Full Length Research Paper

ABSTRACT
Ultrasound scanning (USS) and high vaginal swab culture and urine microscopy culture and sensitivity (m/c/s) tests are the most common investigations used for the diagnosis of pelvic inflammatory disease (PID) in our locality. The aim of this study was to determine the diagnostic accuracy of ultrasound in the diagnosis of PID keeping laboratory high vaginal swab/urine microscopy, culture as gold standard. The USS, high vaginal swab and urine m/c/s reports of patients referred with PID conditions between January 2010 to April 2013 were obtained from the medical records departments of Nnamdi Azikiwe University teaching hospital, Nnewi, Anambra state. The diagnostic accuracy was determined by calculating sensitivity, specificity, positive predictive value and negative predictive value using performance characteristics test. Descriptive and inferential statistics were also used. Spearman rho’s non parametric analysis and statistical package for social sciences (SPSS) version 17.0 was equally used. The total number of subjects that were scanned for PID was 120. The highest number of subjects 80 (66.6%) was seen in 21 to 30 years age group. The sensitivity, specificity, accuracy, negative predictive value and positive predictive value of ultrasound in PID diagnosis was found to be 100, 65.3, 89.2, 100 and 86.3%, respectively. There was no significant correlation between USS diagnosis of PID and HVS/urine culture findings (p > 0.01). Ultrasound is valuable as the first line of investigation (screening tool) in the diagnosis of PID and should be used in conjunction with other medical investigations to facilitate accurate diagnosis of PID.
Key words: Ultrasound, pelvic inflammatory disease, urine culture, high vaginal swab culture, diagnostic accuracy.
INTRODUCTION
Pelvic inflammatory disease (PID) is a polymicrobial infection in women characterised by infection of the upper genital tract including endometritis, salpingitis, pelvic peritonitis, occasionally leading to the formation of tubo-ovarian abscess (Turzic and Kocijancic, 2010). It is an infection caused by inflammatory continuum from the cervix to the peritoneal cavity (Soper, 2010). It is a serious complication of some sexually transmitted diseases (STDs), especially Neisseria gonorrhoeae and Chlamydia trachomatis in women of child bearing age. Adolescents are at the increased risk for PID and should therefore be advised to delay the onset of sexual activity until age 16 years or older (Simms et al., 2006). It can be acquired non-sexually through operative or non-operative introduction of vaginal bacteria (Grodstein and Rothman, 1999; Roses, 2001). PID can also develop from an unsterile abortion or child delivery or may be a complication of intrauterine contraceptive devices (IUCDs) insertion. If pelvic inflammatory disease is not promptly treated, they can cause damage to the fallopian tubes and to tissues in and near the uterus and ovaries. They can also lead to infertility, ectopic pregnancy, abscess formation and chronic pelvic pain (CDC, 2011).
Pelvic inflammatory disease is the single most important cause of tubal pathology leading to infertility (CDC, 2011). The signs and symptoms of PID are usually indistinguishable among women with acute salpingitis, those with endometritis without acute salpingitis and those with cervicitis but neither endometritis nor salpingitis (Eckert et al., 2002; Wiendfield et al., 2003; Welner-Hanssen et al., 1983). Patients with PID can present with unbearable abdominal pelvic pain or may be completely asymptomatic (Dayan, 2006). They may also be present with lower abdominal pain or pelvic pain, vaginal discharge, abnormal vaginal bleeding, dyspareunia and adnexal mass or tenderness, cervical motion tenderness or fever (Dayan, 2006). No specific international data are available for PID incidence worldwide. In 2005, the world health organisation (WHO) estimated that approximately 448 million new cases of curable sexually transmitted infections occur annually in individuals aged 14 to 49 years (WHO, 2010). Factors contributing to difficulty of determining the actual worldwide incidence and prevalence of PID include the following (Lon et al., 2006):
1. Non recognition of the disease on the part of the patient.
2. Difficulties in obtaining access to care.
3. The often subjective method of disease diagnosis.
4. The lack of diagnostic and laboratory facilities in many developing countries.
5. Underfunded overstretched public health system.
Laboratory urine microscopy, culture and sensitivity(m/c/s) and high vaginal swab (HVS) tests, are sensitivity and specificity tests which aid in the identification and confirmation of the presence of organisms that may be the causative factor of the infection and to determine the best antibiotic therapy for treatment (Monica, 2000).
These tests are mostly used in our locality because they are cheap. With the advent of real time sonography, the female reproductive organs can be easily assessed and the uterus, cervix, vagina, fallopian tubes and the ovaries seen. Real time imaging is preferred to other conventional diagnostic methods because of its simplicity and accuracy in evaluation of the female reproductive organs. Ultrasonography is the imaging method of choice followed closely by Magnetic Resonance Imaging (Jaiyeoba and Soper, 2011). It is also used as an additional diagnostic tool to high vaginal swab and urine m/c/s tests for the diagnosis and confirmation of pelvic inflammatory disease. Scanning of the body using ultrasound is capable of showing areas of abnormal anatomy and pathology that may facilitate the achievement of specific diagnosis or add further support to the results drawn from other methods of diagnosing pelvic inflammatory disease.
Ultrasound plays a tremendous role in the investigation of the pelvic visceral. Pelvic sonography is performed commonly in patients who have a clinical diagnosis of PID. Although, the study may be normal or sometimes non specific, there are various findings that are characteristic of this process (Horrow et al., 2007). Pelvic ultrasonography has limited sensitivity for the diagnosis of PID but the specific finding of thickened fluid-filled tubes by ultrasonography supports the diagnosis of upper genital tract infection (Timor-Tritsch and Rottem, 1987). Ultrasonography is the most frequently ordered imaging examination when pelvic inflammatory disease (PID) is suspected (Agarwal, 2013).
Other diagnostic methods for investigating PID include laparascopy, endo-cervical/ urethral swab tests and endometrial biopsy. No single test has adequate sensitivity and specificity to diagnose PID. A large multisite United States study found that cervical motion tenderness as a minimum common criterion increases the sensitivity of the CDC diagnostic criterion from 83 to 95%. However, the modified 2002 CDC criteria do not identify women with subclinical disease (Blenning et al., 2007).
In developing countries such as Nigeria, ultrasonography remains a diagnostic tool for assessment of pelvic inflammatory disease because it is cheap, readily available and does not make use of ionizing radiation.
METHODOLOGY
This was a cross sectional validation study of documented records. This study covered a period of 3 years from January, 2010 to April, 2013. The folders of patients who were suspected/diagnosed of having PID and had undergone USS, urine m/c/s and HVS tests in Nnandi Azikiwe University Teaching Hospital, Anambra State were evaluated. A total of 120 patients’ folders were obtained from the medical records department of the hospital within the 3 year period studied (that is, between January, 2010 to April, 2013). In this study, folders with both ultrasound, HVS and urine m/c/s reports were included while the folders with either one or none of them were excluded. Sources of data were basically secondary relying on the information the hospital and staff recorded in patients’ folders, request cards and ultrasound registers. It was carried out by going through the ultrasound registers to note all cases of pelvic scan with clinical indication of PID. Then using their hospital numbers, the folders were traced to the medical records departments with permission from the hospital heads. The names and age of the patients were also obtained from the folders.
Data analysis
The correlation of ultrasound diagnosed cases of PID with laboratory high vaginal swab and urine m/c/s findings was calculated using Spearman rho’s non-parametric analysis and statistical package for social sciences (SPSS) Version 17.0, while the sensitivity, specificity and accuracy, positive predictive value and negative predictive value of ultrasound scan in diagnosis of PID using high vaginal swab as the gold standard, was calculated using performance characteristics test.
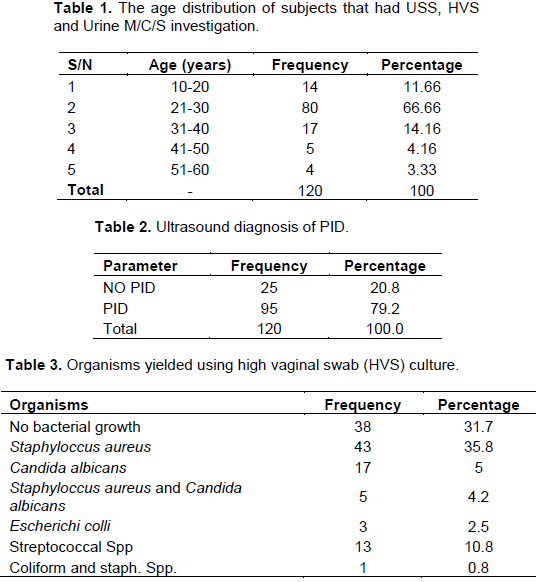
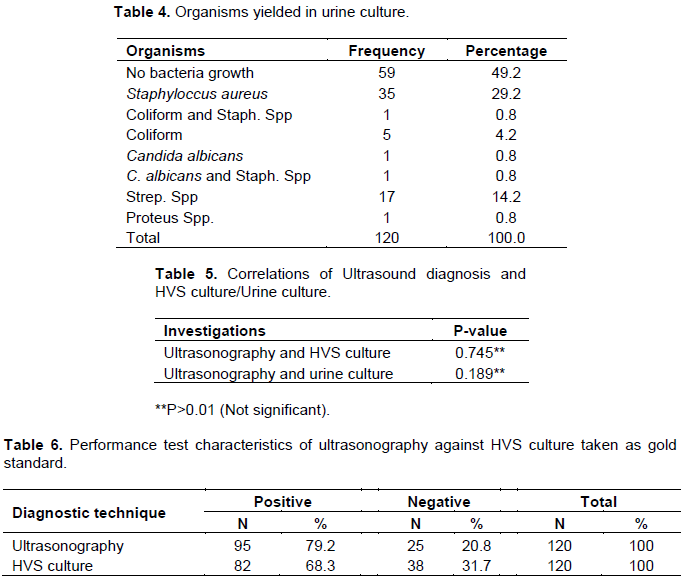
Most of the subjects were within the age range of 201-30 years (Table 1). PID was noted in 79.2% of the cases (Table 2). Staphylococcus aurens was the most occurring organism detected using HVS while colliform and staphylococcus species were least occurring (Table 3). Majorly there was no bacterial growth detected in the urine culture (Table 4). There was no significant difference between sonographic finding and HVS culture and also no significant difference in urine culture (Table 5). The performance test characteristics of ultrasonography against HVS culture taken as gold standard shows that more positive results were obtained using sonography (Table 6).
RESULTS
Medical records of 120 female subjects were assessed to correlate ultrasound scan (USS) diagnosis of PID with laboratory urine m/c/s and HVS diagnosis and also to determine the sensitivity, specificity and accuracy of ultrasound in the diagnosis of PID. There were 120 subjects studied. Their age ranged from 11 to 60 years and their mean age was 28 years. Most of them were within the age range of 21 to 30 years, and constituted 66.6%. The least age group was within 51 to 60 years and they constituted 3.3% of the study. Using ultrasound for the diagnosis, 95 (79.2%) were reported to have PID while 25 (20.8%) do not have it. The most prevalent causative organism for this condition using HVS and Urine cultures were staphylococcus species. There was no significant correlation (r = 0.030) between ultrasound diagnosis and HVS culture diagnosis of PID. No significant correlation existed between ultrasound and urine culture in the diagnosis of PID (r = 0.121).
DISCUSSION
Pelvic inflammatory disease refers to the infection of the upper genital tract of the female reproductive organ which if left untreated can lead to serious consequences including infertility, ectopic pregnancy, abscess formation and chronic pelvic pain (CDC, 2011). The spread of these infections are normally in an ascending manner through the vagina or cervix into the uterine cavity. Lymphatic spread may also occur either parametrially or along the surface of the uterus.
Infection can also spread from the bowel or can be blood borne (Ash, 2006). Ultrasonography is the most frequently ordered imaging examination when pelvic inflammatory disease is suspected (Agarwal, 2013). Its advantage lies in the fact that it is safe, non invasive and readily available. The diagnosis of PID is also facilitated with the combined use of ultrasonography and laboratory high vaginal swab culture and urine culture, as these laboratory tests aid in the identification of the causative organisms of PID and also in determining their level of sensitivity to antibiotic therapy which is used in the treatment of PID (Monica, 2000) while sonography on the other hand reveals the extent of the damage and effects on surrounding tissues (Njoku et al., 2008). From this study, the highest number of subjects referred for sonography examinations for symptoms related to PID, were those within the age range of 21 to 30 years. This is the sexually active group and this finding is similar to that of Njoku et al. (2008) which noted higher prevalence of PID in women within the age range of 20 to 30 years. Common microbial organisms isolated from the HVS specimen were Staphylococcus species, Candida albican and Streptococcus species. The findings are similar to that of Njoku et al. (2008) and Olowe et al. (2012) but differ from that of the Centre for Disease Control and Prevention that were predominantly N. gonorrhoea and C. trachomatis. However, failure to isolate Chlamydia may be in keeping with previous observations that it does not readily grow on culture. Common microbial organisms isolated from the urine culture were Staphylococcus species and Streptococcus species.
There was no significant (p > 0.01) correlation between ultrasound diagnosis and HVS culture diagnosis of PID. No significant correlation existed between ultrasound diagnosis and urine culture diagnosis of PID. This can be attributed to the following reasons:
1. Ultrasound finding is not specific to any particular disease condition and because of this the features presented in ultrasound which is indicative of PID can also be indicative of other diseases or physiological processes for example fluid in the pouch of Douglas which is the commonest sonographic feature that is positive for PID (Njoku et al., 2008), can also be seen during the ovulatory period of the female because as the graffian follicle ruptures, fluid is also released which collects in the pouch of Douglas. Fluid collection might also be as a result of inflammation of organs surrounding the female reproductive organ.
2. The stage of the disease (PID): The findings on pelvic sonograms frequently appear normal in the early stages of PID or in uncomplicated conditions (Patter, 2007). This can lead to a negative diagnosis by ultrasound investigation, but on investigating using other diagnostic methods, for example Laboratory HVS culture, the result might be positive.
The results show that the accuracy of ultrasound diagnosis of PID is 89.2%, while the specificity of ultrasound diagnosis of PID is low (65.8%). This may be due to the stage of infection at the point of diagnosis. Ultrasound findings may be nonspecific in early or mild PID and correlation with clinical and laboratory findings is helpful to increase accuracy. Equipment quality and sonographer experience affect the sensitivity and specificity of sonography (Anjali, 2015).
This shows that it is not specific in PID diagnosis because there were a high number of false positive results according to the study. This implies that ultrasonography cannot be used as a confirmatory test in the diagnosis of PID but it should be used instead as a first line of investigation (screening tool) for PID diagnosis before other investigations should be carried out. This finding agrees with that of Njoku et al. (2008).
CONCLUSION
There is no significant correlation between ultrasound diagnosis of PID and findings from HVS culture and urine culture. No single diagnostic test has adequate sensitivity and specificity to diagnose PID.
RECOMMENDATION
The researchers wish to make the following recommendations:
1. Ultrasound, HVS culture and urine culture investigations should be carried out by qualified and experienced Sonographers /Sonologists and laboratory Scientists in order to facilitate accurate diagnosis.
2. When in doubt, further investigations using other diagnostic methods should be used in the diagnosis of PID.
3. It is very necessary to establish routine pelvic ultrasound scanning in females of reproductive age for early diagnosis of PID before it gets complicated.
4. The efficiency of record keeping both at ultrasound unit and medical records departments should be improved.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ash M (2006). Gynaecology by ten teachers.18th ed.London Hodder Arnold. 171-175. |
|
|
Blenning CE, Muench J, Jadkins DZ, Roberts KJ (2007). Clinical Inquieries. Which tests are moet useful for diagnosis of PID. J. Fam. pract. 56(3)216-220. |
|
|
Centre for Disease Control and Prevention (CDC)(2011). Pelvic inflammatory disease (PID)-CDC fact sheet. Atlanta, GA: US Department of Health and Human Services. |
|
|
Dayan L (2006). Pelvic inflammatory. Aust. Fam. Phys. 35:858-62. |
|
|
Eckert LO, Hawes SE, Wölner-Hanssen PK, Kiviat NB, Wasserheit JN, Paavonen JA, Eschenbach DA, Holmes KK (2002). Endometritis; the chemical pathologic syndrome. Am. J. Obstetr. Gynaecol. 186(4):690-695. |
|
|
Grodstein F, Rothman KJ (1999). Epidemiology of pelvic inflammatory disease. Epidemiology 45:234-42. |
|
|
Lon N, BroutetN, Adu-SarkodieY, Barton P, Hossain M, Hawkes S (2006). Global control of sexually transmitted infections. Lancet 368(9551). |
|
|
Horrow MM, Rodgers SK, Naqvi S (2007). Ultrasound of pelvic Inflammatory Disease. Ultrasound Clin. 2(2):297-309. |
|
|
Monica C (2000). District laboratory practice in tropical countries. London, Cambridge University press. 90-2,116-124. |
|
|
Njoku J, Agwu KK, Idigo FU, Ogbu SO (2008). The value of transabdominal sonography in the diagnosis and management of pelvic inflammatory disease. N Nigerian J. med. imaging and radiation therapy 1(1):24-29. |
|
|
Olowe OA, Alabe A, Akinde AA (2012). Prevalence and pattern of bacterial isolates in cases of pelvic inflammatory disease patients at a tertiary hospital in Oshogbo, Nigeria. Environ. Res. J. 6(4):308-311. |
|
|
Jaiyeoba O, Soper DE (2011). A practical approach to the diagnosis of pelvic inflammatory disease. Infectious Diseases in Obstettr. Gynaecol. 2011:753037. |
|
|
Patter RM (2007). Correlation of laparoscopic findings with endovaginal sonography in the diagnosis of PID. CNE Crade. s 10(5):3-4. |
|
|
Roses J (2001). Pelvic inflammatory disease. BMJ. 322:658-659. |
|
|
Agarwal A (2013). Imaging in pelvic inflammatory disease and tuboovarian abscess. Available at: http://telradsol.com/imaging-in-pelvic-inflammatory-disease-and-tubo-ovarian-abscess/ |
|
|
Simms I, Stephenson JM, Mallinson H, Peeling RW, Thomas K, Gokhale R, Birley H (2006). Risk factors associated with pelvic inflammatory disease. Sexually transmitted infections, 82(6): 452-457 |
|
|
Soper DE (2010). Pelvic Inflammatory Disease. Obst. Gynecol.116 (2 pt 1):419-28. |
|
|
Timor-Tritsch IE, Rottem S (1987). Transvaginal ultrasonographic study of the fallopian tubes. Obstetr. Gynaecol. 70:424-428. |
|
|
Turzic M, Kocijancic D (2010). Pelvic inflammatory disease: Contemporary diagnostic and therapeutic approach.Srp Arh. Celok Lek. 138(9-10):658-663. |
|
|
Welner-Hanssen PK, Mardh PA, Svensson L, Westrom L (1983). Laparoscopy in women with chlamydial infection and pelvic pain: a comparison of patients with and without salpingitis. Obstetr. Gynaecol. 16(3):299-303. |
|
|
Wiesenfeld HC, Sweet RL, Ness RB, Krohn MA, Amortegui AJ, Hillier SL (2003). Comparison of acute and subclinical pelvic inflammatory disease. Sexually Transmitted Sexual Dis. 32(7):400-405. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


