ABSTRACT
In many of the textile industries, workers are largely exposed to cotton dust, which can leave workers with respiratory disorders. The aim of this study was to evaluate respiratory status of workers exposed to cotton dust in Arba Minch textile factory, Southern Ethiopia, 2017. A comparative cross sectional study was done and 51 workers exposed to cotton dust in the factory and 51 age and sex matched controls were investigated. Their lung function was measured with a pocket size digital Spirometer. A standardized questionnaire based on British Medical Research Council Questionnaire was used to assess respiratory system symptoms and use of personal protective devices. This study reveals that the percentage prevalence of cough, phlegm, wheeze, breathlessness and chest tightness was 64.7, 55, 39, 41 and 43% for exposed respondents, respectively and 25.5, 14, 8, 6 and 0% for control subjects, respectively. Lung function indices such as, forced vital capacity (FVC), forced expiratory volume in one second (FEV1), peak expiratory flow rate (PEFR) and forced mid expiratory flow between 25 and 75% of FVC (FEF25-75%) were higher in control respondents than in exposed respondents and the mean difference was found to be statistically significant (p<0.05) and the mean difference of predicted percentage values of FVC and FEV1 between the groups was found to be statistically significant (P<0.05). FEV1% was higher in the control group than in exposed group. Therefore, the factory management should provide personal protective devices (PPDs) to exposed employees and should train them.
Key words: Cotton dust, textile, lung functions, respiratory symptoms.
Abbreviation:
AAU, Addis Ababa University; ANOVA, analysis of variance; BMRC, British Medical Research Council; COPD, chronic obstructive pulmonary diseases; DRPC, Department Research and Publication Committee; FEF25-75%, forced mid expiratory flow between 25 and 75% of FVC; FEV1, forced expiratory volume at first second; FVC, forced vital capacity; GOLD, global initiative for chronic obstructive lung diseases; ILO, International Labor Organization; OSH, Occupational Safety and Health; OSHA, Occupational Safety and Health Administration; PEFR, peak expiratory flow rate; PEL, permissible exposure limit; PPDs, personal protective devices; SNNPR, South Nations Nationalities and Peoples Region; SPSS, Statistical Package for Social Science.
Textile industry is one of the oldest large-scale economic activities that led the industrialization process since centuries ago and the first manufacturing industry to have a worldwide dimension. This sector is the most geographically wide spread of all industries across the developed and developing countries including Africa (Ethiopian Textile Industry: Status and Growth Prospects,2013). In spite of their importance, industries associated with the processing of cotton, specifically yarn, thread and fabric mills are most associated with worker exposure to cotton dust (Neil et al., 2011; Michael, 2004). Studies reported that exposure to cotton dust provokes respiratory effects (Kilburn, 1998; Christiani et al., 2001). The effects of exposure to cotton dust are usually evaluated as changes in respiratory symptoms over shift or terms of decline over the years (Zhong et al., 2002).
In many of the textile industries, workers are largely exposed to dust. Industrial workers in developed countries are very careful about occupational health, but this issue is quite neglected in developing countries (Hagling et al., 1981). Occupational safety and health is a key element in achieving sustained decent working conditions and strong preventive safety cultures (ILO, 1980). According to ILO world day report for safety and health at work, worldwide an estimated 2.34 million people die each year from work-related accidents and diseases. Nowadays, the world community has been facing increasing risks of respiratory diseases due to smoke, dust exposure, indoor and outdoor air pollution, occupational hazards, and infections in different industrial sectors (ILO, 2013).
Textile industry is one of the largest manufacturing industries, in which workers especially in the bale opening, carding, spinning and weaving sections, are exposed to large amount of cotton dust with deleterious effects on their lung function (Mannino and Buist, 2007; Wang et al., 2005). In low and middle income country, including Africa, occupational respiratory symptoms and diseases are very high due to the expansion of investments, high unemployment rate; workers are probably more likely to continue working even when having poor health status and old machines that are producing excessive dust to work environment are still used for production purpose (WHO, 2010).
A lot of studies have been done concerning textile workers mostly in Asia (Christiani et al., 2001), Europe (Simpson et al., 1998), but only scantly data is available for Africa, particularly Ethiopia. In Ethiopia, only a few cross sectional studies were conducted to explore the adverse effect of cotton dust on workers well-being in a textile mills. As it stands now, further studies on cotton dust effect have been highly useful in understanding the risks of working in textile mills and the prevalence of respiratory symptoms and lung function impairment in the textile factory workers in comparison to non-exposed groups (peoples working in cotton dust free sectors). This is useful to minimize the occurrence of highly rising occupational respiratory problems in people working in textile mills.
Study area
Found in Arba Minch town. Arba Minch town is located in Gamo Gofa Zone, in Southern Nations Nationalities and Peoples Region (SNNPR) and at a distance of 454 km from Addis Ababa and 276 km from Hawassa (the capital city of SNNPR). Arba Minch textile mill was opened with 193 million Ethiopian birr on May 6, 1992 with the aim of satisfying the enormous need for polyster/cotton blended fabric in the country. The factory supplies high quality yarn and woven fabrics made from cotton and polyster/cotton mixed fibers to the local and international markets. There were about 181 production workers in spinning department which consists of 6 working sections (blowing, carding, drawing, roving ring frame and reeling) and 109 workers in preparatory and loomshed sections of weaving department. Totally, there were 290 production workers (that is, those involved in the direct processing of textile materials) in different sections of the factory. The final output of spinning department is yarn production whereas the output of weaving department is fabric production.
Study design
A comparative cross sectional study design was conducted.
Study subjects
Study group
The study was conducted on 51 workers selected from the textile factory. Each subject who participated in this study did it based on his/her own full voluntariness and having ages ranging from 18 to 60 years.
Control group
A total of 51 volunteers from areas free of cotton dust were selected as a control group for this study. These included administration workers in the factory, university instructors, students and administration workers living in Arba Minch town, whose age ranges from 18 to 60 years.
Inclusion criteria: Workers who had direct involvement in the production unit or cotton processing unit and had exposure to cotton dusts for minimum of one year were included.
Exclusion criteria: Workers with abnormalities of vertebral column and thoracic cage, diagnosed cases of pulmonary tuberculosis, bronchial asthma, chronic bronchitis, emphysema and other respiratory diseases were excluded. Those who had past history of abdominal or chest surgery were not be allowed to participate in the study. Workers aged over 60 were excluded as many studies have reported the effect of aging on pulmonary function. Smokers, pregnant women, individuals with unstable cardiovascular status and workers who stayed at work for less than one year were not included.
Control subjects
Inclusion criteria: Workers from areas free of cotton dust were included. Age and sex matched individuals with that of exposed subjects were included.
Exclusion criteria: Individuals with abnormalities of vertebral column and thoracic cage, diagnosed case pulmonary tuberculosis, bronchial asthma, chronic bronchitis, emphysema and other respiratory diseases were excluded. Those who had undergone abdominal or chest surgery, pregnant women and individuals with unstable cardiovascular status and smokers were excluded from the study.
Sample size determination and sampling techniques
The sample size was determined by double population proportion formula; the likely percentage value for exposed group (43%) and the likely percentage value for control (14%) were obtained from study on lung function in textile mill workers (Nagoda et al., 2012). Based on the calculation, the determined sample size in each group was 46 and assuming non-response rate, 10% of the calculated sample size was added. Such that the total sample size was 102, 51 for exposed group and 51 for control group. Based on proportional allocation, 32 exposed subjects were selected from spinning department working sections and the remaining 19 subjects were selected from weaving department. Both stratified sampling and simple random sampling methods were utilized to select study participants from the Arba Minch textile factory and proportional allocation method was used to determine sample size of each strata. Subjects who had direct involvement in the processing areas were selected and included in exposed group. Healthy and volunteered subjects who had no direct involvement in processing areas or working in cotton dust free sectors in the factory and in the same town who matched with the age range and sex to the exposed subjects were taken as a control group for better comparison.
Data collection methods and procedures
A standardized questionnaire based on British Medical Research Council (BMRC) Questionnaire 1986 version, was used to assess personal information, respiratory system symptoms, occupational history, past illness, family history and use of personal protective devices (PPDs). The study participants were interviewed by the trained interviewers. Before the interview, brief explanation was given to each subject about the purpose of the study to avoid anxiety in the subjects and to develop good rapport. The questionnaire was translated into Amharic language and administered to all control and exposed subjects and then translated back into English to verify the accuracy and for statistical data analysis.
Anthropometric measurements
Weight and height of both the exposed and control subjects were measured with light clothing to the nearest 1 kg and without shoes to the nearest 1 cm, respectively.
Study equipment’s
The following equipment where used in the study:
(1) Spirometer: A pocket size digital Spirometer (Spiro-ProJAEGER) was used to measure lung function indices.
(2) Digital balance and measuring tape was used to measure weight and height of the subjects, respectively.
(3) A standard questionnaire based on British Medical Research Council (BMRC) questionnaire format was used to assess personal information, occupational history, respiratory symptoms, past illness, and use of PPDs.
Measurement of lung function test variables
Spirometry assessment was done in both control and exposed subjects. Using digital spirometer, FVC, FEV1, FEV1%, FEF25-75% and PEFR were measured. Before performing the actual procedure of the test, the spirometer was calibrated and the mouthpiece was cleaned by using antiseptic agents (70% alcohol). Subject’s personal data including sex, age, height, and weight were fed into the spirometer and was instructed to practice deep inspiration followed by complete forceful expiration. The subjects took 10 to 15 min of rest before performing the Spirometry. By putting a nose clip to prevent air leakage through the nose, the subject’s took full inspiration and expired out as hard and as fast as possible into the Spirometer. All measurements were made in the morning in a sitting position. Three readings were taken by giving 3 to 5 min rest in between the trials and from those readings the best or the highest was selected and recorded.
Data collection and analyses
First, the collected data was checked for completeness and consistency by the investigator and then, the following statistical activities were carried out. Microsoft Excel 2007 was used to arrange and organize the data and Statistical Package for Social Science (SPSS) version 21 was utilized to analyze the data. Descriptive statistics was utilized to summarize service year, job description, use of PPDs and anthropometric measurements of subjects. Chi-square test with Yates continuity correction and Odds ratio were used to analyze and estimate the prevalence of respiratory system symptoms such as cough, phlegm, productive cough, breathlessness, chest tightness and wheezing in both groups.
Independent sample t-test was applied to compare the mean respiratory values of exposed and non-exposed group in each subgroup (Age ranges). One way analysis of variance (ANOVA) was served to check the presence of significant differences in lung functions of exposed subjects across different service year categories. Pearson’s correlation coefficient was used to quantify the degree of linear relationship between respiratory system measurements and duration of exposure. The data was expressed in terms of Mean±standard deviation (SD), number and percentage. Statistical significance was tested at 5% and expressed in terms of p-value with p<0.05 which was considered to be statistically significant.
Ethical considerations
Before getting into the investigation work, ethical clearance and permission was obtained from Medical Physiology Department Research Committee (DRC), Addis Ababa University (AAU). Then, permission from the factory manager and full voluntariness of the study participants to engage in this work was secured. Any information that is obtained in connection with the study participants and that can be identified with the participants would be kept confidential.
Socio-demographic characteristics of the study participants
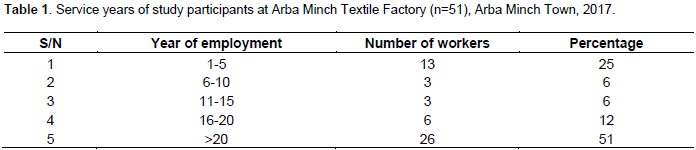
The data was collected from all 102 study participants with 100% response rate. Regarding the job description, from 51 subjects in exposed group, 63% (n=32) of the respondents were from spinning department and 37% (n=19) of respondents were from weaving department. Out of 51 subjects in non-exposed group, 63% (n=32), 19% (n=10), 8% (n=4), and 10% (n=5) were administration workers in the factory, summer students, instructors and administration staff in Arba Minch University, respectively. Each group had 53% (n=27) male and 47% (n=24) female participants. Out of 51 exposed workers, 26 (51%) of the study participants had a service year above 20 years and 13 (25%) had a service period of 1 to 5 year. Out of 51 subjects in exposed group, 57% (n=29) attended secondary education and majority of the subjects in the control group were certificate/diploma holders. Subjects were grouped by their ages using an interval of five years; majority of the respondents in both groups were within the range of 41 to 45 years of age. The minimum and maximum service year of the exposed respondents was 2 and 29 years, respectively. All participants in both groups were fulltime workers (that is, employees were working 8h per day) 1 to 5 year (Table 1).
The study reveals that the mean age of exposed and non-exposed respondents was 38.45 years with a range of 21 to 50 years and 36.20 years with a range of 21 to 53 years, respectively. The result of the study shows that the mean height and weight of the exposed respondents were 157.65 cm (range: 141 to 175 cm) and 63.45 kg with a range of 40 to 93 kg; the mean height and weight of the control respondents were 164.06 cm with a range of 152 to 177 cm and 63.49 kg with a range of 42 to 84 kg, respectively. The result of the study reveals that the anthropometric measurements of exposed and non-exposed study participants were found to be near similar. The mean and standard deviations of anthropometric measurements are shown in Table 2.

Workers awareness and practice of wearing personal protective devices
All the 51 respondents agreed with the idea that all textile factory workers should wear personal protective devices. The workers complained that, there is no supply of any personal protective devices in the factory. In addition, all of the workers replied that they did not get awareness about proper utilization of PPDs and its importance from the factory administration. Even though, workers of the factory have free medical services, there is no extra measure taken as part of a protective tool. All the workers were aware of the impact of cotton dust on their health. Out of 51 subjects, 78% (n=40), 9% (n=4) and 68.6% (n=35) were responded that exposure to cotton dust causes problem to lung and airways, lung and heart, and lung, airways and eyes, respectively.
Prevalence of respiratory symptoms
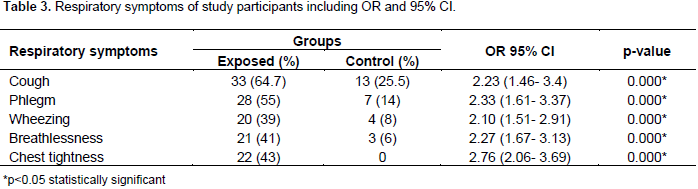
This study revealed that the percentage prevalence of cough, phlegm, wheeze, breathlessness and chest tightness was 64.7, 55, 39, 41 and 43% for exposed respondents, respectively and 25.5, 14, 8, 6 and 0% for control subjects, respectively. The result shows higher percentage prevalence of respiratory symptoms among exposed respondents compared to the control respondents. The odds of cough in workers exposed to cotton dust was 2.23 times (OR=2.23, 95% CI: 1.46, 3.4) more than was in the controls and the statistical association was found to be significant. Those respondents exposed to cotton dust had phlegm 2.33 times (OR=2.33, 95% CI: 1.61, 3.37) more than was in the respondents not exposed to cotton dust and the statistical association was found to be significant. The odds of wheeze was 2.1 times (OR=2.1, 95% CI=1.51-2.91) higher for exposed respondents than for non-exposed respondent and the association was found to be statistically significant. The odds of breathlessness was 2.27 times (OR=2.27, 95%CI=1.65-3.13) higher for exposed respondents than for non-exposed respondents and the association was found to be statistically significant. The odds of chest tightness was 2.76 times (OR=2.76, 95%CI= 2.06, 3.69) higher for exposed respondents than for non-exposed respondents and the association was also found to be statistically significant (Table 3).

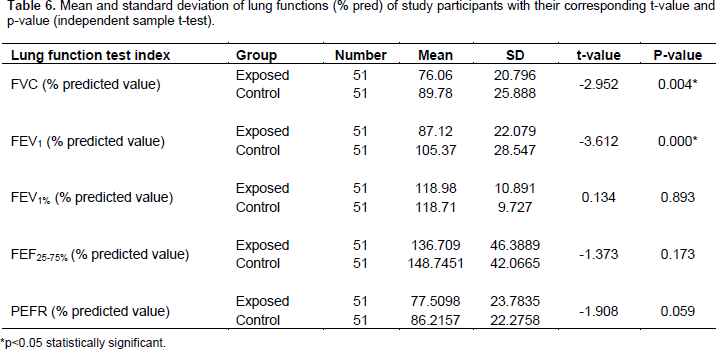
Similarly, the percentage of the predicted values of lung function indices were lower in exposed group than in control. And the mean difference of predicted percentage of FVC and FEV1 between the groups was found to bestatistically significant (P<0.05) as shown in Table 6. The lung functions of exposed and control group were compared across different age ranges. For FVC and FEV1 values across age ranges of 31-35, 41-45 and 46-50 years of the study participants, controls had greater lung function and the mean difference was statistically significant (P<0.05). Regarding lung function value of FEV1 for age category (26-30 years), controls had greater lung function than exposed subjects and the difference was statistically significant.

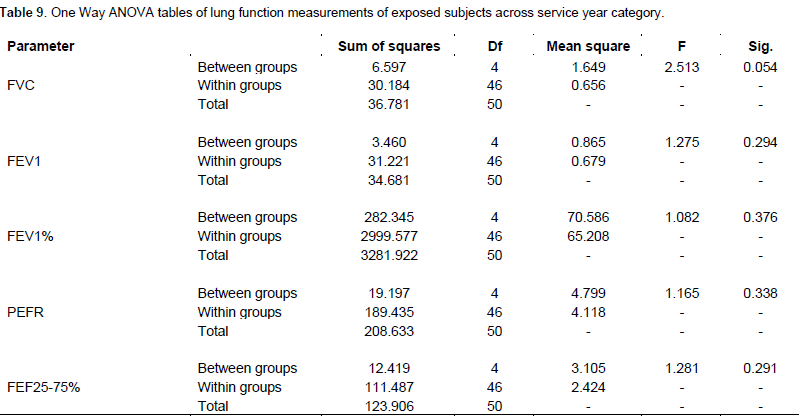
Pearson correlation was used to see the relationship between service year and lung function measurements. There was a negative correlation between lung functions and duration of exposure, but it was not statistically significant (P>0.05) (Table 8). One way analysis of variance was applied to check the presence of significant difference in means of lung func-tions of exposed group among different service years, but the mean differences were not found statistically significant (P>0.05) as shown in Table 9.
The main purpose of this study was to evaluate the effect of cotton dust on respiratory system of textile mill workers. Different techniques and parameters were used to assess the exposure effect of cotton dust on res-piratory function of workers of Arba Minch textile factory. All the exposed subjects agreed with the idea that, factory workers should wear the personal protective devices at work time. Even though they knew the fact that the workers should wear PPDs at working time, all of them agreed that they were not informed about proper usage and purpose of PPDs from the factory manage-ment (employers). The result of this study revealed nil supply of the PPDs in the factory.
The percentage prevalence of respiratory symptoms including cough, phlegm, wheeze, breathlessness and chest tightness for the exposed respondents was 64.7, 55, 39, 41 and 43%, respectively. The corresponding percentage prevalence of respiratory symptoms for control subjects were 25.5, 14, 8, 6 and 0% for cough, phlegm, wheeze, breathlessness and chest tightness, respectively. The result of the study showed that cough was the most prevalent respiratory symptom among exposed subjects. The odds of cough was found to be 2.23 times higher in exposed than in non-exposed respondents (OR=2.23).
This finding is in agreement with the study conducted among textile factory workers in Kano, Nigeria which showed a higher prevalence of work-related respiratory symptoms in exposed workers than in controls. The prevalence in exposed subjects were cough (43%), phlegm (41%), wheezes (13.5%), breathlessness (24.5%) and chest tightness (22.5%), whereas prevalence in control group were cough (14%), phlegm (23%), wheezes (1.5%), breathlessness (12%) and chest tightness (6%) (Nagoda et al., 2012). Another related study in Nigeria revealed that the prevalence of respiratory symptoms in the exposed group was higher than in the control group with cough and phlegm as the most common symptoms (Oyejide, 1989). A study in India, reported a higher prevalence of respiratory symptoms in cotton mill workers, 20% of the workers reported to have cough, 15% reported chest tightness and 19% complained of breathlessness (Pragati and Aruna, 2016). Christiani et al. (2001) reported a higher prevalence of respiratory symptoms in cotton textile workers.
Similar study in Egypt revealed a higher prevalence of respiratory symptoms in exposed group than in controls (Khalifa et al., 2003). The study done by Ghasemkhani et al., (2006) in South Tehran, Iran, found a significantly higher prevalence of respiratory symptoms related to textile industrial workers such as cough 30.8%, phlegm 53.8% and dyspnea 65%.The prevalence of respiratory symptoms varied between departments and among various sections of the company. Workers in spinning department had a higher prevalence of symptoms than workers in weaving department and percentage prevalence of respiratory symptoms was higher in blowing and carding sections of the spinning department and in loomshed or weaving section of weaving department.
This finding is in agreement with a study done in Nigeria, which reported spinning section had the highest frequency of symptoms, followed by weaving (Nagoda et al., 2012). Report by OSEJI et al. (2006) revealed a higher prevalence of respiratory symptoms among spinners compared to workers in other sections (OSEJI et al., 2006). Related study conducted in Akaki textile factory in Ethiopia, reported the prevalence of respiratory symptoms was high in the spinning department, in which 29.8% had cough, 24.4% had phlegm, 23.4% had chest tightness and 43.3% had dyspnea compared with the weaving department and the highest prevalence of respiratory symptoms (cough 77%, phlegm 62%, chest tightness 46% and dyspnea 62%) were found in the carding section (Alemu et al., 2010). Related study conducted in Bahir Dar Northern Ethiopia, reported that workers in the spinning section (Raza et al., 1999) and having respiratory symptoms in the spinning department was higher than in the weaving department (Ahasan et al., 2000).
The present study also showed the presence of high percentage prevalence of symptom complexes of chronic bronchitis such as chronic cough, chronic phlegm and chronic cough with phlegm to be 45, 41, and 41%, respectively and byssinosis (grade1/2 and grade1 were 12 and 29%, respectively) and dyspnea (grade 2) was 7.8% in exposed respondents. The result revealed the absence of symptom complexes of chronic bronchitis and byssinosis in non-exposed respondents. This finding is consistent with the study conducted in China, which showed a high prevalence of chronic cough (14%), chronic phlegm (13.6%) and byssinosis [grade1/2+1 (7.6%)] among the cotton textile workers than among the controls (Christiani et al., 1986). Khalifa et al. (2003) reported high prevalence of productive cough (40%), wheeze (46.25%) and dyspnea (28.75%) in exposed group than in controls. A study done by Abebe and Seboxa in Bahir Dar, Northern Ethiopia revealed that chronic cough was significantly higher among textile workers (Abebe and Seboxa, 1995).
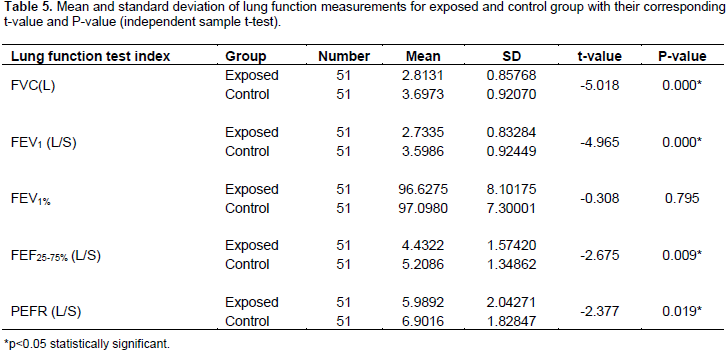
The result of the current study is also in agreement with a study conducted by Beck et al. (1982) in which 16% of the cotton mill workers developed symptom complexes of chronic bronchitis, as compared to only 1% of appropriate controls. Regarding pulmonary function, the mean values of lung function parameters such as, FVC, FEV1, FEV1%, PEFR and FEF25-75% of exposed group were lower than those of the control group. And the mean differences were found to be statistically significant (p=0.05), except FEV1% (p>0.05). FVC and FEV1 values across age ranges of 31-35, 41-45 and 46-50 years were greater in controls and the mean differences were statistically significant (P<0.05). Controls had greater mean FEV1 value than exposed subjects across 26 to 30 age category and the difference was statistically significant (P=0.029). FEV1% across the age category (21-25years) was low in exposed group, and the difference was statistically significant. PEFR and FEF25-75% values across 46 to 50 years age category were low in exposed group and the differences were statistically significant.
This finding is in line with the work of Nagoda et al. (2012) in Kano textile workers, Nigeria in which the mean values of PEFR, FVC, and FEV1 of exposed group were lower than those of the controls. Subjects exposed to cotton dust in this study showed decreased lung function compared to control group which is in agreement with the report of various related studies (Pragati and Aruna, 2016; Fishwick et al., 1996). Another studies revealed significantly decreased mean FEV1 and FVC in cotton workers which are in accordance with result of the present the study (Vyas, 2012; Bakirci et al., 2007). A study in Egypt showed a significant decline in FEF25-75% in exposed subjects compared to non-exposed subjects (Khalifa et al., 2003). Ibrahim and Alselevany (2008) reported that there was a statistically significant reduction of FVC and FEV1 in cotton textile workers in comparison with controls in all age groups above 40 years; which is in agreement with the current study.
A study by Dhanasree et al. (2014) reported that the overall mean values of lung function parameters like FVC, FEV1, FEV1%, PEFR and FEF25-75% were lower in workers exposed to cotton dust as compared to controls which is in accordance with the present study. The present study is also in agreement with the study done in Bahir Dar, Ethiopia, which reported the mean measured values of FEV1 and FVC were significantly reduced in the exposed group (Woldeyohannes et al., 1991). Pearson correlation analysis showed that there was a negative correlation between lung function measure-ments and duration of exposure, but it was not statistically significant. In the present study, the mean difference of lung function across different service years was found statistically insignificant. The result was found to be in agreement with a study conducted in Kano, Nigeria which showed no consistent variation in mean values of lung function parameters with duration of employment in the factory (Nagoda et al., 2012).
When respiratory passages are affected by various factors, they may lead to obstructive or restrictive air way diseases. Based on British Thoracic Society COPD Consortium and GOLD Spirometry guide, restrictive respiratory disease was observed among 20 (39.2%) and 3 (5.8%) of the exposed and control subjects, respectively and about 2% of the exposed study participants had obstructive respiratory disease (Bellamy et al., 2005; GOLD, 2010). Under normal condition, during a forced expiratory maneuver, at least 70% of the FVC should be expelled in the first second. In the presence of airway obstruction, FEV1 is affected more than the FVC and the ratio of FEV1/FVC is reduced below 70%. In case of lung volume restriction, both FVC and FEV1 values are lower than 80% of predicted value proportionally so that FEV1/FVC ratio is normal or exceed 70% (Hastings, 2003; Pellegrino et al., 2005). A study conducted in Nigeria found obstructive con-dition in 10 and 5.5% of the exposed and control group, respectively. It showed variation from the present study, this could be probably due to the presence of smokers. In a similar study, restrictive pattern based on FVC less than 80% of predicted value, with a normal FEV1/FVC was found in 80 (40%) workers in the exposed group and 10 (5%) in the control group (Nagoda et al., 2012) which is in accordance with the present study.
The prevalence of respiratory symptoms was found higher among workers exposed to cotton dust in textile factory. Exposure to cotton dust encountered in the factory environment was shown to reduce the overall mean values of lung function parameters like FVC, FEV1, FEV1%, PEFR and FEF25-75%. The study revealed an obstructive pattern in 2% of exposed workers on spirometry and a restrictive pattern in 39.2% of exposed workers. The duration of exposure was shown to have negative correlation with lung function among the exposed workers. The result of the study showed the absence of personal protective devices supply; due to this, workers in the manufacturing sections of the factory were performing their activity without using any PPDs.
This study shows the fact that cotton textile workers are highly vulnerable to occupational lung diseases. So, pre-ventive measures play indispensable role in minimizing minimizing the prevalence of respiratory disorders in cotton textile workers. Therefore, the factory management should provide PPDs to exposed employees and should provide additional protective measures like giving fresh milk to improve the wellbeing of workers and this in turn increase productivity of the factory. The factory management should also arrange training programs to exposed workers, focused on potential health effects of exposure to cotton dust, proper use and purpose of personal protective devices either by itself or in collaboration with concerned governmental and nongovernmental organizations. Concerned governmental bodies should instruct the employers to supply proper safety materials for their workers. It should also emphasize regular assessment on the factory environment. Provision of regular medical check-ups and maintaining proper ventilation aimed to improve the working conditions is highly recommended to the factory administration. Workers should take care of their own safety and health as much as they can while working in the manufacturing areas.
The authors have not declared any conflict of interests
The authors would like to thank Arba Minch Textile Factory staffs and all study participants for their valuable time and cooperation in providing the necessary information. The authors thank data collectors for the devotion and quality work during data collection. The work was funded by College of Health Sciences, Addis Ababa University.
REFERENCES
|
Abebe Y, Seboxa T (1995). Byssinosis and Other Respiratory Disorders among Textile Mill Workers in Bahir Dar, northwest Ethiopia. Ethiop. Med. J. 33:37-49.
|
|
|
|
Ahasan MR, Ahmad SA, Khan TP (2000). Occupational exposure and respiratory illness symptoms among textile industry workers in a developing country. Appl. Occup. Environ. Hygiene 15(3):313-320.
Crossref
|
|
|
|
|
Alemu K, Kumie A, Davey G (2010). Byssinosis and other respiratory symptoms among factory workers in Akaki textile factory, Ethiopia. Ethiop. J. Health Dev. 24(2).
Crossref
|
|
|
|
|
Bakirci N, Kalaca S, Francis H, Fletcher AM, Pickering CA, Tumerdam N, Cali S, Oldham L, Niven R (2007). Natural history and risk factors of early respiratory responses to exposure to cotton dust in newly exposed workers. J. Occup. Environ. Med. 49(8):853-861.
Crossref
|
|
|
|
|
Beck GJ, Schachter EN, Maunder LR, Schilling RSF (1982). A prospective study of chronic lung disease in cotton textile workers. Ann. Int. Med. 97:645-651.
Crossref
|
|
|
|
|
Bellamy D, Booker R, Connellan S, Halpin D (2005). Spirometry in practice. A practical guide to using spirometry in primary care. The British Thoracic Society (BTS) COPD Consortium.
|
|
|
|
|
Christiani DC, Eisen EA, Wegman DH, Ye TT, Lu PL, Gong ZC, Dai HL (1986). Respiratory disease in cotton textile workers in the People's Republic of China: I. Respiratory symptoms. Scand. J. Work Environ. Health 40-45.
Crossref
|
|
|
|
|
Christiani DC, Wang XR, Pan LD, Zhang HX, Sun BX, Dai H, Eisen EA, Wegman DH, Olenchock SA (2001). Longitudinal changes in pulmonary function and respiratory symptoms in cotton textile workers: a 15-yr follow-up study. Am. J. Respiratory Crit. Care Med. 163(4):847-853.
Crossref
|
|
|
|
|
Dhanasree Naidu, V.S Sai Sankalp Naidu, P.S. Sudheer Dwarak, P.S.Supriya Sree and N. Anu Deepthi (2014). Effect of Cotton Dust on Pulmonary Function among Cotton Textile Workers. MRIMS J. Health Sci. 2(2).
|
|
|
|
|
Ethiopian Textile Industry: Status and Growth Prospects (2013). Status and growth prospects of Ethiopian textile industry, LAP Lambert Academic Publishing.
|
|
|
|
|
Fantahun M, Abebe Y (2017). Self-reported disease conditions among workers of the textile mill in Bahir Dar, Northwest Ethiopia. Ethiop. J. Health Dev. (EJHD) 13(2).
|
|
|
|
|
Fishwick D, Fletcher AM, Pickering CA, Niven RM, Faragher EB (1996). Lung function in Lancashire cotton and man-made fibre spinning mill operatives. Occup. Environ. Med. 53(1):46-50.
Crossref
|
|
|
|
|
Ghasemkhani M, Kumashiro M, Rezaei M, Anvari AR, Mazloumi A, SadeghiPour HRG, Masaharu K, Mansour R, Ali R, Adel M, Hamid R (2006). Prevalence of respiratory symptoms among workers in industries of south Tehran, Iran. Industrial Health 44(2):218-224.
Crossref
|
|
|
|
|
Global Initiative for Chronic Obstructive Lung Disease (GOLD) (2010). Spirometry for health care providers. Available at:
View
|
|
|
|
|
Haglind P, Lundholm M, Rylander R (1981). Prevalence of byssinosis in Swedish cotton mills. Occup. Environ. Med. 38(2):138-143.
Crossref
|
|
|
|
|
Ibrahim MK, Alselevany BK (2008). Effect of cotton dust on lung functions. Ann. Coll. Med. Mosul. 34(2):141-147.
|
|
|
|
|
International Labor Organization (ILO) (1980). Occupational Exposure to Airborne Substances Harmful to Health, Geneva. Available at:
View
|
|
|
|
|
International Labor Organization (ILO) (2013). World Day for Safety and
|
|
|
|
|
Khalifa HO, Darwish K, El-Hady AA, El-Baset EA, EL-Deen RS, Mohamadein H (2003). Pulmonary function tests and respiratory symptoms among cotton ginning workers in Southern Egypt (SOHAG). AAMJ 1(2).
|
|
|
|
|
Kilburn KH (1998). Byssinosis and other diseases of textile workers. Environmental and occupational medicine. 3rd edn. Philadelphia: Lippincott-Raven Publishers pp. 449-55.
|
|
|
|
|
Mannino DM, Buist AS (2007). Global burden of COPD: Risk factors, prevalence, and future trends. Lancet 370(9589):765-773.
Crossref
|
|
|
|
|
Michael D (2004). Respiratory Diseases and Their Prevention. A Look at Industrial Dust and Its Control Facility Safety Management. Available at:
View
|
|
|
|
|
Nagoda M, Okpapi JU, Babashani M (2012). Assessment of respiratory symptoms and lung function among textile workers at Kano Textile Mills, Kano, Nigeria. Niger. J. Clin. Pract.15(4):373-379.
Crossref
|
|
|
|
|
Neil E, Chter S (2011). Respiratory effect and other disease patterns in textile industry. ILO Encyclopedia of Occupational Health & Safety. Geneva.
|
|
|
|
|
Oseji M, Isah EC, Osieogun A, Iyawe V (2006). Prevalence of byssinosis and other respiratory problems among textile mill workers in Asaba, Nigeria. Niger. Postgraduate Med. J. 13(4):333.
|
|
|
|
|
Oyejide OC (1989). Sample size determination in Oyejide OC ed Health research methods for developing country scientists. Ibadan Codat Publications. pp. 56-57.
|
|
|
|
|
Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi RE, Coates A, Van Der Grinten CP, Gustafsson P, Hankinson J, Jensen R (2005). Interpretative strategies for lung function tests. Eur. Respiratory J. 26(5):948-968.
Crossref
|
|
|
|
|
Pragati D, Aruna T (2016). Lung function among non-smoking cotton mill workers. Ind. J. App. Res.6.
|
|
|
|
|
Raza SN, Fletcher AM, Pickering CA, Niven RM, Faragher E (1999). Ventilatory function and personal breathing zone dust concentrations in Lancashire textile weavers. Occup. Environ. Med. 56(8):520-526.
Crossref
|
|
|
|
|
Simpson JC, Niven RM, Pickering CA, Fletcher AM, Oldham LA, Francis HM (1998). Prevalence and predictors of work related respiratory symptoms in workers exposed to organic dusts. Occup. Environ. Med. 55(10):668-672.
Crossref
|
|
|
|
|
Vyas S (2012). A study of pulmonary function tests in workers of different dust industries. Age (Years) 30(6.31):30-75.
|
|
|
|
|
Wang XR, Zhang HX, Sun BX, Dai HL, Hang JQ, Eisen EA, Wegman DH, Olenchock SA, Christiani DC (2005). A 20-year follow-up study on chronic respiratory effects of exposure to cotton dust. Eur. Respiratory J. 26(5):881-886.
Crossref
|
|
|
|
|
Woldeyohannes M, Bergevin Y, Mgeni AY, Theriault G (1991). Respiratory problems among cotton textile mill workers in Ethiopia. Occup. Environ. Med. 48(2):110-115.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2010). Report on Global Status of Non Communicable Diseases. Available at:
View
|
|
|
|
|
Zhong Y, Li D, Ma Q, Rylander R (2002). Lung function and symptoms among cotton workers and dropouts three years after the start of work. Int. J. Occup. Environ. Health 8(4):297-300.
Crossref
|
|