Full Length Research Paper

ABSTRACT
High maternal, neonatal and child mortality rate constituting about 70% of the population in Zimbabwe. Zimbabwean rural women have faced challenges in accessing and utilizing Maternal, Neonatal and Child Health (MNCH) services. Rural areas in Zimbabwe have had high prevalence of home deliveries and pregnancy related complications associated with lack of access to and utilization of MNCH services, resulting in high maternal, stillbirths, new-born, neonatal and infant mortality rates. Access to and utilisation of MNCH services and facilities by rural based pregnant women has been limited by several issues that have been explored and assessed in the Primary Health Care clinics. However, the 3 delays (seek, access and receive health service) effects on the factors affecting health care and outcomes remain largely unclear in rural settings. Qualitative and quantitative methods research was conducted in Mutare district, Manicaland Province, Zimbabwe. Data collection tools including interviews questionnaires and focus group discussion guides were used to show how the three delays affected health service access in the district. GraphPad InStat Software and Statistical Package for Social Science were used for data analysis. Religious and cultural beliefs contributed to patient delays in seeking healthcare. With long distances and lack of transport attributed to Delays 1 and 2 with, drug unavailability, up-to date equipment and delay causing Delay 3. The patient, the provider and health systems were critical in accessibility, utilization and linkages of MNCH with other health services being crucial for achieving 4th and 5th Millennium Development Goals the targets.
Key words: Maternal, Neonatal and Child Health Services, new-born; neonatal-infant mortality, three-delay model, Mutare District, child bearing Age.
Abbreviation: MNCH, Maternal, Neonatal and Child Health, MoHCC, Ministry of Health and Child Welfare; EmONC, Emergency Obstetric and Neonatal Care, PHC, Primary Health Clinic, WCBA, Women of Child Bearing Age.INTRODUCTION
Zimbabwe has endured rapid economic decline over the past decade that has dramatically reduced the socioeconomic and physical wellbeing of its 12 million inhabitants, of whom women and children comprise over 70% of the population (MoHCC, 2008). Manicaland districts of Chipinge, Mutare and Mutasa in Zimbabwe exhibit some of the country’s highest maternal and neonatal death rates, lowest institutional deliveries, and proliferation of faith groups that resist modern medicine (Plan international, 2012). Zimbabwe continues to address maternal and neonatal health challenges as reflected by several international agreements adopted, aimed at reducing maternal and neonatal mortality. The predecessor of Zimbabwean Nation, the Rhodesian Government, adopted the Primary Health Care (PHC) approach in 1978 which places emphasis on community participation. In 2000 and 2015, Zimbabwe adopted the Millennium Development Goals (MDGs) Declaration and Sustainable Development Goals respectively. One of the targets of these ambitious goals is to reduce maternal mortality ratio by three quarters and to reduce by two thirds the under-five mortality rate. Despite endorsing these goals, the scourge of maternal and child mortality continues to escalate.
Women of childbearing age (WCBA), ages from 15-49 years (Ngwenya et al., 2020). In rural areas, WBCA disproportionately face bigger challenges compared to their counterparts in urban settings in accessing and utilizing MNCH services. In most rural districts of Manicaland Province, early marriages and other religious-cultural practices have placed women and girls at health risk (Ncube et al., 2020). In addition, there is a high prevalence of home deliveries and pregnancy complications among rural areas dwellers. These are associated with lack of access to and utilization of MNCH services, which contribute to high maternal and neonatal and infant mortality in the nation. Infant Mortality Rate (IMR) is higher in rural areas due to disparities in access and quality of health care service (Ncube et al., 2020). Most childhood deaths occur in the neonatal period due to birth-related complications. Reports shows that at least 75% of neonatal deaths occur within the first week of life (MOHCC, 2009). Rural areas also presents with higher infant and child mortality rates (Nyereyemhuka et al., 2020). This observed maternal, neonatal, and infant deaths, to some extent emanate from several factors that affect the access and utilization of MNCH services in these rural areas (Nyereyemhuka et al., 2020).
Many of the factors contributing to maternal deaths are also responsible for new-born death. Good health and quality of life do not derive only from the health sector but are influenced by a myriad of other factors which are outside the health sectors’ direct control. All sectors of the economy impacted on the health and quality of life of all citizens through their direct influence on the social determinants of health (USAID, 2007). The health of mothers, new-borns, infants and children is essential for any society. A healthy mother gives birth to healthy infants who grow into adults with sound body and mind, live a productive life, and contribute to the family and society. Being the prime caregivers of children, mothers have the most significant impressionable effect on their children in the early developmental years (Worthman et al., 2016; National Academies of Sciences, Engineering, and Medicine, 2016).
The future health of a society depends on the health of the children of today and their mothers, who are guardians of their future. If physically and mentally healthy, women can steer their children and the family towards prosperity and long-lasting happiness. Poor maternal health can have a significant negative impact on the family and society as it is a major determinant of the health of children and indirectly affects the formation of human capital (Mattoo et al., 2020). Developed societies place great emphasis on the health care and gender equity of mothers, new-borns and children (Sen, 2019). Therefore, investigating the accessibility to and utilization of MNCH services by rural women is essential for determining the execution of health promotion programs, teaching and education of women on Women and Child Health, planning for resources allocation, advocating for future developmental projects resource allocation and determining lines of interaction necessary with women in general. Nevertheless, infant mortality rate for Zimbabwe was 38.4 deaths per 1,000 live births in 2019 which is gradual decrease from 72.7 deaths per 1,000 live births in 1970 attributable mostly to possible improved access to health care (KNOEMA, 2020).
Whilst there are organizations, including the Government, allocating a lot of resources into MNCH, there remains a scarcity of information on what really happens to women on the ground and how they access the much-needed services and their own views and interpretations of programs rolled out to assist them (Sen, 2019). Exploring and assessing how rural women’s health requirements are accessible to them is an ongoing process. As society devolves, the spectrum and quality of needs permutate, generational and cultural practices evolve and blend in new characteristics losing older beliefs. This necessitates continuous appraisals of systems, processes, knowledge, beliefs and perceptions that inform the perpetuation of the sub-community on which the future of the nation is inexorably hinged to in whom a high burden of high maternal, neonatal and child mortality exists. The study sought to explore the extent to which three main delays associated with access and utilization MNCH services by rural women, that is, challenges that women face with recognizing danger signs and making a decision to seek proper recommended health care; challenges in reaching the health facility concerned and challenges of women receiving appropriate care at the health facility.
MATERIALS AND METHODS
Area of study
Mutare district in Manicaland province is situated in the North Eastern Zimbabwe. Mutare is the fourth largest city in Zimbabwe, with a population of around 170,000 and is the capital city of Manicaland province, where women constitute about 52% of the population. The major livelihood of people living in the rural areas of Mutare district include: trading of agricultural produce, horticulture and fruits, farming, and in some areas, dairy farming (Plan international, 2012).
Randomly selected PHC on which the study was conducted include Muromo, Bakorenhema, Zvipiripiri and Marange clinics in Mutare District. The catchment of each health centre comprised of the population in the surrounding areas of the health centre who receive a direct service from the PHC. The main sources of primary data for this study were the rural pregnant women and those women that had given birth within two years of the time of study and representatives from Plan International. The main sources of secondary data were the Ministry of Health and Child Care (MoHCW) officials and Maternal and Child Health Integrated Programme (MCHIP) health coordinators. This research was based on a case study on Mutare district clinics and their catchment areas where four clinics were randomly selected from a total of 42 rural clinics in the district. The aim of the study was to assess factors associated with accessibility and utilization of health services by rural communities.
The research setting, data collection, analysis and interpretation was based on the 3 delays to access model mainly: deciding to seek care, reaching the healthcare facility receiving care, all aspects that may improve with increases access to health facilities (Mgawadere et al., 2017; Pacagnella et al., 2012; Ngoma-Hazemba et al., 2019).
Interviews and direct observations were used to collect data for the study. Four types of interviews were used in the research. These were household interviews with pregnant women (or women who delivered at most a year before the study), focus group discussion interviews, key informant interviews and interviews with health personnel during the health facility assessment. The household questionnaire (collected quantitative data). Household demographics were examined to determine how they affected access to healthcare using the 3 delays model. Focus group discussion guide (collected qualitative data) seeking to find how the access to medical facilities improved outcomes in infant health while the health facility assessment questionnaire evaluated the suitability of these may affect accessibility of health care according to the 3 delays model.
Key informant interview questionnaire was developed and used in the study to evaluate specialist knowledge and input in the healthcare system in its ability to deliver accessibility to health facilities in the district. Direct observations were also used during the interview process for household, key informant interviews and focus group discussions. Observations were also done during the interviews for health facility assessments (where tours of each of the health facilities were conducted to assess the capacity of the clinics in terms of infrastructure, medical drugs and equipment in relation to provision of MNCH services).
Interviews for this study were conducted with individuals and with groups, which are characterised by Mikklesen (2005: 179) as: individual interviews, key informant interviews and Group Interviews (Mikklesen, 2005). Respondents included pregnant women and health personnel during the health facility assessment. Key informant interviews were conducted with the aim of obtaining special knowledge on a given topic from MoHCC personnel and health coordinators for Non-Governmental Organisation (NGO) implementing MNCH related projects in Mutare such as Plan international and MCHIP. Focus Group Discussions (FDG) provided access to a larger body of knowledge and were undertaken under minimum guidance of a facilitator with pregnant women or women that had delivered within a year of the time of study (to minimise recall bias). The focus group discussions were done with each group having not more than 12 women to enable good group control and allow all women to participate fully in the discussion (Arntsen and Waldrop, 2018). Focus groups were likely to create severe issues of external validity, especially where the reactive effects of the testing arrangement probed the perceptions, opinions, beliefs, and attitudes towards the service.
Eight FDGs were conducted with two for each clinic catchment area. The FDGs were conducted in the community in an informal set up so that all respondents would feel free to participate. The women were made to sit in a U-shape with the facilitator guiding the discussion and two note takers sitting among the women. The facilitator ensured that all women participated fully and dominators were controlled. Two note-takers were used to ensure all the information discussed by the women was recorded. What one note-taker might have missed would be taken note of by the other. The FDGs were conducted in vernacular to ensure all women had a full understanding of the issues under discussion. The FDGs were kept short so that the respondents remained focussed.
Pretesting of data collection
Prior to any data collection, the pretesting of tools was undertaken to minimise ambiguity. After pretesting of data collection tools, tools were revised and data collection in the field was commenced, in a systematic or well-planned manner.
Sample size for data collection
The sample size used was 10% of the population of pregnant women in the catchment areas of the randomly selected clinics which was shown statistically to be working estimate of the population in the district. The breakdown for each clinic in terms of number of household interviews conducted, key informant interviews and health facility assessment interviews conducted was given under results (Table 2).
Time frame and approach to data collection
The field research entailed the following: household questionnaires, key informant interviews and health facility assessments at the selected clinics. The data collection was conducted over a two-week period through the use of questionnaires and guided interviews.
Analysis framework
Data analysis was descriptive where the survey provided primary data that were collected in the catchment areas of the four selected health centres in Mutare district using questionnaires to collect qualitative and quantitative data using both open ended and closed ended questions and guided interviews to collect specifically qualitative data.
Research assistances
The research assistants engaged exhibited excellent communication skills, good knowledge of English and the local language of the area of study, a perceptive intelligence, inexhaustible patience, unfailing dependability and ability to get along with members of the local population (Devereux and Hoddinott, 1992). Three female research assistants fluent in Shona the prevailing local languages in the target area of the study. The female research assistants were deliberately selected since the study participants were primarily female, and this ensured that the study participants would freely open up confidential issues.
Study target population
The target study population comprised of pregnant women or women who gave birth or miscarried less than a year from the time of the study, health workers and key informants who reside in the catchment area of the study clinics.
Unit of analysis
The units of analysis were the health centres and their catchment area which created an explanatory order of the units and explained differences among them.
Sampling
The study employed the probability sampling that allocated equal chances of selection for each respondent and removed the element of bias in respondent selection. Thus, simple random sampling and cluster sampling approaches were adopted for this study. The clusters were defined as the catchment areas of the selected four healthcare centres where the study women and health workers of the clinics were interviewed. The catchment area was defined as the area surrounding a health centre, and was not restricted to the village as a health centre served several villages or wards or part ward depending on the location of the healthcare centre. The general norm was that one visits the health centre closest to them, but in reality, other considerations came into play such as the level of skill of health workers at the closest health centre, user fees, distance, the availability of drugs, equipment and previous treatment experience at a centre (Furusa and Coleman, 2018).
Random sampling
Simple random sampling was used in the selection of the four out of 42 rural clinics in Mutare district that were selected for the study. These comprised approximately 10% of the total number of rural clinics (Westfall, 2008). On these four selected clinics, health facility assessments were conducted to assess the capacity of the health centres in terms of health workers skill, availability of equipment, drugs and status of the infrastructure used for the provision of MNCH services. The selection of the specific women who were interviewed on access and utilization of MNCH services was by cluster sampling.
Cluster sampling
Block sampling was used where the population to be sampled was divided into clusters, which were heterogeneous to match the community (Westfall, 2008). A random sample was drawn from within the selected clusters, which comprised people living in the catchment areas of the healthcare centre, regardless of village or ward demarcations.
Data analysis and presentation
Qualitative data was analysed through establishing themes where possible. For quantitative data, Statistical comparisons were performed analysis of variance (ANOVA) followed by Tukey's Multiple Comparison Test. Where necessary the One Sample t test was used as a test for discrepancy between parameters. Percentage means of groups were compared for relative and comparative differences, which were considered statistically varied when P < 0.05. Analysis of data used GraphPad InStat Software (version 5, GraphPad Software, San Diego, California USA) as well as IBM SPSS Statistics 26.0 (IBM SPSS Statistics, Chicago, USA).
Reliability and validity issues
Reliability relates to the consistency of data collected (Kothari, 1985) and all research assistants were thoroughly trained prior to data collection to ensure a level of accuracy, consistency and completeness of questionnaires throughout data collection. Focus group discussions were facilitated by the researchers and two note takers to ensure a high level of quality, validity and reliability during the process. Some women of childbearing age (15-49years) may have challenges of recalling their experiences during pregnancy and childbirth that may have occurred more than 3 years ago. To ensure more accurate data, the study endeavoured to focus on interviewing pregnant women and those who had given birth or had had miscarriages in a period of at most 1 year. Literacy levels in rural areas are not consistent in all the clusters. Regardless of Zimbabwe’s high literacy rate (92%), some rural women would have dropped out of school during or immediately after completing the primary level of education due to poverty or lack of parental support (Plan international, 2012). Therefore, to ensure that every woman had a clear understanding of the questions asked during the interviews, the questionnaires were administered in vernacular- Shona and Ndebele languages. The Cronbach’s alpha values were determined for the questionnaires to check for their internal consistency reliability.
Ethical considerations
In this study, each respondent gave written informed consent. Furthermore, as per traditional norms, permission was sought from the village heads prior to entering their areas of jurisdiction, and sensitization was done at the District Administration (DA) offices and MoHCC District offices, prior to the commencement of the data collection process.
RESULTS
Causes of constraints to accessibility to and utilization of Maternal Neonatal and Child Health (MNCH) services in the Mutare District findings included those that were related to population demographics and characteristics, factors causing Delay 1, factors that cause Delay 2, factors that cause Delays 3, health facility related findings and rural women perspectives on health delivery. The research findings were categorised using the conceptual framework of the ‘Three delay Model’ proposed by D. Maine. Key findings were that, religious and cultural beliefs greatly contributed to the initial delay (delay in seeking care) in this community. Long distances and lack of transport attributed to the second delay (delay in reaching health care) and unavailability of drugs and up-to-date equipment contributed to the third delay (delay in receiving treatment at the centre).
Demographic data of the overall target population
Secondary data collected from MoHCC Provincial Information Office on demographics of the target population has been presented in Table 1. While females are the majority, only 46.2% were of childbearing age, whereas all of the adult males are of reproductive age. Apostolic Faith believers constitute approximately 44.5% of the population. This also reduces the utilisation of health facilities unless the beliefs of this group changes.
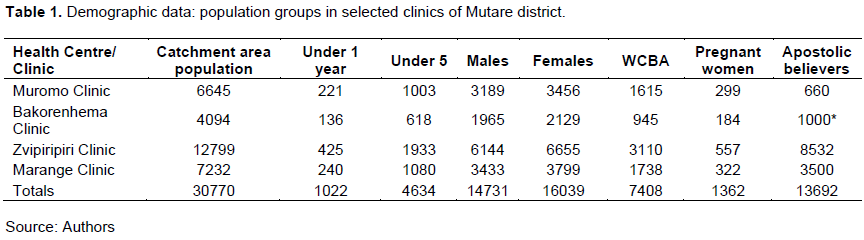
Demographic data were examined for balance and bias between clinics. The sample demographic data was evenly distributed amongst the clinics that were selected for the study. One-way analysis of variance (ANOVA) showed a P = 0.0503, F =3.003, R squared = 0.2729. The Bartlett's test for equal variances gave a corrected Bartlett statistic of 11.20, indicating that the variances were equal amongst the different clinic samples (*P < 0.0107). However, the Tukey's Multiple Comparison Test for Bakorenhema Clinic vs Zvipiripiri Clinic showed a significant difference in the whole sample distribution (*P <0.05, Mean Diff = -2911, q = 3.963, 95% CI of diff -5777 to -45.27) while the other comparative relationships did not show any significant differences (Table 1).
The catchment area for Zvipiripiri clinic (12799 people) was the largest relative to the other clinics. This area also had the highest population (67%) of apostolic faith believers (AFBs) who rely on alternative medicine and spiritual approaches to healing, and neither visit health care centres nor allow child immunization. The AFBs practice polygamy- and their households were often found to have more children (>5). Marange clinic also had a relatively high proportion of AFBs (48%) in its catchment area (Table 1).
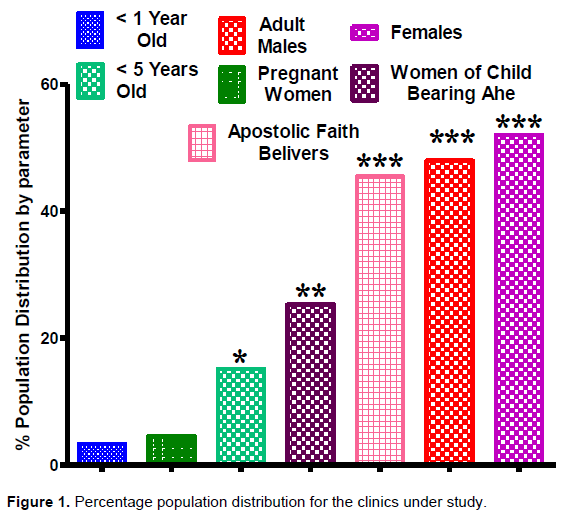
One-way ANOVA of the population demographics of selected clinics showed a significantly different distribution (***P < 0.0001, F = 1308, R squared = 0.9982) showing that that the variables were independent. Tukey's Multiple Comparison Test for < 1 Year Olds vs < 5 Years Olds was significantly different (***P < 0.05, Mean diff = -11.78, q = 20.40, 95% CI of diff -14.57 to -8.992), for < 1 Year Old vs Adult Males (***P < 0.05, Mean diff = -44.68, q = 77.39, 95% CI of diff -47.47 to -41.89), for < 5 Years Old vs Females (***P < 0.05, Mean diff = -36.90, q = 63.91, 95% CI of diff -39.69 to -34.11) for < 5 Years Old vs Apostolic Faith Believers (***P < 0.001, Mean diff -30.40, q = 52.65, 95% CI of diff -33.19 to -27.61) for Adult Males vs Pregnant Women (***P < 0.05, Mean diff = 43.50, q = 75.34, 95% CI of diff 40.71 to 46.29), for Pregnant Women vs Apostolic Faith Believers (***P < 0.05, Mean diff = -41.00, q = 71.01, 95% CI of diff "-43.79 to -38.21). Children < 5 years of age formulated relatively smallest proportion in the households as compared to women of childbearing age. There were twice as many females as compared to the WCBA. The % of children < 5years were more than twice the proportion of either children < 1year or the pregnant women. %WCBA were half the total % females (Figure 1).
Factors contributing to Delay 1- (delay in decision to seek health care)
Household demographics and characteristics of sampled households
Sampled household characteristics were seen as enablers or obstructers to accessibility and utilization of health services. The average age of the household heads was 47 years, with a range of 18-94 years. In all the four study clusters (catchment areas of clinics), over three-quarters of the household heads were found to be married and those who were widowed. Household heads were distributed as 74% males and 26% females. Adverse effects of males headed-households was directing of household income to extraneous issues away from the family needs, thus delaying decisions and processes to seek health services by family members.
From the FGDs some women (about 40%) stated that they have to request permission prior to seeking health care whether for themselves or for their children. One woman in Bakorenhema catchment area stated “ini ndakamborambidzwa kuyenda kukliniki nemurume wangu nokuthi ayida kushandisa mari yacho kutenga doro”. Translated to mean, “I was once not given permission to go to the clinic, as my husband wanted to use the money, he had to buy beer”. The study found that the average household size of the sampled houses was 6 people. On average the sampled households had at least 2 children under the age of 5 years and of which one child was under 12 months. About 54% of mothers’ or caregivers’ ages mainly fell within the 21-34 years age range and (18.9%) were in the 35-49 years age range. From survey findings, (10.6%) of children had lost their biological mothers at the time of the study.
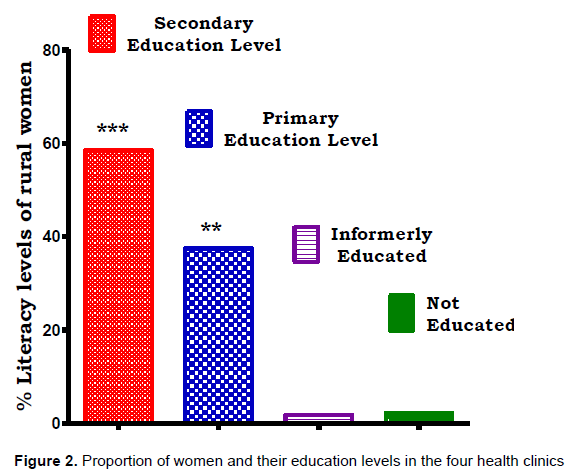
Literacy levels of rural women attending of health services
Rural women literacy level was used as a marker of facilitation to accessibility and utilization of health services for this subpopulation. More than half of the mothers (59.5%) had completed secondary school education and (37.5%) had received only primary school education. Only (1.9%) had never received any formal education whilst (1.2%) were informally educated. Women who had attained secondary level education were overly represented in the households interviewed compared to those who had attained primary level education and those who had either received informal education or received no formal education at all. Those women who had attained primary level education were relatively more represented as compared to those who were formerly or not educated at all. One-way analysis of variance (ANOVA) of women groups from the four clinics showed significantly different frequencies by educational levels (***P < 0.0001, F = 2544, R squared = 0.9990). Moreover, Tukey's Multiple Comparison Test for Secondary Education vs Primary Education Levels showed significant variation (***P < 0.05, Mean diff =21.00, q = 37.99, 95% CI of diff 18.50 to 23.50), for Secondary Education Level vs Informally Educated (***P < 0.05, Mean diff = 56.63, q = 102.5, 95% CI of diff 54.13 to 59.14), for Secondary Education Level vs Not Educated (***P < 0.05, Mean diff = 56.27, q = 101.8, 53.76 to 58.77, for Primary Education Level vs Informally Educated (***P < 0.005, Mean diff = 35.63, q = 64.46, 95% CI of diff 33.13 to 38.14) and for Primary Education Level vs Not Educated (***P < 0.05, Mean diff = 35.27, q = 63.80, 95% CI of diff 32.76 to 37.77) (Figure 2).
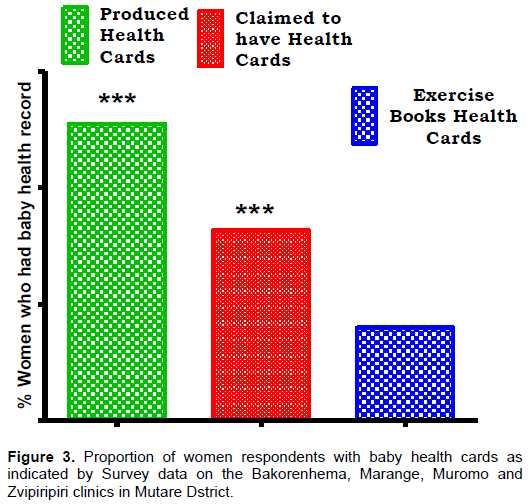
Presence of a health card for infants
A baby health card was used as a surrogate indicator for access to health service for both mother and baby. Women with baby health cards were 3.19-fold more when compared to those using exercise books as baby health cards and 1.54-fold more than those who claimed to have baby cards. The proportion of women who did not produce baby cards but claimed to have them was twice as much as those who used exercise books for baby health cards. Women with baby health cards were 3.19-fold more when compared to those who were using exercise books as baby health cards and 1.54-fold more than those who claimed to have baby cards. One-way ANOVA of the proportion of women and possession of baby healthy cards revealed a significant difference of the groups (***P < 0.0001, F = 1182, R squared = 0.9975). Furthermore, Tukey's Multiple Comparison Test showed significantly differences for group who Produced Health Cards vs Claimed to have Health Cards (***P < 0.05, Mean diff = 18.33, q = 36.01, 95% CI of diff 16.12 to 20.54), for group who Produced Health Cards vs who Exercise Books Health Cards (***P < 0.05, Mean diff 35.00, q = 68.74, 95% CI of diff 32.79 to 37.21) and for group who Claimed to have Health Cards vs Exercise Books Health Cards (***P < 0.05, Mean diff = 16.67, q = 32.73, 95% CI of diff 14.46 to 18.88) (Figure 3).
Baby weights as indicators of accessibility to health services
Baby weights at birth was used to identify features of underweight associated with reduced accessibility and utilization of health services. The survey findings indicated that children on average weighed 3.1kgs at birth. Of the interviewed households (12%) of the children were not weighed at birth because they were delivered at home and some of these mothers only took their babies to the clinics some months after delivery when their child had developed an illness which could not be handled by alternative approaches.
Immunization of infants as indicators of accessibility and utilization of health service
In the surveyed clinics’ catchment areas, 33.8% of children had been fully immunized. About 56.5% of children still had to complete their immunization. The children below <18 months had received BCG, DPT 1 Polio 1, DPT2 Polio 2 and DPT3 Polio 3 vaccines but were still to receive the DPT and Polio vaccine at 18 months to complete their primary immunization course. About 9.7% were not fully immunized at all for reasons of religious connotations.
Immunization status indicated accessibility and utilization of health services. Generally, children were partially immunized all round. In Bakorenhema partially immunized children were relatively over represented as compared to the fully immunized or the not immunized children. In Marange partially immunized children were relatively over represented as compared to the fully immunized or the not immunized. A similar pattern was seen in Muromo and notable was the near absence on the not immunized proportion in this area (Figure 4).
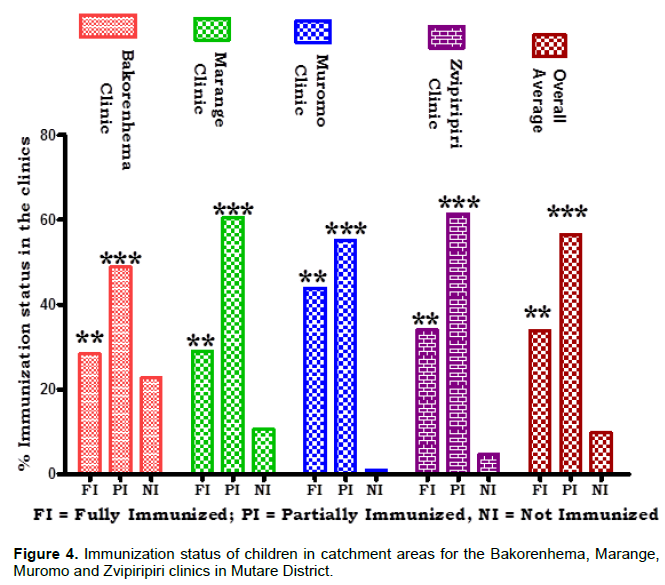
In Zvipiripiri the partially immunized were overly represented when compared to the fully or not immunized. The overall average immunization status resembled closely the immunization pattern shown in Marange. Bakorenhema and Marange showed in increased tendency towards children who were not immunized, 22.7 and 10.5%, respectively. Religious beliefs of the Johane Marange Apostolic Faith seemed to influence the former areas against immunization and visit the clinic for any form of treatment.
Two-way ANOVA showed a % of total variation percentage of 62.10% for immunization status amongst the clinics which was significantly varied (***P < 0.0001, Df = 2, Sum-of-squares = 9126, Mean square = 4563, F = 5196). The Bonferroni posthoc t-test comparing Bakorenhema Clinic vs Marange Clinic showed a significant difference amongst the clinics for the partial immunization (PI) status groups (***P < 0.001, Difference = 11.70, t = 8.828, 95% CI of diff 6.807 to 16.59) and for no immunization (NI) groups (***P < 0.001, Diff = -12.20, t = 9.206, 95% CI of diff -17.09 to -7.307). There was a significant difference when Bonferroni post hoc-test was used to compare Bakorenhema Clinic vs Muromo Clinic among the fully immunized (NI) group (***P < 0.001, Diff = 15.50, t = 14.32, 95% CI of diff 11.50 to 19.50), for the PI group (***P <0/001, Diff 6.200, t = 5.730, 2.205 to 10.20), for the NI group (***P < 0.001, Diff -21.70, t = 20.05, 95% CI of diff -25.70 to -17.70). For the comparison Bakorenhema Clinic vs Zvipiripiri Clinic, the Bonferroni post-test showed a significant variation for FI; PI; NI (***P <0.001, Diff = 5.600, t = 5.175, 95% CI of diff 1.605 to 9.595; Diff = 12.50, t = 11.55, 95% CI of diff 8.505 to 16.50; Diff -18.10, t = 16.73, 95% CI of diff, respectively). Bakorenhema Clinic vs Overall Average was also significantly different for FI: PI; NI (***P < 0.001, Diff = 5.400, t = 4.990, 95% CI of diff 1.405 to 9.395; Diff = 7.600, t = 7.024, 95% CI of diff 3.605 to 11.60; Diff = -12.97, t = 11.98, 95% CI of diff -16.96 to -8.971, respectively). Marange Clinic vs Muromo Clinic, Marange Clinic vs Zvipiripiri Clinic, Marange Clinic vs Overall Average, Muromo Clinic vs Zvipiripiri Clinic, Muromo Clinic vs Overall Average and Zvipiripiri Clinic vs Overall Average showed significantly different PI, FI, and NI distributions with the exception of the FI for Zvipiripiri Clinic vs Overall Average and PI for Muromo Clinic vs Overall Average.
Factors that contribute to Delay 2- (delay in reaching care)
The second delay covered the time needed for a rural woman or infant to reach the health centre or a trained health service provider, once a decision had been made to seek proper health care. The major factors found in this study that contributed to this delay were the distance travelled to the nearest clinic and the mode of transport used to reach it.
Distance travelled to nearest health centre
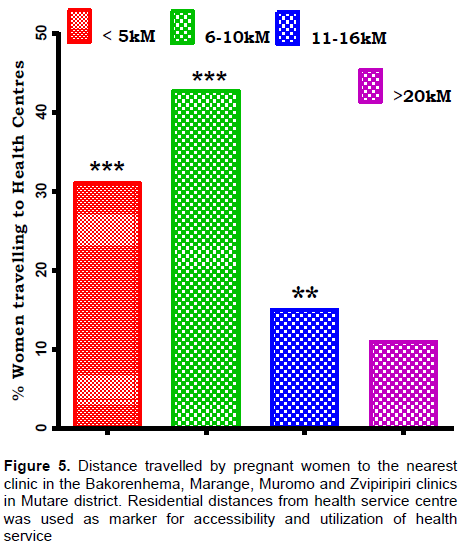
Figure 5 shows the distances travelled by women to the nearest clinic. Women who lived between 6-10kM away from the nearest healthcare facility were relatively over represented when compared to those who lived <5km, 11- 16kM 16kM and >20kM 20kM The %women who lived <5kM from the nearest clinic were relatively higher when compared to those who lived 11-16kM 16kM and >20kM, respectively, from the nearest health clinic Overall, over 50% of the pregnant women lived beyond the recommended distance of 8kM from the nearest health centre in any district. The proportion of people and distance travelled to health Centre was statistically significantly different (***P < 0.0001, F = 772.9, R squared = 0.9966). The Tukey's Multiple Comparison Test showed significant differences between < 5kM vs 6-10kM (***P < 0.001, Diff = -11.67, q = 22.14, 95% CI of diff -14.05 to -9.280), between < 5kM vs 11-16kM (***P < 0.0001, Diff = 16.00, q = 30.36, 95% CI of diff 13.61 to 18.39), between < 5kM vs >20kM (***P < 0.0001, Mean diff = 20.00, q = 37.95, 95% CI of diff 17.61 to 22.39), 6-10kM vs 11-16kM (***P < 0.0001, Mean diff = 27.67, q = 52.49, 95% CI of diff 25.28 to 30.05), between 6-10kM vs >20kM (***P < 0.0001, Mean diff = 31.67, q = 60.08, 95% CI of diff 29.28 to 34.05) and between 11-16kM vs >20kM (***P < 0.0001, Mean diff = 4.000, q = 7.589, 95% CI of diff 1.613 to 6.387).
Mode of transport used to reach health centres
On further questioning concerning travelling to their nearest health centres, the women revealed the modes of transport they used to travel to their nearest health centres. The results have been graphically presented in Figure 6.
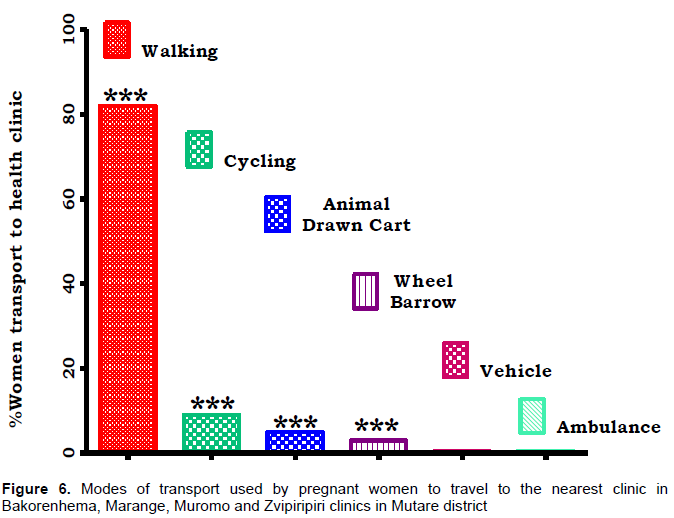
Mode of transport to health facility was used as an indicator to accessibility and utilization of health services for the study population. Walking as a mode of transport was relatively over represented as compared to cycling, animal drawn cartage, wheel barrow use, vehicle or ambulance use. Use of the a vehicle or use of an ambulance were the rarest means of transport to a health facility for the rural women. One-way ANOVA of frequency a particular mode of transport was used to compare access and utilization of health facility and significantly differences were observed amongst the study population (***P < 0.0001, F =772.9, R squared = 0.9966). Tukey's Multiple Comparison Test was extremly significant for < 5kM vs 6-10kM (***P < 0.05, Mean diff = -11.67, q = 22.14, 95% CI of diff -14.05 to -9.280), for < 5kM vs 11-16kM (***P < 0.05, Mean diff = 16.00, q = 30.36, 95% CI of diff 13.61 to 18.39), for < 5kM vs >20kM (***P < 0.05, Mean diff = 20.00, q = 37.95, 95% CI of diff 17.61 to 22.39), for 6-10kM vs 11-16kM (***P <0.05, Mean diff = 27.67, q = 52.49, 95% CI of diff 25.28 to 30.05), for 6-10kM vs >20kM (***P < 0.05, Mean diff = 31.67, q = 60.08, 95% CI of diff 29.28 to 34.05) and significant for 11-16kM vs >20kM (**P < 0.05, Mean diff = 4.000, q = 7.589, 95% CI of diff 1.613 to 6.387) (Figure 6).
Most rural women walk, some due to poverty, some due to the fact that in rural areas there are no fully established road networks, nor do many people own bicycles, let alone motor vehicles. A woman from Muromo explained that “if a pregnant woman was unable to walk the family would hire an animal drawn cart to ferry her to the clinic but if they could not afford it, they would have to be ferried i her in a wheel barrow”
Factors that contribute to Delay 3- (delay in receiving treatment /health care)
The Third Delay looked at receipt of appropriate and effective treatment at the healthcare centre once the preceding challenges had been overcome. The study revealed findings on the proportion of women that delivered at home and reasons given by the respondents.
Place of delivery for pregnant women
The place of delivery was assessed in order to determine the proportion of women that had delivered at a health centre or at home with the latter being an indirect indicator of the inaccessibility od health services indirectly. Figure 8 shows results on the place of delivery. Further extrapolation of research data to triangulate these results was done through the use of qualitative data from the FDGs. A woman from Marange stated that “isu hatizvariri kuchipatara, nokthi tiinotevedzera church yedu” when translated means “we do not deliver our babies in health care facilities because our church does not allow that,”. Another woman from Zvipiripire said “mhepo dzekumusha dzinoda kuti mhunhu azvare achishandirwa” translated to mean “our ancestors require us to give birth according to our customs therefore we do not encourage our women to go to the clinic”.
Place of birth was analysed to see if the it was influential to accessibility and utilization of health services by rural women. On analysing data on % likelihood of one giving birth at home or at the clinic, the question asked was whether place of birth did have the same effect at all values of clinic or home. Interaction between variables accounted for 99.79% of the total variance and was considered to be extremely significant (***P < 0.001, F = 2554.67, DFn = 3, DFd = 8). As the interaction was statistically significant, the P values that f were obtained for the row and column effects were difficult to interpret. On examining whether a particular clinic or home delivery affected the results, it was found that indeed, clinic or home delivery accounted for 0.10% total variance and thus considered significant (*P = 0.022, F = 8.00, DFn = 1, DFd = 8).
Women from Bakorenhema and Muromo areas showed relatively higher tendencies for giving birth at home and at the clinic, respectively. In Marange and Zvipiripiri areas there was an inverse relationship between attendance to give birth at the clinic or at home (Figure 7). Additional information given by a MoHCC official was that:
“most women delivered their babies at home because of a number of reasons such as: their belief that when they have received prayers from faith healers they deliver without complications; the clinic at times refers the pregnant women to far away hospitals but Ambuya (traditional birth attendant) does not usually refer patients, and Ambuya does not ignore mothers or mistreat them but at the clinic health workers (nurses) usually follow hours especially when their supervisors are not around, or may sometimes delay waking up if the woman comes late in the night”.
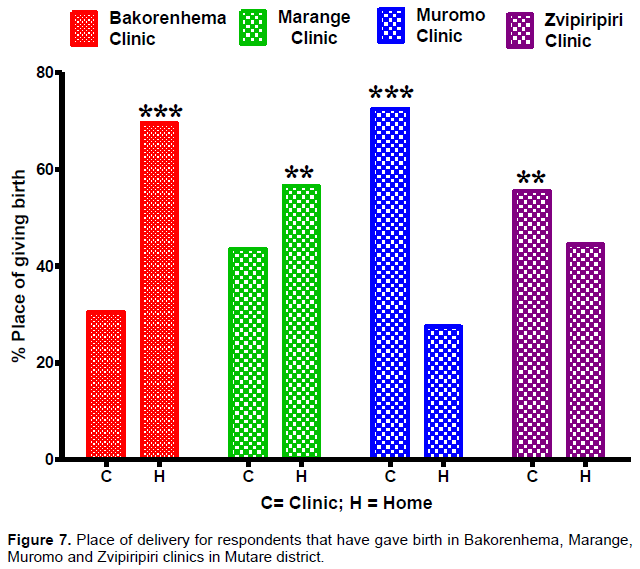
Those women who delivered at home, that is, 31.6% of the mothers, said that a traditional trained birth attendant was present at their time of delivery, 53.7% of the mothers indicated that an untrained traditional birth attendant was present and only 14.7% said that a skilled birth attendant was present at the time of delivery. However, the Bonferroni post-tests comparing the likelihood of a woman giving birth at a clinic or home showed a significant variance forBakorenhema Clinic vs Marange Clinic for home delivery (***P < 0.001, Diff = -13.00, 95% CI of diff = -15.80 to -10.20, t = 18.38), for Bakorenhema Clinic vs Muromo Clinic (***P < 0.001, Diff = -42.00, 95% CI of diff = -44.80 to -39.20, t = 59.40), for Bakorenhema Clinic vs Zvipiripiri Clinic (***P < 0.001, Diff = -25.00, 95% CI of diff = -27.80 to -22.20, t = 35.36), for Marange Clinic vs Muromo Clinic (***P < 0.001, Diff = -29.00, 95% CI of diff = -31.80 to -26.20, t = 41.01), for Marange Clinic vs Zvipiripiri Clinic (***P < 0.001, Diff = -12.00, 95% CI of diff = -14.80 to -9.199, t = 16.97) and for Muromo Clinic vs Zvipiripiri Clinic there was a bias towards the clinics as birth place (***P < 0.001, Diff = -17.00, 95% CI of diff = -19.80 to -14.20, t = 24.04) (Figure 7).
First point of contact when an infant or pregnant woman is sick
Women were then asked who their first contact was when their child got sick. The following results were obtained and presented in Figure 8. Figure 8 depicts the first point of contact of a sick infant or pregnant woman in Bakorenhema, Marange, Muromo and Zvipiripiri clinics in Mutare district. The first point of call for the study population emphasized the accessibility and utilization of conventional health services as compared to alternative medicine practitioners. A Two-way ANOVA for the “First point of Contact” for health service was more dependent on the type of health service provider in all the areas rather than on the area where the facility was situated with an extremely significant interaction as source of variation (***P < 0.001, % source of variation = 26.34, Df = 12, Sum-of-squares = 2557, Mean square = 213.1, F = 568.1) and Type of health service provider as source variation being also extremely significant (***P < 0.0001, % of total variation = 73.58, Df = 4, Sum-of-squares = 7142, Mean square = 1786, F = 4762). The Bonferroni post-tests for Bakorenhema Area vs Marange Area showed that the preference for type of health service was extremely significant different for VHW in the two areas (***P < 0.0001, Diff = -6.00, t = 9.798, 95% CI of diff -8.040 to -3.960), for NNA (***P < 0.0001, Diff = 11.00, t = 17.96, 95% CI of diff 8.960 to 13.04), for FSH (***P < 0.001, Diff = -11.00, t = 17.96, 95% CI of diff -13.04 to -8.960), for TH (***P < 0.001, Diff = 5.000, t = 8.165, 95% CI of diff 2.960 to 7.040). The preference for type of health service provider was considered extremely significant for Bakorenhema Area vs Muromo Area and Bakorenhema Area vs Zvipiripiri Area in that the area of health facility did not have the same effect at all values of the Type of health service.
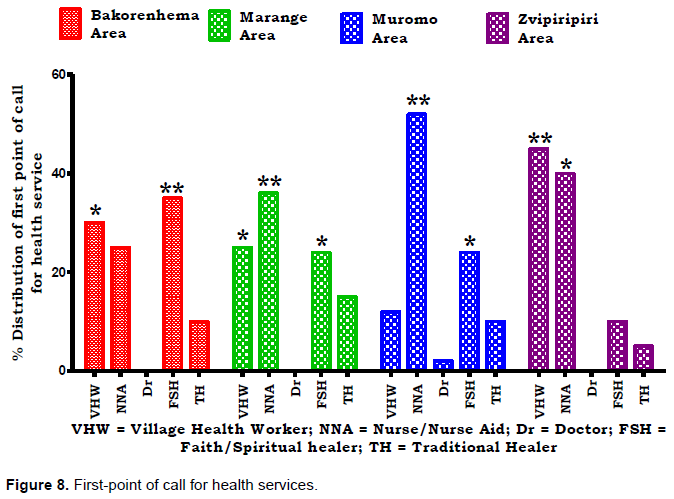
In Bakorenhema the most popular point of call for an infant or pregnant women consultation was the Faith-Spiritual Healer as compared to the village health worker or nurse-nurse aid or traditional healer. The nurse-nurse aid was the most common first point of call for infants and pregnant women in the Marange as in Muromo area as compared to either village health worker or Doctor or faith-spiritual healer or traditional healer. The village health worker was the most consulted for the infant of pregnant women problems in Zvipiripiri area as compared to either nurse-nurse aid or doctor or faith-spiritual healer or traditional healer. The traditional healer was the least to be called on when an infant or pregnant woman needed to consult in all areas with the medical doctor being only consulted 2% of the time in Muromo area.
Patients satisfaction/dissatisfaction of health services received
An average of 47% of the woman had at least visited the clinic once in the past two years and 75% stated that they were satisfied with the healthcare services they were receiving. Those who were not satisfied with the healthcare services that they had received, gave the following reasons: inadequate drug supply (33%), poor service delivery (29.1%) and delayed assistance at centre (16%), while others felt that the service provided was not comprehensive (21.4%). Figure 9 shows for each clinic the proportions of women who were satisfied and those dissatisfied by the health service provided.
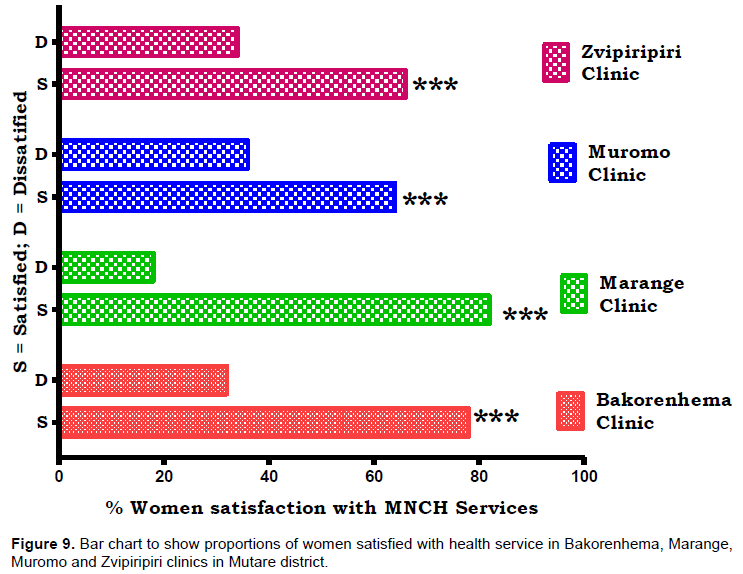
In the four clinics relatively, higher women were satisfied with the service they received as compared to those who had feelings to the contrary. For those who attended the clinics, the least dissatisfied women were found at the Marange Clinic. Two-way ANOVA for the proportion of women and their degree of satisfaction as per health institution showed a statistically significant variation in the interaction (***P < 0.0001, % of total variation = 9.49, Df = 3, Sum-of-squares = 784.0, Mean square = 261.3, F = 522.7), in the health institutions (***P < 0.0001, % of total variation = 0.91, Df = 3, Sum-of-squares = 75.00, Mean square = 25.00, F = 50.00), and in the degree of satisfaction (***P < 0.0001, % of total variation = 89.55, Sum of squares = 7396, Mean square = 7396, F = 14790). Bonferroni post tests for comparisons of the degree of satisfaction with services showed extremely significant differences between those satisfied with the services for Bakorenhema Clinic vs Marange Clinic (***P < 0.001, Diff = 5.000, 95% CI of diff = 2.199 to 7.801, t = 7.071), for Bakorenhema Clinic vs Zvipiripiri Clinic (***P < 0.001, Diff = -13.00, 95% CI of diff = -15.80 to -10.20, t = 15.56), for Marange Clinic vs Muromo Clinic (***P < 0.0001, Diff = -18.00, 95% CI of diff = -20.80 to -15.20, t = 25.46), for Marange Clinic vs Zvipiripiri Clinic (***P < 0.001, Diff = -16.00, 95% CI of diff = -18.80 to -13.20, t = 22.63) and for Muromo Clinic vs Zvipiripiri Clinic (*P < 0.05, Diff = 2.000, 95% CI of diff = -0.8014 to 4.801, t = 2.828)(Figure 9).
Health facility assessment
Health workers were interviewed and direct observation of the clinics’ capacity in terms of physical structures, buildings, staff skills, equipment and drug availability were carried out to assess the accessibility and utilization of health facilities by clients.
Staff availability and capacity
Almost all the clinics had two nurses of the same sex and one nurse if the opposite sex. Marange clinic was found to have one Registered General Nurse (RGN) and two nurse aids. The other three clinics had one Primary Care Nurses (PCN) and one State Certified Nurses (SCN). A gender sensitivity was displayed in the deployment of nurses in clinics (Table 2).
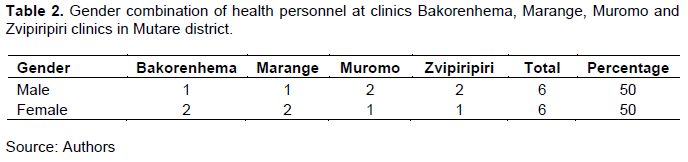
Overall, there was a balanced representation of gender in health personnel in the district. Through further interviewing the capacity of the staff in terms of MNCH service provision was assessed using the type of training received in relation to MNCH that the staff have received in the past 2 years. Figure 10 shows training received by staff in the past 2 years. The study investigated whether the quality and quantity of recent training may influence the accessibility and utilization of health services for all particular health institutions in Mutare District. Also, the effect of training type according to gender of the staff was examined Figure 10. Females and males were equally trained in some areas but differently in others. Critical training such as Post Abortion Care, Family Planning, Gender Mainstreaming, Emergency Preparedness, and Governance and Management were conspicuously missing amongst the staff members in the study area.
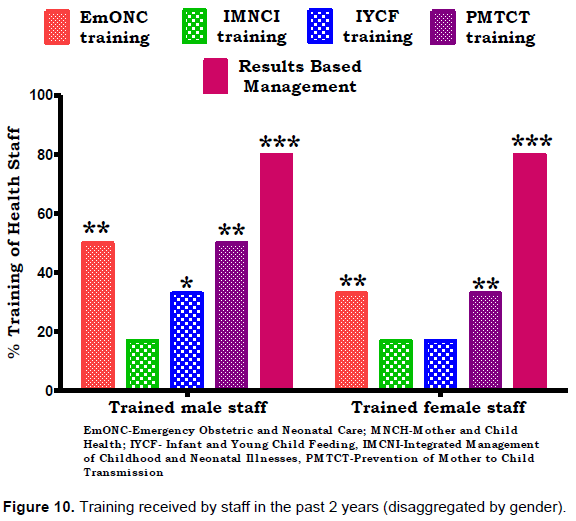
Two-way ANOVA comparing the type of training by gender of those trained showed a significantly higher variation towards the type of training than the gender (**P = 0.0034, % of total variation = 91.86, Df = 4, Sum-of-squares = 4707, Mean square = 1177, F = 28.19). The Bonferroni posthoc-tests comparing health institutions in terms of male and females trainings received showed statistically significant variation towards males receiving EmONC training vs IMNCI training (*P < 0.05, Difference = -33.00, 95% CI of diff = -94.76 to 28.76, t = 3.611), for IMNCI training vs PMTCT training (*P < 0.05, Difference = 33.00, 95% CI of diff = -28.76 to 94.76, t = 4.613), for IMNCI training vs Results Based Management (**P <0.05, Difference = 63.00, 95% CI of diff = 1.244 to 124.8, t = 6.894) and for IYCF training vs Results Based Management (*P < 0.05, Difference = 47, 95% CI of diff = -14.76 to 108.8, t = 5.143). Statistically significant variations towards more females training was observed for IMNCI training vs Results Based Management (**P <0.05, Difference = 63.00, 95% CI of diff = 1.244 to 124.8, t = 6.894), for IYCF training vs Results Based Management (**P < 0.01, Difference = 63.00, 95% CI of diff = 1.244 to 124.8, t = 6.894) and for PMTCT training vs Results Based Management (*P < 0.05, Difference = 30, 95% CI of diff = -31.76 to 91.76, t = 5.143) (Figure 10).
State of the clinic (infrastructure, drugs and health equipment availability)
On assessing the state of the clinics in terms of structures or buildings, drugs and or equipment, it was found that three of the four clinics had security fences. Zvipiripiri clinic had a fence that was in a fair condition, while Muromo and Marange clinics had fences that were in a very bad condition and Bakorenhema had no fence at all. For communication, the nurses stated that they use their own cellular phones as the radio equipment was now old while other clinics did not even have a communication radio.
The structures or buildings at Muromo Clinic were in poor condition while the other three had buildings in fair condition. All the clinics (100%) had incinerators, Otto Way pits and a Bottle-disposal pit and were practicing proper liquid and solid waste disposal. All the clinics used electricity power sources and when power cuts occurred candles and firewood were used. At Bakorenhema there were very frequent power cuts. Night deliveries were often affected when there was no light to see and to monitor the mother and child. Warm water was not available at and after delivery during power cuts. In Marange catchment area a woman stated that “when a woman is about to deliver and it is during the night, we find it better to deliver at home as there may be no electricity at the clinic and it will be too cold for the baby at the clinic at night”.
In relation to MNCH Bakorenhema, Zvipiripiri and Muromo clinics had 50% drug stock outs of misoprostol, magnesium sulphate, antihypertensives (methyldopa, nifedipine), while Marange clinic was only short of 35% of the drugs. The MoHCC official stated that their rural clinics were being assisted by UNICEF in terms of drug stocks, but that the NGO had specialised in supplying certain drugs only and not all the drugs required by the clinics, resulting in an oversupply and a vast shortage of some drugs at the clinics.
All the clinics lacked about 30% of essential equipment such as resuscitative sets, adults and baby laryngoscopes, airway tubes, endotracheal tubes, heavy duty and surgical gloves. All other equipment required for MNCH services was available in all clinics with equipment donations having been recently received from the Canadian National Office (CNO) of Plan international. A health coordinator from Plan International explained that it was an NGO implementing a project on maternal health called “Women and their Children’s Health” (WATCH) which supplied the equipment which aimed to ‘improve maternal, neonatal and child health for underserved populations in the Mutasa, Mutare and Chipinge districts in Manicaland Province.
Water and sanitation
Two out of four of the clinics were found to have separate staff toilets while the other two clinics toilets were shared between patients and staff. The patient toilets for all four clinics where Blair toilets and functional. Each clinic had at least a hand washing facility in close proximity to the Blair toilets.
State and capacity of the delivery room
Each of the clinics had a delivery room with at least 2 beds and one drip stand but none of the clinics had incubators for new-born babies, especially for those born with complications. “Women that gave birth to premature babies had to carry their babies and transport them themselves to the nearest mission or district hospital for specialised care as clinics had no capacity to provide this care, nor to transport the baby as there were no ambulances that were kept at the clinics”, it was stated at one FDG. All clinics had delivery packs, a sluice sink, functional suction device, a portable light, a baby breathing kit and adult and baby weighing scales. However, 50% of the scales were old and malfunctioning. 100% of the nurses had no protective clothing for use during delivery, no oxygen supply equipment and no functioning heaters.
Recordkeeping tools and skills
Although all the clinics had ANC booking registers, delivery registers, and postnatal registers that where being fully utilized, none of the clinics had peri-natal reporting forms and referral registers and only fifty percent of the health centres had a copy of the National Health Strategy and Road Map that focus on MNCH services. All the clinics had a Health Centre Committee that would meet at least once a month to discuss health related issues and on the management of the clinics.
Major constraints faced in accessing and utilizing MNCH services as proposed by rural women
The women were asked for their own opinions of what they perceived to be the major constraints they faced in accessing and utilising MNCH services. The results have been presented in Figure 11.
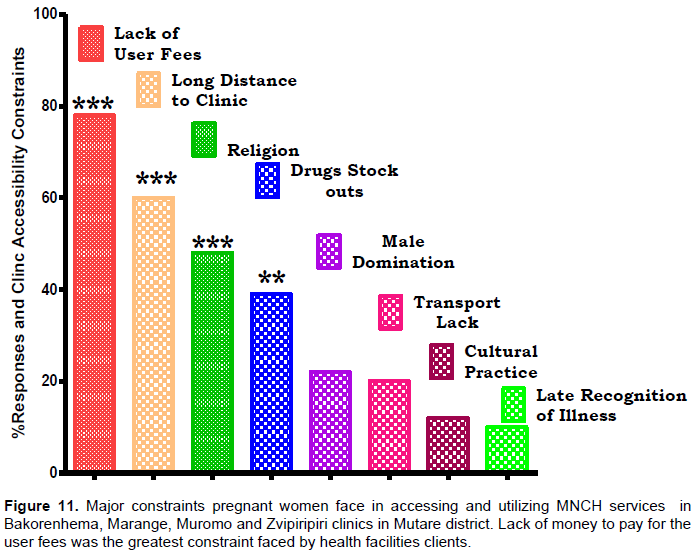
The bar chart below graphically presents the major constraints that rural women in Mutare stated to be facing in accessing and utilizing MNCH services in their own opinion, in the study. Distance from clinic posed meaningful obstruction to access of health facilities, followed religion and fear of drugs stocks out influenced attendance of the clinics as well. One-way ANOVA for the major constraints faced when accessing and utilizing health facilities and services indicated that the factors were extremely significantly varied in contributing to the issue (***P < 0.0001, F = 1799, R squared = 0.9987).
The Tukey's Multiple Comparison Test showed that the factors cited as constraints for accessibility and utilization of health facilities were statistically significantly varied and independent from each with lack of user fees showing a higher prevalence as seen for Lack of User Fees vs Drugs Stock outs (***P < 0.05, Mean Diff = 39.00, q = 67.55, 95% CI of Diff = 36.17 to 41.83), for Lack of User Fees vs Male Domination (***P < 0.05, Mean Diff = 56.00, q = 96.99, 95% CI of Diff = 53.17 to 58.83), for Lack of User Fees vs Transport Lack (***P < 0.05, Mean Diff = 58.00, q = 100.5, 95% CI of Diff = 55.17 to 60.83), for Lack of User Fees vs Cultural Practice (***P < 0.05, Mean Diff = 66.00, q = 114.3, 95% CI of Diff = 63.17 to 68.83). Lack of User Fees vs Recognition of Danger Late significantly influenced inaccessibility and utilization of health facilities (***P < 0.05, Mean Diff = 68.00, q = 117.8, 95% CI of Diff = 65.17 to 70.83). Long Distance to Clinic vs Transport Lack negatively influenced accessibility and utilization of health facilities (***P < 0.05, Mean Diff = 40.00, q = 69.28, 95% CI of Diff = 37.17 to 42.83), for Long Distance to Clinic vs Cultural Practice (***P < 0.05, Mean Diff = 48.00, q = 83.14, 95% CI of Diff = 45.17 to 50.83), and for Long Distance to Clinic vs Recognition of Danger Late (***P < 0.05, Mean Diff = 50.00, q = 86.60, 95% CI of Diff = 47.17 to 52.83). Religion vs Recognition of Health Danger Late contributed negatively towards accessibility and utilization of health facilities (***P < 0.05, Mean Diff = 38.00, q = 65.82, 95% CI of Diff = 35.17 to 40.83) as well as did Religion vs Cultural Practice (***P < 0.05, Mean Diff = 36.00, q = 62.35, 95% CI of Diff = 33.17 to 38.83). Drugs Stock outs vs Cultural Practice encouraged reduced accessibility and utilization of health facilities (***P < 0.05, Mean Diff = 27.00, q = 46.77, 95% CI of Diff = 24.17 to 29.83), as well as Drugs Stock outs vs Recognition of Health Danger Late (***P < 0.05, Mean Diff = 29.00, q = 50.23, 95% CI of Diff = 26.17 to 31.83) and Drugs Stock outs vs Transport Lack (***P < 0.05, Mean Diff = 19.00, q = 32.91, 95% CI of Diff = 16.17 to 21.83).
DISCUSSION
In the Mutare District, accessibility and utilization of healthcare facilities for health-related issues was shown to be governed by three categories of factors described as those that cause delays in making decisions to seek health care (Delays 1), those that cause a delay in reaching health care (Delay 2), and those that cause delays in receiving treatment at the health care facility (Delays 3). Indicators of delays in decision-making to seek heath care was noted by the sampled household demographics and its characteristics, women's literacy level, availability of a baby health card and baby birth weight. Delay 2, delay in reaching a healthcare facility, as a contributor to accessibility and utilization of health services was the distance to nearest health facility and the mode of transport used reach health facility. Delay in receiving treatment at health care facility, Delay 3, was indicated by the place where women delivered, the first Point of contact when infant or pregnant woman is sick, client satisfaction/dissatisfaction of health services received, staff availability at health facility and facility capacity, health facility state (infrastructure, drugs and health equipment availability), water and sanitation, state and capacity of delivery room, record keeping tools and skills and major constraints faced by clients.
In exploring and identifying factors that cause rural women to commit Delay 1 in seeking MNCH services male domination, religious and cultural beliefs, low literacy levels and late recognition of danger warning signs of a sick infant, prominently featured in the findings. Male domination was shown by that about 74% of the households where male-headed and FGD with women brought out that some women were denied access to health care by their husbands who had the decision-making role in the household. Gender-related issues have an effect on women’s access and utilization of MNCH services especially in patriarchal societies, especially those found in the rural parts of Zimbabwe. Similar findings have been known where male dominated households tended to have a higher impact on < 5-year-old malnutrition (Ncube et al., 2020) as well as a being a determinant of their malnutrition and stunting (Ncube et al., 2020).
Sensitized, informing and or educating men on the importance of MNCH services for women and their children’s, through the use of campaigns and Information, Education and Communication (IEC) material such as posters and fliers may assist in changing male dominance in households. Maternal, neonatal, infant, and child mortalities and morbidities in their community and the nation as a whole is reduced when men are made aware that access and utilization of MNCH services by women and infants is essential. Having a clear understanding of the benefits of utilizing quality health services by men may bring their buy-in to the vision of the MDGs to reduce maternal and child mortalities. Religious and cultural beliefs of male over female dominance pervade the lengths and breaths of the Zimbabwean, if not sub-Saharan Africa, moral fabric (Ditekemena et al., 2012) with gender based violence an acceptable anomaly (Ntaganira et al., 2008).
The over-representation of Apostolic Faith believers in Bakorenhema (67%) and Marange (48%) catchment areas showed a religious dominance in the areas which was intimately associated with low levels of infant immunisations 28.4 and 28.9%, respectively. The strong teaching by spiritual leaders and resultant belief that healing was obtained through prayer was intimated by rural women who revealed that their members were not allowed to visit the clinic for care. This religious system may be converted to adopt both religions and conventional medical practice for the advantage of MNCH as a select, unique, obedient and compliant population already exists (Bopp, 2013; Brooks and Koenig, 2002). Whether prayers are legitimate in healing disease and sickness is neither here nor there but there is a robust following of this phenomenon in Mutare District which needs to be utilized to drive positive MNCH outcomes (Dossey and Hufford, 2005).
Very high home baby deliveries in Bakorenhema (70%) and Marange (57%) contrasted sharply with Muromo (23%) and Zvipiripiri (44%) where the religious beliefs were not as rife. There is great need for practical sensitization of cultural and religious leaders on the importance of quality and timely health care for pregnant women and infants along the continuum of care (from pregnancy to delivery to child growth) (Bennett and Hale, 2009; Barnes and Curtis, 2009). Once the leaders have a full acceptance of how crucial it is for pregnant women and infants to receive quality health care, the appreciation and acceptance of access and utilization of MNCH services will eventually cascade down to all the believers (Olivier et al., 2015; Levin, 2016). While the Marange Apostolic Faith Church may be controversial in it approach to conventional medical practice, it remains an influential organization whose impact on health outputs and outcomes cannot be ignored and ways need to be found to harness it strengths in leadership and fellowship to the advantages of health systems (Curlin et al., 2007).
Low literacy levels and late recognition of danger warning signs of a sick infant was found to be guided by level of education of the mothers as 59.5 and 37.5% of the women had completed secondary and primary education, respectively Informal and not being educated at all were at 1.2 and 1.9% which are too high for a country known to have high literacy levels. Due to limited formal education, a woman might not be able to fully identify symptoms of pregnancy complications and or danger warning signs of the sick infant in time to react and seek health care for herself or the baby.
Awareness campaigns need to be made informing and educating WCBA (15-49years), on what danger warning signs to be aware of to enable timely decisions making to seek quality health care. Loosely, CCGs are groups of up-to 10 women that have a leader called the ‘Lead Mother’, whom goes (with other Lead mothers) twice a month to be capacitated by a Village Health Worker on MNCH related issues, such as on exclusive breast feeding, importance of immunisation, Ante-Natal Care visits, etc. These lead mothers then, in-turn, disseminate the information to the other 9 women in their CCG.
Women in rural areas have challenges in reaching health care centres for MNCH services. Most clinics were a long distance away, which is a strain for pregnant women or infants to reach without reliable transport thus, creating a barrier to reach the health clinics. Distance traveled by 31% of women were <5 km to the nearest health centre and 43% lived between 6-10 km from the health centre. Noting that the recommended optimum distance to travel to nearest health centre or clinic is 8 km, 26% of the respondents stayed >10km away and 15% stayed between 11-20 km with 11% being >20 km away from the nearest health centre. Health referral systems need to be strengthened and expanded through the provision of vehicles that can be used as ambulances to ferry people to and from the health centers and increase MNCH service outputs and outcomes.
Mother waiting shelters need be constructed at all clinics as this will assist pregnant women that stay more than 10 km away from the clinics and motivate women to go to the clinic as they will be able find shelter before and after delivery and not need to travel to and from the nearest clinic for the recommended four antennal visits.
With walking being the most common mode of transport (81%) to the nearest health centre, it is plausible to observe the dire need for transport infrastructure as an impediment to access to health clinics for MNCH. Animal drawn cart (6%), bicycle (8%) and wheel barrow were cited as the alternative modes of transport to the clinics, with none of the women having ever been in an ambulance. Women were forced to walk to clinics due to poverty and poor road infrastructure and networks. As women are not able to reach clinics easily, capacitating village health workers with mobility and ability to monitor pregnant women and infants at home for any danger warning signs of pregnancy complications or infant sicknesses could ensure quicker patient management and avert, where possible, transfer of patients to health clinic or where necessary to do so quickly.
Additionally, a mother waiting for homes availability at health centres will ease travelling needs that expose both pregnant women and infants to harsh conditions and discourage them from accessing MNCH services. While at the clinics, certain factors tend to affect women and infants during the course of receiving treatment and these intrude on their desire to continue receiving health services. These factors were explored and identified as unavailability of drugs and up-to date equipment at the clinic and low capacity and skill of health workers to give quality health care. The drug stocks relative to MNCH use were observed to be at 50% in Bakorenhema, Zvipiripiri and Muromo clinics. Stocks had run out of drugs such as misoprostol, magnesium sulphate, antihypertensive methyldopa, and antihypertensive nifedipine, while Marange clinic was only short of 35% of the drugs. While NGO’s supplied drugs to clinics for free, it is recommended that the do so after consultation with the clinics as to what drugs were needed and were in short supply to curb over supply of certain drugs when there was dire need of other essential drugs. Capacitating staff on equipment maintenance may go a long way in reducing the down time or complete run down of critical equipment.
Low capacity and skill of health workers to give quality health care was observed as an area deserving critical attention as public confidence in the health system tended to be eroded if adequate care is not provided. While about 50% of the male and 33% of female staff had received training in Prevention of Mother to Child Transmission (PMTCT) and Emergency Obstetric and Neonatal Care (EmONC), 17% of both male and female staff had been trained in IMNCI, and 80% in Results Based Management. None of the staff members from the 4 clinics had been trained in Post Abortal Care, Family planning; Gender mainstreaming, Emergency preparedness and or Governance and management in the past 2 years. Therefore, there is need for ongoing training workshops and courses for rural health workers every three years for PCTCT, IMNI, EmONC and annual training on new MNCH aspects such as gender mainstreaming Emergency preparedness and or Governance and management.
CONCLUSION
Imperatively, all women should have access and utilization of MNCH services so as to be able to increase maternal outputs and outcomes. Contributing factors to women’s lack of access and utilization of MNCH services can be categorised into those factors that delay the women making a decision to seek health care, those that delay the women reaching the health facility in time, and those that delay the woman and infant receiving timely quality care or treatment at the health centre.
Geographic location from health centre, lack of money and or user fees, religion, capacity of the health workers, treatment received at the health centre, up-to date equipment and drugs unavailability, male domination, lack of transport, cultural beliefs, low literacy levels and late recognition of danger warning signs of a sick infant were observed as major obstacles to receiving access to quality MNCH care in Mutare District. Support from NGO’s and community-based organizations to Governments, Local Authorities to the clinics to address challenges so that women receive the quality health care they need which they and their new-borns have a right to receive. Churches, religious and spiritual faith-based organizations (Marange Apostolic Faith) may be instrumental in building strong rural health systems if the leaders may be convinced that it is the best way to go for quality healthy outputs and outcomes (Campbell et al., 2007).
RECOMMENDATIONS
Continuous educational programs need to be given to men and religious groups on the creation of enabling environment for women and children to have accessibility and utilization of health facilities. Construction of waiting homes for pregnant women homes be constructed at every clinic for women to stay in, a few days before and after delivery. Religious leaders be sensitized on the importance of the use of Maternal, Neonatal and Child Health services by women of child bearing age. Health workers require continuous training to build trust and confidence in the communities they serve and reduce referrals that increased costs on clients with subsequent abhorrence of the services provided.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate the NUST Faculty of Medicine, UKZN for providing enabling environment, accounting services and extra budgetary contingencies that facilitated the smooth running and writing of the MS. The NUST paid for the research through resources like time, office space and salaries which were not recouped from the research budget. UKZN supported the Manuscript writing funding through time and office stationery.
REFERENCES
|
Arntsen H, Waldrop A (2018). Introduction to Special Issue: Qualitative Method/ologies in Development Studies. Forum for Development Studies. 45(2):185-189. |
|
|
Barnes PA, Curtis AB (2009). A national examination of partnerships among local health departments and faith communities in the United States. Journal of Public Health Management and Practice 15(3):253-263. |
|
|
Bennett RG, Hale WD (2009). Building Healthy Communities through Medical-Religious Partnership. Baltimore: Johns Hopkins University Press. |
|
|
Bopp M, Fallon EA. (2013). Health and wellness programming in faith-based organizations: a description of a nationwide sample Health Health Promotion Practice 14(1):122-131. |
|
|
Brooks RG, Koenig HG (2002). Crossing the secular divide: government and faith-based organizations as partners in health. The International Journal of Psychiatry in Medicine 32(3):223-234. |
|
|
Campbell MK, Hudson MA, Resnicow K, Blakeney N, Paxton A, Baskin M (2007). Church-based health promotion interventions: evidence and lessons learned. Annual Review of Public Health 28:213-234 |
|
|
Curlin FA, Lawrence RE, Chin MH, Lantos JD (2007). Religion, conscience, and controversial clinical practices. New England Journal of Medicine, 356(6):593-600. |
|
|
Devereux S, Hoddinott J (1992). Fieldwork in Developing Countries Harvester: New York. |
|
|
Ditekemena J, Koole O, Engmann C, Matendo R, Tshefu A, Ryder R (2012). Determinants of male involvement in maternal and child health services in sub-Saharan Africa: a review. Reproductive Health. 9(1):32. |
|
|
Dossey L, Hufford DJ (2005). Are prayer experiments legitimate?: twenty questions. Explore (NY) 1(2):109-117. |
|
|
Furusa SS, Coleman A (2018). Factors influencing e-health implementation by medical doctors in public hospitals in Zimbabwe. SAJIM (Online) 20(1):1-9. |
|
|
KNOEMA (2020). Zimbabwe - Infant mortality rate. [cited 2021 17.03.2021]; |
|
|
Kothari CR (1985). Research Methodology-Methods and Techniques. New Delhited: Wiley Eastern Limited. |
|
|
Levin J (2016). Partnerships between the faith-based and medical sectors: implications for preventive medicine and public health. Preventive medicine reports 4:344-350. |
|
|
Mattoo K, Shubayr M, Al Moaleem M, Halboub E (2020). Influence of Parental Physical Activity and Screen Time on the BMI of Adult Offspring in a Saudi Population. Healthcare (Basel). 8(2):110. |
|
|
Mgawadere F, Unkels R, Kazembe A, van den Broek N (2017). Factors associated with maternal mortality in Malawi: application of the three delays model. BMC Pregnancy and Childbirth. 17(1):219. |
|
|
Mikklesen B (2005). Methods for Development Work and Research, A New Guide for Practitioners. 2nd ed, ed. New Delhi: SAGE Publishers 179 p. |
|
|
MoHCC (2008). The National Health Strategy for Zimbabwe (2009-2013). MoHCC, Editor MoHCC: Harare, Zimbabwe. |
|
|
MoHCC (2009). National Child survival Strategy for Zimbabwe 2010-2015, MOHCW., MoHCC, Editor.(2009): Harare, Zimbabwe. |
|
|
National Academies of Sciences, Engineering and Medicine (2016). Parenting Matters: Supporting Parents of Children Ages 0-8. 2016, Washington, DC: The National Academies Press. |
|
|
Ncube B, Mavondo GA, Chamisa JA. (2020a). Maternal Influences Contributing to under 5 Years Child Malnutrition in Insiza District, Matebeleland South, Zimbabwe. Asian J Pregnancy and Childbirth. 3(2):1-25 |
|
|
Ncube B, Mavondo GA, Kandawasvika G, Chamisa JA (2020b). Elucidation of Food Security as a Determinant of Malnutrition and Stunting on Children under Five Years: A Case of Insiza District, Matabeleland South, Zimbabwe Asian J Pediatric Research 3(3):11-31. |
|
|
Ngoma-Hazemba A, Hamomba L, Silumbwe A, Munakampe MN, Soud F (2019). Community Perspectives of a 3-Delays Model Intervention: A Qualitative Evaluation of Saving Mothers, Giving Life in Zambia. Global Health: Science and Practice 7(Supplement 1):S139-S150. |
|
|
Ngwenya S, Nleya F, Mwembe D (2020). Maternal survival in a low-resource setting, Mpilo Central Hospital, Bulawayo, Zimbabwe. BMC Res Notes 13(46 ). |
|
|
Ntaganira J, Muula AS, Masaisa F, Dusabeyezu F, Siziya S, Rudatsikira E (2008). Intimate partner violence among pregnant women in Rwanda. BMC Womens Health 8:17.10.1186/1472-6874-8-17 |
|
|
Nyereyemhuka NC, Mavondo GA, Moyo O, Chikuse FF, Mkhwanazi BN, Chavani O (2020). An Analysis of Factors Contributing to Late Focused Antenatal Clinic (FANC) Booking for Pregnant Women Attending Hartcliffe Polyclinic in Harare, Zimbabwe. Asian J Pregnancy and Childbirth. 3(2):26-45 |
|
|
Olivier J, Tsimpo C, Gemignani R, Wodon Q (2015). Understanding the roles of faith-based health-care providers in Africa: Review of the evidence with a focus on magnitude, reach, cost, and satisfaction. The Lancet 386(10005). |
|
|
Pacagnella RC, Cecatti JG, Osis MJ, Souza JP (2012). The role of delays in severe maternal morbidity and mortality: expanding the conceptual framework. Reproductive Health Matters 20(39):155-163. |
|
|
Plan international (2012). Women and their Children's Health (WATCH) Baseline report, Mutare, Zimbabwe: Plan International: Harare, Zimbabwe. |
|
|
Sen G (2019). Gender Equality and Women's Empowerment: Feminist Mobilization for the SDG s. Glob Policy (10):28-38. |
|
|
USAID (2007). Improving the Coverage of Maternal Newborn and Child health in Pakistan, Islamabad: USAID: Islamabad, Pakistan. |
|
|
Westfall L (2008). Sampling Methods, The Certified Software Quality Engineer handbook. London: ASQ Quality Press. |
|
|
Worthman CM, Tomlinson M, Rotheram-Borus MJ (2016). When can parents most influence their child's development? Expert knowledge and perceived local realities. Social Science and Medicine154:62-69. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


