Full Length Research Paper

ABSTRACT
Tonsillectomy has generally been regarded as an in-patient procedure. Presently though, due to rising costs and space constraints, it has increasingly became popular as a day case procedure world-wide. However, careful selection of patients is advised so as to avoid undue risks and possible resulting mortalities. To find out the suitability or otherwise of day case tonsillectomies in a resource poor country, taking note of possible complications arising from the surgeries and also pre-operative management modalities adopted to prevent these. Case notes of 52 Patients who underwent day case tonsillectomies and Adenotonsillectomies over a nine year period were reviewed. Indication for Surgery was recurrent tonsillitis for 11 (25.6) children and Adenotonsillar Hypertrophy for 32 (74.4%) children. The indication for surgery of all the adults was recurrent tonsillitis. Data extracted included age, sex, indication for surgery, procedure used for both Anesthesia and Surgery and complications arising from Surgery. 52 Patients met the criteria for day case surgeries. 43 (82.7) were Children and 9 (17.3%) were Adults. 49 patients (94.3) recovered well except 3 (5.7%) patients who had had complications and had to be admitted overnight afterwards. 1(1.9%) patient represented in the Hospital following earlier discharge for overnight admission. Day case Tonsillectomies/Adenotonsillectomies are relatively safe procedures especially when patients are carefully selected and pre-operative measures to encourage heamostasis instituted.
Key words: Day case, costs, tonsillectomies, complications, haemostasis.
INTRODUCTION
Tonsillectomy is generally accepted as an inpatient procedure due to risk of post-operative hemorrhage (AL- Shagahin et al., 2019). Due to rising cost of treatment also as average length of hospital stay previously was 3 days, tonsillectomy is now preferred as a day case procedure (Raymond, 1986; Kharytaniuk et al., 2015). Tonsillectomies and Adenotonsillectomies are among the common surgeries in otorhinolaryngologic practice (Onakoya et al., 2004). However, before embarking on a day case tonsillectomy, it is important that the candidates are carefully chosen from the pool of patients who are booked for Elective Tonsillectomies. This is to avoid undue risks and possible resulting mortalities. Day case tonsillectomies have become popular over the world, the rate of day case tonsillectomies in the USA is 89, Canada 67, Belgium 93% and it is slowly gaining ground in Nigeria. Researchers, therefore present their local experience which to the best of their knowledge is the first from Delta State Nigeria, and hope to encourage more ORL Surgeons in Nigeria to adopt this practice.
MATERIALS AND METHODS
This study involved a retrospective review of case notes of 52 patients who had elective day case Tonsillectomy/ Adenotonsillectomy done at a private facility in Warri Delta State, Nigeria from December, 2010 to December, 2019. These surgeries were all performed by a Chief Consultant ENT Surgeon who used the same protocol for all the patients. All patients had preoperative injection Dicynone administered, 250 mg for children and 500 mg for adults one hour prior to surgery. All the surgeries were performed via cold steel dissection. Boyles Davis mouth gag was inserted after patient had been anaesthetized.
The type of Anaesthesia used for all the patients was Total Intravenous Anaesthesia (TIVA) with Propofol/fentanyl combination at induction and Endotracheal (orotracheal) intubation. Maintenance of Anaesthesia was with Propofol infusion, while analgesia was with intravenous diclofenac. After the insertion of the Boyles Davis mouth gag with an appropriate sized tongue plate, the soft palate was retracted, and the post nasal space inspected. Adenoids were then curetted out and tonsils dissected out, Haemostasis was secured with pressure packs and when needed suture ligatures were placed to secure bleeders. Anaesthesia and Surgery lasted between 30 min to 45 min. Patient was observed for a period of at least 6 to 8 h post-surgery and oral intake (cold soft diet) was commenced immediately patient was fully awake. Patient was then discharged home with strict instructions to present back in the clinic in the event of signs of bleeding, disorientation or refusal of feeds.
Criteria for choosing the cases
1) Patients must be over 3 years
2) ASA 1 and11
3) The distance/travel time of maximum of 30 min from the Hospital, which means that they must be resident in Warri (Hanss et al., 2011; Wong et al., 2016).
RESULTS
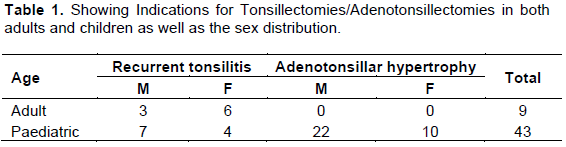
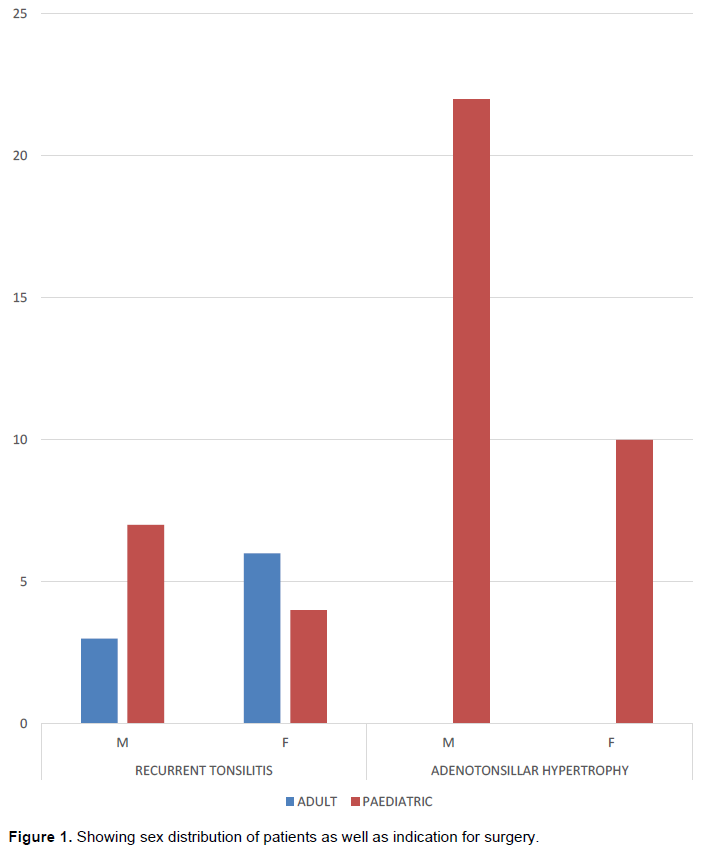
52 patients during this period met the criteria for Day Case surgeries. The 52 patients 9(17.3) were adults and 43 (82.7%) were children. Indication for surgery was recurrent tonsillitis for 11 (25.6) children and Adenotonsillar Hypertrophy for 32(74.4%) children. Table 1. The indication for surgery for the adults was recurrent tonsillitis. 49 patients (94.3) Figure 1 recovered well except 3 (5.7%) patients who had complications and had to be admitted overnight afterwards. 1 (1.9%) patient, presented back in the Hospital following earlier discharge for overnight admission.
DISCUSSION
Day case surgeries are usually selected procedures not considered high risk and usually the goal is both to minimize cost for the patient and in Government centers with few in-patient admission facilities, create room for more morbid cases (Abdulkareem, 2011).
In Nigeria, patients usually pay out of pocket for their medical bills and in situations where there is insurance cover, surgeries like tonsillectomies are not usually covered. In such situations, day case surgeries become desirable in order to reduce costs. Tonsillectomy, due to its high risk of both primary and reactionary haemorrhage (Adoga et al., 2008; Trinidade et al., 2014) which occur within 12 h following surgery, is considered an inpatient procedure, However when certain criteria are met, it can be considered as a day case procedure. These include patients over 3 years of age, American Society of Anaesthesiologist Physical Status (ASA) I and II, patients who reside within at least 30 min from the Hospital and patients are also required to have functional phone service. Obstructive sleep apnea is considered a contradiction (Kishore et al., 2001; Sanders et al., 2006).
To mitigate the risk of post-operative haemorrhage, each of these patients had routinely administered IV Dicynone (Ethamsylate) 250 mg for children and 500 mg for Adults as premedication 1 h before surgery. Dicynone (Etamsylate) is an antihaemorrhagic agent which is believed to work by promoting platelet adhesion. Studies done had looked at the effectiveness of dicynone in reducing blood loss at Surgeries and observed that there was significant reduction in frequency of secondary haemorrhage following adenotonsillectomy in children when they were administered preoperative dicynone (Garay et al., 2006; Arora and Manford, 1979). Thus they therefore inculcated the use of Dicynone into their preoperative protocol as a safety measure and safeguard against postoperative haemorrhage in these patients.
All patients also had pre-operative intravenous prophylactic antibiotic, intravenous ceftriaxone administered also 1 h prior to surgery. All patients were screened for bleeding disorders and had blood grouping and cross matching done. Majority (82.7%) of all the cases were children. This agrees with several earlier studies done of these 32(74.4) had adenotonsillar hypertrophy, and 11 (25.6%) recurrent tonsillitis as the indication for surgery. 49(94.3%) of the patients had good outcomes, commenced oral intake few hours after surgery and were discharged home on oral medication. 3(5.7) had prolonged recovery from anaesthesia which necessitated their being admitted overnight, whilst 1(1.9%) after being discharged presented back with vomiting /refusal of feeds, however there was no active bleeding. Patient was readmitted, commenced on IV fluids, intravenous medications and eventually was discharged the next day. No mortality was recorded from day case tonsillectomy/adenotonsillectomy during this period.
CONCLUSION
The high success rate (94.8%) will lead researchers to conclude that Day Case tonsillectomies are relatively safe procedures. However it is pertinent to note that patients should be carefully selected and pre- operative measures to promote haemostasis is encouraged. They should be closely observed for a minimum of 6 h and should be tolerating orally without any sequela before they are discharged home.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abdulkareem IH (2011). Day Case surgery in Nigeria. Nigeria Journal of Clinical Practice 14(4)383-389 |
|
|
Adoga AS, Onakoya PA, Mgbor NC, Akinyemi OA, Nwaorgu OGB. (2008). Day Case Adenotonsillectomy: Experience of two private Clinics in Nigeria. Nigeria Journal of Medicine 17(3):299. |
|
|
AL-Shagahin HM, ALBtoushO, Alrawashdeh B, ALsunna Z, Ababseh S. (2019) Day Case tonsillectomy in Children: Experience from a Teaching Hospital in Jordan. International Journal of Surgery 19:1-4. |
|
|
Arora YR, Manford MLM (1979). Operative Blood loss and frequency of Haemorrhage associated with Adenotonsillectomy in Children. A double blind trial of Ethamsylate. British journal of Anaesthesia 51(6):557-561. |
|
|
Garay RP, Chiavaroli C, Hannaert P (2006). Therapeutic Efficacy and Mechanism of action of Ethamsylate, a long standing Hemostatic agent American Journal of Therapeutics 13(3):236-247. |
|
|
Hanss J, Nowak C. Decaux A. Penon C, Bobin S (2011). Outpatient tonsillectomy in children: a 7 year experience . European Annals of Otorhinolaryngology, Head and Neck Diseases 128(6):283-289. |
|
|
Kharytaniuk N, ALR Sharafa A, Keogh IJ (2015). Day Case tonsillectomy: practical solution or practical impossibility. Irish Medical Journal 108(1):11-13. |
|
|
Kishore A, Haider- AL, Gedded NK (2001). Patient Eligibility for day case PaediatricAdenotonsillectomy Clinical Otolaryngology and Allied Sciences 26(1):47-49. |
|
|
Onakoya PA, Nwaorgu OGB, Abja UM, Kokong DD (2004). Adenoidectomy and Tonsillectomy: is clotting relevant. Nigerian Journal of Surgical Research 6(1-2). |
|
|
Raymond CA.(1986) Study Questions. Safety economic benefits of outpatient tonsil/ Adenoid Surgery. JAMA 256(3):311-312. |
|
|
Sanders JC, King MA, Mitchel RB, Kelly JP (2006). Perioperative complications of Adenotonsillectomy in children with Obstructive sleep apnea syndrome. Anesthesia and Analgesia 103(5):1115-1121. |
|
|
Trinidade A, Phillips JS, Bath AP. (2015). Day Case Tonsillectomy: Is the NHS demanding unobtainable target. The Bulletin of the Royal College of Surgeons of England 96:188-190. |
|
|
Wong HT, Sien Hu T, Chong AW (2016). Is Day Care tonsillectomy safe. Iranian Journal of Otorhinolaryngology 28(86):183. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


