A, Awoke T, Alemu S, Megabiaw B (2012). Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-sectional study. BMC Cardiovascular Disorders 12(1):113. |
|
|
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL (2003). The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. Jama 289(19):2560-2571 |
|
|
Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murray CJL (2002). Comparative risk assessment collaborative group: selected major risk factors and global and regional burden of disease. The Lancet 360(9343):1347-1360. |
|
|
Kearneya PM, Wheltona M, Reynoldsa K, Wheltona PK, He J (2004). Worldwide prevalence of hypertension: a systematic review. Journal of Hypertension 22:11-9 |
|
|
Law MR, Morris JK, Wald NJ (2009). Use of blood pressure-lowering drugs in the prevention of cardiovascular disease: a meta-analysis of 147 randomized trials in the context of expectations from prospective epidemiological studies. BMJ 38:b1665. |
|
|
Law MR, Morris JK, Wald NJ (2009). Use of blood pressure-lowering drugs in the prevention of cardiovascular disease: a meta-analysis of 147 randomized trials in the context of expectations from prospective epidemiological studies. BMJ 338:b1665. |
|
|
Lemba D, Reese A, Gelaye B, Lemma S, Berhane Y, Williams MA (2012). Prevalence of hypertension and diabetes among Ethiopian adults. Diabetes & Metabolic Syndrome: Clinical Research and Reviews 6(1):36-41. |
|
|
Reich DL, Bennett-Guerrero E, Bodian CA (2002). Intraoperative tachycardia and hypertension are independently associated with adverse outcome in non-cardiac surgery of long duration. . Anesthesia Analgesia 95(2):273-277. |
|
|
Sapkata S, Sherpa M, Bhattarai B (2011). Incidence of hypertension in patients undergoing surgery at Dhulikhel Hospital-Kathmandu University Hospital. Kathmandu University Medical Journal 9(2):40-43. |
|
|
Shishani K, Dajani R, Khader Y (2013). Hypertension risk assessment in the largest ethnic groups in Jordan. Journal of Immigrant and Minority Health 15(1):43-48. |
|
|
United Nations (2011). Department of Economic and Social Affairs, Population Division. World population prospects. New York. The 2010 Revision, Volume I: Comprehensive Tables. ST/ESA/SER.A/313. |
|
|
Van H, Byass P, Chuc N, Wall S (2006). Gender differences in prevalence and socioeconomic determinants of hypertension: findings from the WHO STEPs survey in a rural community of Vietnam. Journal of Human Hypertension 20(2):109. |
|
|
World Health Organization (WHO) (2015). Raised blood pressure. Situation and trends. Global Health Observatory (GHO) data (cited 2015); |
|
|
World Health Organization (WHO) (2015). A global brief on hypertension. The silent killer, global public health crisis [cited 2015]; |
|
|
Williams B, Lindholm LH, Sever P (2008). Systolic pressure is all that matters. The Lancet 371(9631):2219-2221. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


