ABSTRACT
Sexual abuse of children is very prevalent in Ghana. The pandemic has been a worrying phenomenon to parents, community leaders and government in recent years because of increasing cases of the phenomenon. This study purposed to determine the common causes of child sexual abuse and the effect on children. The study also concerned itself with community knowledge, attitude and care toward child sexual abuse. Data were collected from May to June 2019. 500 opinion leaders were used for the study because of their special role as communicators and leaders in community issues. Adopting a cluster sampling technique, the author conducted a household survey on 25 communities using a five Likert scale questionnaire. Analysis of data was by the factor analysis which was used to assess associations between factors and community orientation towards sexual violence against children. The study identified weak family structure, low level of education, family’s inability to meet children economic needs and age as the common factors of child sexual abuse. The study again found withdrawal from family and friends and some physical disorders as effects of child sexual abuse. Also, it was clear from the study that community’s orientation is measured by its knowledge, attitude and care of the children. Another significant finding was that community’s knowledge and concern for children promote community orientation and subsequently reduce child sexual abuse and its associated outcomes. The study recommended to one toward care and attention to children at the community level, and strict application of sanctions against offenders at the local and national authority levels.
Key words: Attitude, child sexual abuse, community, community knowledge, community orientation.
To improve the quality of an organization and increase customer satisfaction with the products, marketers have always adapted approach that helps update and match the characteristics of their products to the needs of customers (Ranjbar et al., 2018). In a similar vein, since the primary customers of every community is the people (both adult and children), and paying attention to the community’s needs and expectations are among the immediate and primary prerequisites for community development (Gorji et al., 2017), community-oriented quality improvement models can serve as a tool for measuring quality life for children who are future leaders. It could also help in continuous needs assessment and understanding children’s requirements with the community knowledge, attitude, care and support (Arefi and Zandi, 2011). The community faces a challenge of contributing to fulfilling the goal to the children with the accurate knowledge, right attitude and right support that give the needed protection to children (Svensson et al., 2018; Nguyen et al., 2007).
A community may be defined as the population that might provide care, including both children and adult. It involves people who are linked geographically, socially, culturally and ethnically; and might share common values, experiences, language or religion (Institute of Medicine, 1977). In this connection, it should be possible for a well-knit community to provide effective care and support for its members, especially the children who are the most vulnerable in society. Just as market orientation is used to study the product and service market (Jaworski and Kohli, 1993), so is its analogous concept, community orientation used to study the people of the community as patrons (Gorji et al., 2017). Therefore, in this conceptualization, community orientation might refer to care providers’ knowledge of community needs and involvement in the community (Muldoon et al., 2010). Proenca (1998:29) defined community orientation “as the generation, dissemination, and utilization of community intelligence to address current and future health needs.
Community orientation is thus a fundamental aspect of community care and support (Dahrouge and Hogg, 2010). Researchers and opinion leaders see community orientation as important for recognizing and addressing social and environmental issues affecting a community through accurate knowledge of the community and actions and partnerships at the community level. Community orientation helps improve the recognition, prevention and management of social vices, including child sexual abuse through knowledge of all members of the community in general and opinion leaders and in particular (Muldoon et al., 2010).
For this study it’s define community orientation as all the actions taken by a community to support and provide community care in considering children’s needs and welfare as a major priority. Community orientation may involve factors that help in developing accurate knowledge of issues confronting children, positive attitude toward children and issues related to children in order to provide care and support for children. Such a model must enable the community’s prompt and indiscriminate response to all community complaints and queries regarding child sexual abuse; and dealing with all other related child violation issues. The article conceptualises that, the degree of community orientation determines the effect of child sexual abuse. Therefore, this research examines the common causes of sexual abuse among children and the effect such abuse has on them, and how community orientation moderates the ultimate outcome. This study is a necessity because while most of the studies in this field concern themselves with just the health and medical outcomes, this current study extends the discussion to the marketing and social field. It is significant to review a few literatures to explain some critical concepts related to this study, and to develop a model for the conceptualization.
Child sexual abuse
This concept refers to any sexual act against a minor, or between two minors, in which the older coerce the younger to having sex. It may also include exposing children to pornography or engaging in oral sex (Townsend and Rheingold, 2013). Most communities underestimate the importance of protecting children and their sexuality. Studies show that about 10% of children would suffer sexual abuse before their age 18 (Townsend and Rheingold, 2013). Studies have revealed that children are the most sexually abused group in society (Townsend and Rheingold, 2013). Offender usually is relatives or members close to the victim’s family (Whealin, 2007). Strangers make up just about one-tenth of those who violate children (Finkelhor, 2012). People, who the family trust, turn to abuse the children (Townsend and Rheingold, 2013).
Sexual abuse is a global phenomenon, and Ghana is no exception from other developing economies. Statistics showed 5,752 defilement cases in Ghana between 2010 -2014, with 342 of the cases perpetrated by family members of the victims. The Domestic Violence and Victim Support Unit (DOVVSU) of the Ghana Police Service reported 1,298 cases of defilement in 2014 with only eight of the victims being males. In 2013, the country reported 1,230 defilement cases, 1,097 cases in 2012 and 1,159 defilement cases in 2011 and 968 cases in 2010. These statistics do not include a good number of abuse cases that were not reported to the police. The central region had the most reported cases, making it a region of interest for scientific investigation.
Factors of child sexual abuse
The first cause of sexual abuse in children is “grooming”. This is when offenders form relationships with potential victims and their families prior to the abuse (Sedlak et al., 2010). Grooming is an act whereby the offender cunningly and secretly engages his victim into a sexual relationship. The process may start with the offender performing certain deeds for the victim and her family, making the family develop trust and respect for him. Grooming is hatched and sustained by the offender paying special attention and showering gifts; being at isolated places with the innocent child. It may also include providing the needs of the child which the family is not providing; treating the child as if he or she is older; and use of threats to keep the relationship secret. Even though every child is at risk when it comes to sexual abuse, some are more susceptible to risk because of certain prevailing factors. The factors may include the family structure. When children live with both parents the risk of being sexually abuse is low. On the other hand, children in divided homes stand a higher risk of being victims of sexual abuse (Sedlak et al., 2010). Children living with people other than their parents also risk suffering abuse. Children who live with a single parent that has a live-in partner are at the highest risk to be victims of child sexual abuse than children living with both parents.
Regarding gender and age, females suffer abuse than males (Finkelhor, 1994), and the younger child are more vulnerable to abuse (Finkelhor, 1994; Putnam, 2003). In average, 20% of sexually abused children are aged eight years or younger (Snyder, 2000). Socio-economic background of families also influences a child risk to sexual abuse. Children in economically poor households risk sexual abuse; and when such children live in rural areas, the risk is even higher (Sedlak et al., 2010). Other studies have averred that victims have always been younger than the perpetrators (Sweet and Welles, 2012; Lambert and Andipatin, 2014). The innocence and weakness of children expose them to abuse by merciless offenders (Mathoma et al., 2006). The offenders use threat to persuade the children to have sex with them (Pasura et al., 2014). Trusted friends and acquaintance take advantage of specific characteristics in the children they abuse and exploit them. These offenders target the passive, quiet, troubled and lonely children as easy prey for sexual abuse (Elliott et al., 1995). Perpetrators seek children who are trusting, find new ways to establish a trusting relationship before abusing them (De Bellis et al., 2011). The level of literacy of the child can also be a contributing factor of sexual abuse. The literature shows that a child’s knowledge toward sexuality in the community varies with the child’s educational level. Education increases knowledge and awareness toward child sexual acts (Johnson, 2004).
Effects of child sexual abuse
Researchers have identified emotional, mental and health problems, academic problems in childhood, physical problems beginning in childhood or adolescence, as some immediate outcomes of child sexual abuse. For instance, victims suffer physical aggression, non-compliance, and oppositional behaviours (Noll et al., 2007). The literature shows that victims of sexual abuse often perform badly in a test measuring cognitive ability and academic achievement compared to their non-abused counterparts (Wells et al., 1997). Studies have also found adolescents victims of sexual abuse to use drugs (Briere and Elliott, 2003). Child sexual abuse has some other lasting consequences for victims. Victims are more likely to develop psychiatric disorders (Kendler et al., 2000). They may also experience bruising, bleeding, redness and bumps, or scabs around the mouth, genitals, or anus, urinary tract infections, sexually transmitted diseases, and abnormal vaginal or penile discharge. Victims may also show signs of anxiety, chronic stomach pain, headaches and age inappropriate language (Leeb et al., 2011; Olafson, 2011; Girardet et al., 2009).
Certain barriers might moderate factors of child sexual abuse to minimise the effect on the victim. This means the higher the level of community orientation would determine occurrence and effect of child sexual abuse. Previous studies estimate that only a third of child sexual abuse cases come to light, and they report even fewer. It is estimated that about 38% of children have suffered sexual abuse (Ullman, 2007). This means few of the victims do report any sexual abuse incidents (Finkelhor, 2012), which would affect the effectiveness of community orientation toward child sexual abuse. The literature also suggests that children either delay or never report their sexual violation experiences (Foster and Hagedorn, 2014), because in most cases they fear the community would not believe them (Cossar et al., 2013). Sometimes children cannot report their sexual experience either to avoid shame or self-blame (Schaeffer et al., 2011). Another barrier is the rape myth, where the community blame children for inviting abuse by their actions instead of taking practical action against offenders (Carmody and Washington, 2001). Common rape myths include blaming children for their dress covering abuse by acquaintances and paying attention to only abuse that results in physical damage to the child (Pasura et al., 2014).
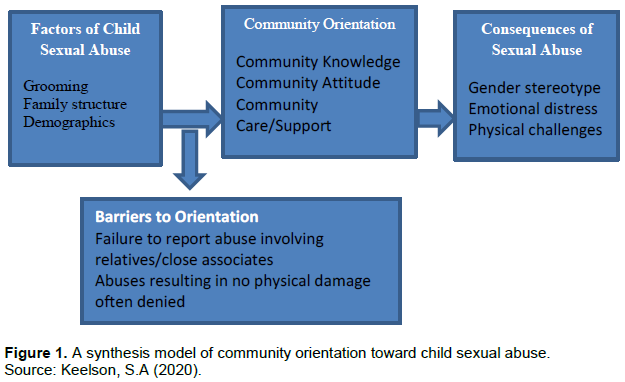
A synthesis model of community orientation towards child sexual abuse
A careful consideration of the literature, suggests that community orientation toward child sexual abuse refers to the level of knowledge toward the abuse in any form, the attitude and care/support provided. Thus, the higher and the more accurate the knowledge of what make up child sexual abuse, the better the community orientation toward child sexual abuse. Based on the literature and the findings of the current study community orientation toward child sexual abuse may be defined as the factors that influence child sexual abuse, how the level of community orientation - moderated by barriers to community orientation, determines the consequences of child sexual abuse. From Figure 1, the current article reveals that the factors of sexual abuse define the existing issues that trigger child violation by offenders. As supported by the literature, factors such as ‘grooming’ (Sedlak et al., 2010) or how the potential perpetrator forms a relationship with the child and/or the family, the structure of the family as single or both parent taken care of a child, demographic factors such as gender, age of the child, educational level of the victim (Sweet and Welles, 2012; Lambert and Andipatin, 2014) make up potential threats or otherwise for child sexual violation. The extent to which the communities manage and address the factors depends on the level of community-oriented behaviour, including the community knowledge, attitude and immediate care/support (Choo and Dunne, 2011). Again, certain barriers moderate the level at which factors of sexual abuse influence community orientation to determine the consequences of sexual abuse. These include, whether children delay in reporting or even never at all report sexual encounters (Foster and Hagedorn, 2014). It also includes the degree to which the community shows genuine belief in victims who report sexual abuse cases, the widespread belief in rape myth and gender stereotype (Pasura et al., 2014). Depending on the level of community orientation at work, child sexual abuse may have rare consequences including emotional and physical consequences (Broman-Fulks et al., 2007; Leeb et al., 2011; Olafson, 2011).
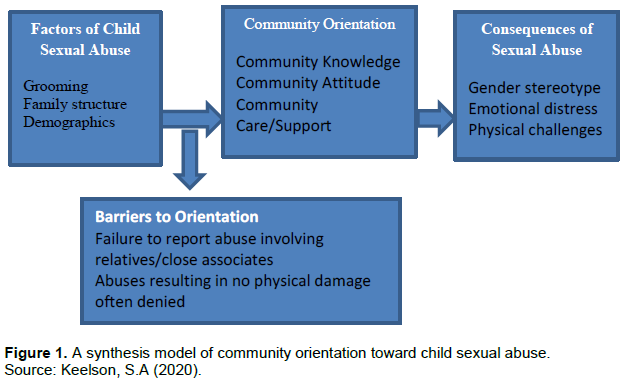
A cursory consideration of the existing literature shows that the prevailing nature of child sexual abuse in the communities results from certain factors, which strengthen or otherwise influence the level of community orientation. Some barriers ultimately moderate the outcome of community orientation and create different degrees of consequences on the communities. This article conceptualized that unlike previous studies; a modicum of factors affects the level of community orientation toward child sexual abuse and also generates several consequences at the same time. The author recommends this synthesis study to develop a model that can transcend different variables and study contexts, since such a study is under-researched. Therefore, the purpose of the current study is to develop a synthesis model (Figure 1) that explains how factors of child sexual abuse when influenced by community-oriented behaviour, is moderated by certain factors to determine the level of consequences of child sexual abuse. This article addresses the following specific objectives:
1) To examine factors affecting community orientation toward child sexual abuse
2) To determine the level of community orientation toward child sexual abuse in the Central Region of Ghana
3) To evaluate barriers moderating the community-oriented behaviour of child sexual abuse
4) To examine the consequences of child sexual abuse in
the community
5) To develop a synthesis model of community orientation toward child sexual abuse
6) We devote the rest of the article to describe the method, Results and discussions of data, and conclusions and limitations of the study.
The scope of study is Central Region of Ghana with a population of about 2.56 million of which 42% were 16 years or younger (Statistical Service Estimates, 2019). The choice of the region for the study is because of its recent continuous reports of abuse of children, some even less than 5 years.
This has put the region in the limelight as a notorious area for child sexual abuse in the country. The sampling unit of the study included opinion leaders of the target communities. Opinion leaders were used as unit of analysis because of the information role in society. Cluster sampling was used to select 25 communities from the about 200 communities. The sampling method devoted to the study was to enable the researcher select communities in clusters using community size, urbanization and level of commercial activities. Opinion leaders were classified by their community affiliation, religious affiliation and educational affiliation. Then, stratified sampling technique was used to select respondents from the three strata of opinion leadership, while we used ‘leads’ in the communities to trace informants. 500 respondents were selected from the communities and used Likert scale questionnaire for data collection. The study used factor analysis technique for data analysis. Factor analysis is a statistical method used to describe variability among observed, correlated variables in terms of a lower number of unobserved variables called factors. Factor analysis (including common factor analysis and principal component analysis) helped to examine the interdependence among variables and to explain the underlying common dimensions (factors) for the correlations among the variables. The procedure allowed the researcher to condense the information in an extensive set of variables into a smaller set of variables by identifying some underlying dimensions and variables that influence them. The study could therefore look upon the underlying dimensions or factors, which are of primary interest but unobservable, as the additional set of variables. Factor analysis facilitates the transformation from the original observable variables to the new variables (factors) with as minor loss of information as possible (Everitt and Dunn, 2001).
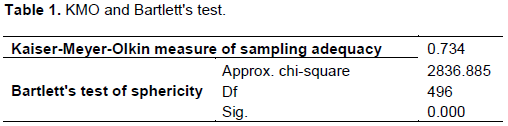
Table 1 shows the KMO measure and the results of the Bartlett’s test, which are used to judge the adequacy of the sample size and whether the correlation matrix is suitable for factor analysis. Both the KMO value of 0.734 (which is greater than the minimum threshold of 0.50 (Sharma, 1996) and the Bartlett’s test ? value of 0.000 suggest the sample size is adequate and that, at least, some variables are inter-correlated and therefore the data were suitable for factor analysis.
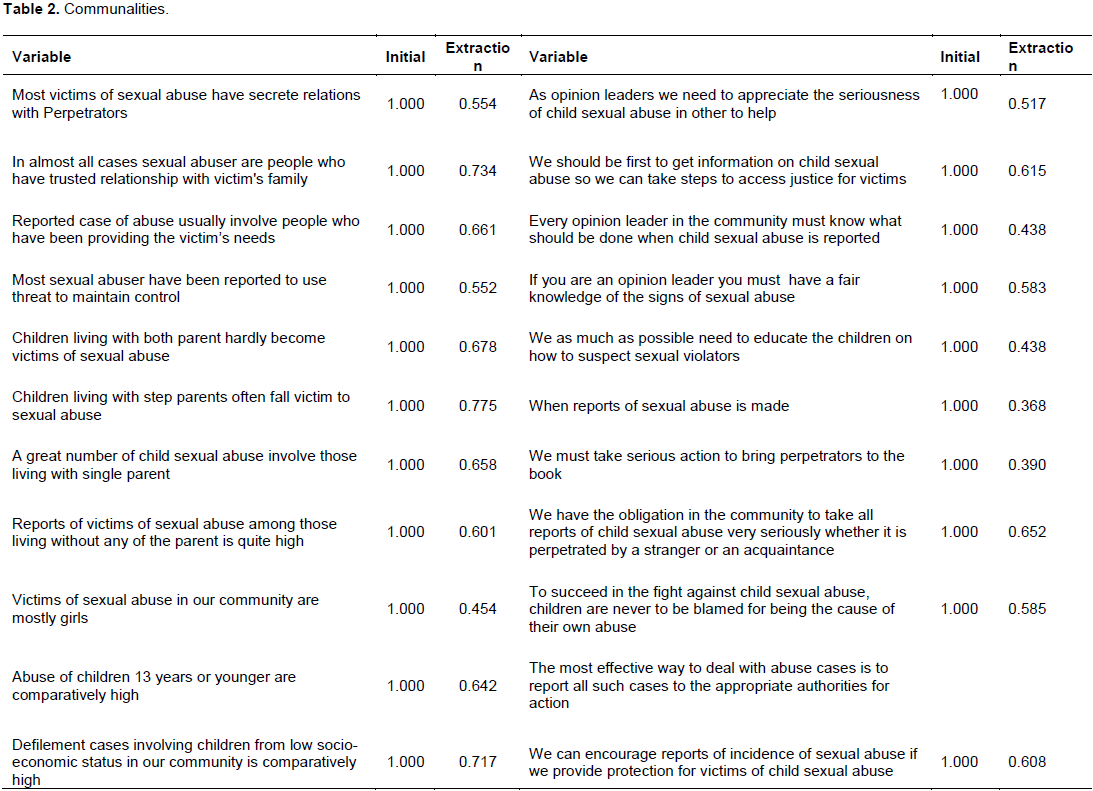
Table 2 shows the initial and final (Extraction) communalities in PCF, all variables assigned are initial variance (total communality) of one, as stated in the Table 2. The final (Extraction) communalities of each variable represent the variance accounted for by the chosen factor solution for the variable. Twenty-two variables remained in the ultimate factor solution out of the 32 variables at the start of the analysis. The other ten were removed from the analysis because their communalities were less than 0.50 or they were cross-loading (loading on over one factor) in the preliminary analysis. From Table 2, all the final communalities are at least 0.50. At least 50% of the initial communality of each variable was accounted for in the final factor solution. The factor solution is considered being satisfactory as at least half of the variance of each variable is shared with the factors.
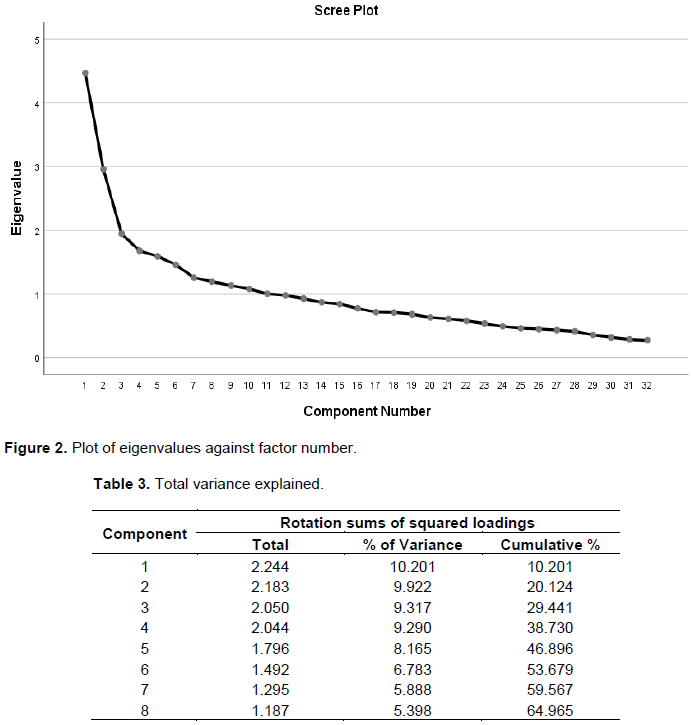
Number of factors extracted
Three criteria were used to decide on the number of factors to keep for interpretation: eigenvalue-greater-one rule, scree plot and the percentage of variance explained. Eight components have eigenvalues greater than one, so going by eigenvalue-greater-one rule; it can retain eight factors for interpretation. The scree plot of Figure 2 suggests extracting six factors as the plot straightens out after the sixth component. However, the first six factors explain 53.86% of the variance in the data while the first eight components account for 64.97% more than the suggested 60% threshold (Hair et al., 2006). Thus, eight components were retained for this work (Table 3).
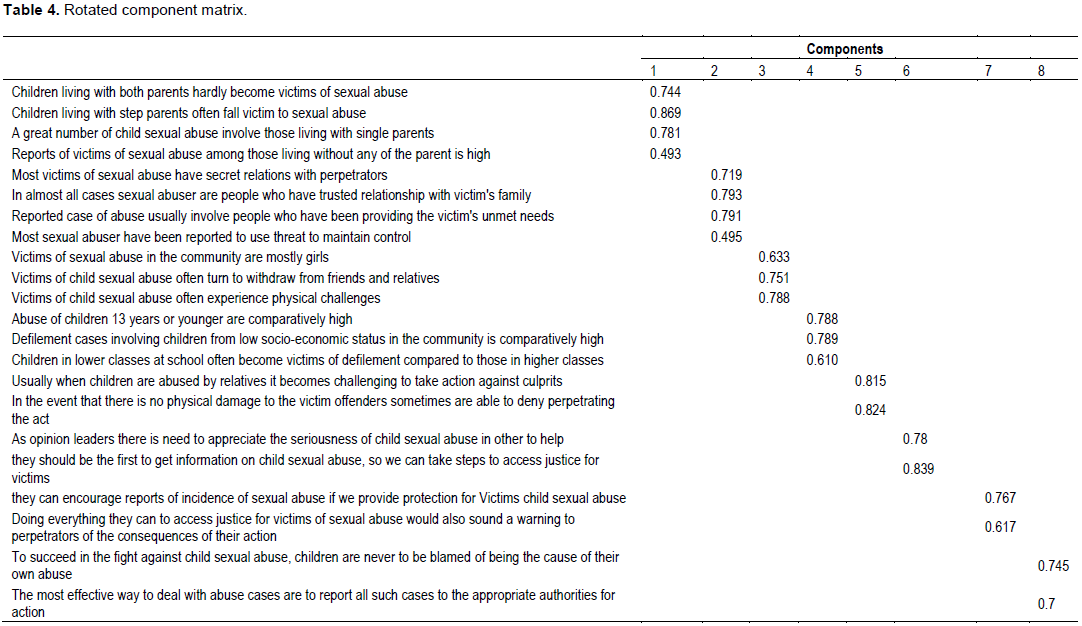
Table 4 shows the extracted factors and the loadings of the various variables on the factors, after it had rotated the initial factor solution via the Varimax method so that each variable load highly on only one factor. The method also ensures that the factors are uncorrelated. As stated in Table 2, the loadings represent the extent of correlation between a variable and a factor. The higher the absolute value of a loading of a variable on a factor, the more influential the variable is on the factor. A loading of 0.40 is considered significant for a sample size of 500 (Hair et al., 2014). However, a higher value of 0.50 was used to ensure that only variables of practical significance were included in the final factor solution. Loadings below 0.50 were omitted, with the remaining ones sorted in descending order of magnitude to facilitate easy interpretation of the final factor solution. Factors (Components 1, 2, 3……, 8 (Table 4)) are presumed to be the underlying dimensions informing the development of a synthesis model of community orientation toward child sexual abuse. We named the factors based on the loadings of the variables shown so that the higher the absolute value of a variable’s loading on a factor; the more influential the variable is in naming the factor. The factors are named as follows:
Factor 1: Family structure
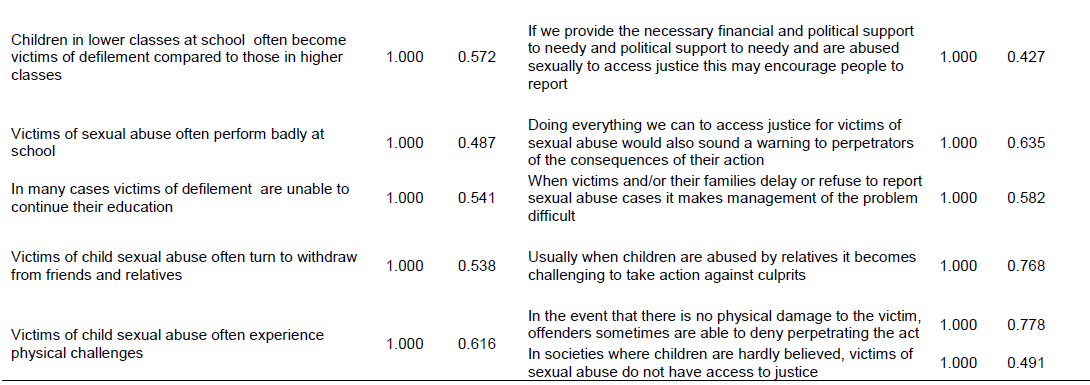
Living with both parents reduces the chances of being sexually abused to a very high degree. Victims are 74% protected, with about only 25.6% being at risk. Children living with step parent are at higher risk (86.9%) of being victims of sexual abuse. Children living with only one parent are highly (78.1%) subject to risk of being sexually violated. Those living with people other than their parents have a lower risk (49.3%) of sexual violation
Factor 2: Grooming
There is usually a high possibility (71.9) that children who are abused often have a secret relationship with offenders. People who the victims trust, form a greater percentage (79.3%) of sexual abuse offenders. In many a case (79.1%) of people who have been providing the unmet needs of the victims abuse the children. Use of threat by offenders to maintain control over their victims account for a reasonable case (49.5) of child sexual abuse
Factor 3: Consequences of child sexual abuse
Girls are at higher risk of being sexually abused (63.3%)
There is greater possibility that (75.1%) of victims withdrawing from friends and relatives after such a bitter experience. In 78.8% of the sexual abuse cases, victims experience physical challenges.
Factor 4: Demographic
Children 13 years or younger are at higher risk (78.8%) of being sexually abused. Coming from a low socio-economic background put children to a high risk of being sexually violated. That is about 78.9% risk. There is a high risk of children at lower classes at school to suffer abuse; about 61% in most of the cases.
Factor 5: Moderators to community orientation toward child sexual abuse
Victims of sexual abuse do not report about 81.5% of the cases because offenders are relatives or close associates. In 82.4% of the cases where victims do not suffer any physical damage, perpetrators often deny committing the offense.
Factor 6: Community knowledge
Opinion leaders’ appreciation of child sexual abuse goes a long way to manage sexual abuse (about 78% in most of the cases). Community leaders’ ability to generate adequate and timely information on child sexual abuse is a sure way of dealing with issues of abuse in the communities. It accounts for about 83.9% success.
Factor 7: Care/support
Provision of protection for victims of child sexual abuse has a high rate (76.7%) of encouraging victims to report incidence of abuse. Doing everything within their power as opinion leaders to access justice for victims of child sexual abuse is a primary means of sounding warning to perpetrators and providing significant care and support for victims.
Factor 8: Community attitude
When the community refrains from blaming victims as cause of their own sexual abuse, it contributes to the fight against child sexual abuse. Such an attitude has 74.5% potential success.
If the community develops a positive attitude of reporting all abuse cases to the appropriate authorities, there is a 70% probability of success in managing child sexual abuse.
The findings have shown that factors such as victim’s secret relation with offenders, offenders providing victim’s unmet needs, offenders use of threat, children living with step parent or single parent, children 13 years or younger, children from low socio-economic background are more susceptible to sexual abuse. The findings of the current study are consistent with other similar studies (De Bellis et al., 2011; Sweet and Welles, 2012; Lambert and Andipatin, 2014; Pasura et al., 2014). These studies also found the identified variable as factors affecting child sexual abuse. The finding and the previous research suggest that the communities can reduce incidence of child sexual abuse if much emphasis is placed in protecting children from low-economic background, very young children and children with single or step parents.
The study also showed a high level of community orientation toward issues relating to the child. All the three-primary community-oriented variables, including community knowledge, community attitude and community care/support for children were present. Thus, the findings reveal that community leaders are always ready to take action against offenders, opinion leaders also generate accurate and timely information on abuse cases, while the community do well not to blame victims of their sad sexual experience so they could report cases of sexual abuse. The community leaders find it necessary to report all abuse cases to the appropriate authorities for legal action, while providing protection and platform to access justice for victims. This shows that community knowledge, attitude and care/support define community orientation behaviour of child sexual abuse.
The result is consistent with (Othman and Jaafar, 2012), who identified parents and opinion leaders’ attempt to create public awareness as a necessary action for community orientation; and Mathoma et al. (2006), who showed that the individual’s ability to identify and define child sexual abuse depends on the person’s knowledge and understanding of the situation. In this connection, it can be concluded that the more opinion leaders take interest in the matters concerning children in their communities the more likely the country can reduce the pandemic. It is again clear from the findings that the community’s ability and willingness to report cases involving relatives and close acquaintances, and the extent to which the community can hold offenders responsible, when victims have no physical damage moderates the community reaction. This means the more the community is ready and able to report all cases, including those involving relatives, the higher the community orientation and the greater the possibility of fighting child sexual abuse. The more the community can determine sexual performance even when the offender denies because there is no physical damage, the more oriented the community will be to care for victims.
The study also supported the fact that child sexual abuse has gender, emotional and physical consequences. The results showed that girls are more subservient to child sexual abuse, and most of the victims turn to withdraw from friends and relatives, while others suffer physical consequences. This outcome is consistent with previous studies (Kendler et al., 2000) which averred that females who fall victim to sexual abusers are three times more likely to develop psychiatric disorders compared to males. It is also consistent with (Polusny and Follette, 1995; Young et al., 2007), who found that emotional and behavioural signals are common among sexually abused children. Some of these are withdrawal, fear, depression, unexplained anger and rebellion. It is however inconsistent with studies such as (Noll et al., 2007; Girardet et al., 2009) who found no behavioural problems, including physical aggression, non-compliance.
Based on the findings the author developed an empirical synthesis model of community orientation (Figure 1).
This paper reports on the results of an investigation aimed to understand what factors affect child sexual abuse in the central region of Ghana, and how community orientation influences such factors to contribute to certain outcomes. A questionnaire including, 32 items that used a five-point differential scale. it subjected a sample of 500 respondents who were opinion leaders to factor analysis. The KMO value of 0.73 and the ?-value of 0.000 for the Bartlett’s test of sphericity meant that the data was suitable for factoring. Combining three criteria to decide on the number of factors to retain for interpretation, the author arrived at an eight-factor solution, which accounted for 64.9% of the original variance in the data. A minimum threshold of a loading of 0.50 was used to include only variables with practical significance in the final factor solution, which resulted from rotating the initial factor solution by the Varimax method, ensuring that the factors in the final factor solution are uncorrelated. The dimensions adduced to be influencing the community orientation of child sexual abuse were: Family structure, Grooming, Consequences, Demographics, Moderators, Community knowledge, Community care/support and Community attitude. Community leaders and governmental authorities can focus on these dimensions as they strive to manage the child sexual abuse pandemic in the communities.
What makes this study different is that as far as the researcher is aware it is the first study to adapt marketing concept to study child sexual abuse in a manner such as this. It is also the first of its kind to have a synthesis study of community orientation and child sexual abuse to highlight factors, and consequences of child sexual abuse, and community’s responsibility in such detail. The current study is the first to develop a model of community orientation toward child sexual abuse.
The study showed that the communities with good knowledge on factors and consequences associated with child sexual abuse are more likely to manage and reduce abuse cases. The findings have important implications for interventions aimed to have a positive attitude toward child sexual abuse and offer appropriate support both at the community level and the government level. The results highlight the challenges associated with changing attitudes towards child sexual abuse and found women as those who need the highest levels of support. Support for the vulnerable and victims and appropriate sanctions for offenders by the communities and local government authorities would be commendable. Again, researchers can use the synthesis model to expand the frontiers of knowledge in the study of sexual abuse. However, the study uses only one region in Ghana. This begs from generalizing the results to different community and cultural settings. Thus, future studies could consider cross-cultural and cross-country studies to support generalisation. The study’s informants were only opinion leaders. While it is known that these have influence in the society, further studies may consider adding parents, guardians and even some sexual abuse victims.
The author has not declared any conflict of interest.
REFERENCES
|
Arefi M, Zandi K (2011). A Model for integrating quality improvement models: A customer-oriented approach to higher education. First international management conference, Future, Entrepreneurship and Industry in Higher Education, Sanandaj, Kurdistan University.
|
|
|
|
Briere J, Elliott D (2003). Prevalence and Symptomatic Sequelae of Self-Report Childhood Physical and Sexual Abuse in a General Population Sample of Men and Women, Child Abuse, Neglect 27(10):1205-1222.
Crossref
|
|
|
|
|
Broman-Fulks JJ, Ruggiero KJ, Hanson RF, Smith DW, Resnick HS, Kilpatrick DG, Saunders BS (2007). Sexual assault disclosure in relation to adolescent mental health: Results from the National Survey of Adolescents. Journal of Clinical Child and Adolescent Psychology 36(2):260-266.
Crossref
|
|
|
|
|
Carmody DC, Washington LM (2001) Rape myth acceptance among college women: The impact of race and prior victimization. Journal of Interpersonal Violence 16(5):424-436.
Crossref
|
|
|
|
|
Choo WY, Dunne M (2011). Victimization experiences of adolescents in Malaysia. The Journal of Adolescent Health 49(6):627-634.
Crossref
|
|
|
|
|
Cossar J, Brandon M, Bailey S, Belderson P, Biggart L, Sharpe D (2013). It takes a lot to build trust'. In recognition and telling: developing earlier routes to help for children and young people.
|
|
|
|
|
Dahrouge S, Hogg W, Tuna M, Russell G, Devlin RA, Tugwell P (2010).An evaluation of gender equity in different models of primary care practices in Ontario. BMC Public Health 10(1):1-12.
Crossref
|
|
|
|
|
De Bellis MD, Spratt EG, Hooper SR (2011). Neurodevelopmental biology associated with childhood sexual abuse. Journal of Child Sexual Abuse 20(5):548-587.
Crossref
|
|
|
|
|
Elliott M, Browne K, Kilcoyne J (1995). Child sexual abuse prevention: What offenders tell us. Child Abuse and Neglect 19(5):579-594.
Crossref
|
|
|
|
|
Everitt B, Dunn G (2001) Applied multivariate data analysis, Arnold; New York: Oxford University Press.
Crossref
|
|
|
|
|
Finkelhor D (1994). Current information on the scope and nature of child sexual abuse. The Future of Children, Sexual Abuse of Children 4(2):31-53.
Crossref
|
|
|
|
|
Finkelhor D (2012). Characteristics of Crimes Against Juveniles. Durham, NH: Crimes against Children Research Center.
View
|
|
|
|
|
Girardet RG, Lahoti S, Howard LA, Fajman NN, Sawyer MK, Driebe EM (2009). Epidemiology of sexually transmitted infections in suspected child victims of sexual assault. Pediatrics 124:79-84.
Crossref
|
|
|
|
|
Gorji AH, Darabinia M, Ranjbar M (2017). Relationship Between Emotional Intelligence and Job Motivation Among Faculty Staff in Mazandaran University of Medical Sciences, Iran. Iranian Journal of Psychiatry and Behavioral Sciences 11:2.
|
|
|
|
|
Foster J, Hagedorn W (2014). A Qualitative Exploration of Fear and Safety with Child Victims of Sexual Abuse. Journal of Mental Health Counseling 36(3):243-262.
Crossref
|
|
|
|
|
Hair F, Hult GTM, Ringle CM, Sartedt M (2014). A primer on partial least squares structural equation modeling. Thousand Oaks, CA: Sage.
|
|
|
|
|
Hair JF, Black WC, Babin BJ, Anderson RE, Tatham RL (2006). Multivariate data analysis (Volume 6). Upper Saddle River, NJ: Pearson Prentice Hall.
|
|
|
|
|
Institute of Medicine, National Academy of Sciences (1977). Primary Care in Medicine-A Definition. Washington, D.C.: Institute of Medicine.
|
|
|
|
|
Jaworski BJ, Kohl AK (1993). Market Orientation: Antecedents and Consequences. Journal of Marketing 57(3):53-70.
Crossref
|
|
|
|
|
Johnson CF (2004). Child Sexual Abuse. The Lancet 364(9432):462-470.
Crossref
|
|
|
|
|
Kendler K, Bulik C, Silberg J, Hettema J, Myers J, Prescott C (2000). Childhood sexual abuse and adult psychiatric and substance use disorders in women: An epidemiological and Cotwin Control Analysis. Archives of General Psychiatry 57:953-959.
Crossref
|
|
|
|
|
Kendler K, Bulik C, Silberg J, Hettema J, Myers J, Prescott C (2000). Childhood sexual abuse and adult psychiatric and substance use disorders in women: An epidemiological and Cotwin Control Analysis. Archives of General Psychiatry 57(10):953-959.
Crossref
|
|
|
|
|
Lambert C, Andipatin M (2014). An exploration of student perceptions of the risks and protective factors associated with child sexual abuse and incest in Western Cape, South Africa. African Safety Promotion Journal 12(1):35-51.
|
|
|
|
|
Leeb R, Lewis T, Zolotor AJ (2011). A review of physical and mental health consequences of child abuse and neglect and implications for practice. American Journal of Lifestyle Medicine 5(5):454-468.
Crossref
|
|
|
|
|
Ranjbar M, Morteza D, Alimorad HG, Seyyed MHA (2018). The Rules and Regulations of the Customer Orientation in Higher Education: Case Study Journal of Education and Human Development 7(2):59-65.
Crossref
|
|
|
|
|
Mathoma A, Maripe-Perera D, Khumalo L, Mbayi B, Seloilwe E (2006). Knowledge and perception of parents regarding child sexual abuse in Bostwana and Swaziland. Journal of Paediatric Nursing 21(1):67-71.
Crossref
|
|
|
|
|
Muldoon L, Dahrouge S, Hogg W, Geneau R, Russell G, Shortt M (2010). Community orientation in primary care practices: Results from the Comparison of Models of Primary Health Care in Ontario Study. Canadian Family Physician 56(7):676-83.
|
|
|
|
|
Nguyen TH, Sherif JS, Newby M (2007). Strategies for successful CRM implementation. Information Management, Computer Security, 15(2):102-115.
Crossref
|
|
|
|
|
Noll JG, Shenk CE, Putnam KT (2007). Childhood sexual abuse and adolescent pregnancy: A meta-analytic update. Journal of Pediatric Psychology 34:366-378.
Crossref
|
|
|
|
|
Olafson E (2011). Child sexual abuse: Demography, impact, and interventions. Journal of Child and Adolescent Trauma 4(1):8-21.
Crossref
|
|
|
|
|
Othman A, Jaafar W (2012). A preliminary Investigation: Children's Awareness of Child Sexual Abuse in Malaysia. International Journal of Social Sciences and Humanity 2(3):242-247.
Crossref
|
|
|
|
|
Pasura D, Jones A, Hafner J, Maharaj P, DeCaires K, Johnson E (2014). Competing meaning of childhood and the social construction of child sexual abuse in the Caribbean. Journal of Childhood 20(2):200-214.
Crossref
|
|
|
|
|
Schaeffer P, Leventhal JM, Andrea GA (2011). Children's disclosures of sexual abuse: Learning from direct inquiry, Child abuse & neglect 35(5):343-52.
Crossref
|
|
|
|
|
Polusny MA, Follette VM (1995). Long-term correlates of child sexual abuse: theory and review of the empirical literature. Applied and Preventive Psychology 4:143:166.
Crossref
|
|
|
|
|
Proenca EJ (1998). Community orientation in health services organizations: the concept and its implementation, Health Care Management Review 23(2):28-38.
Crossref
|
|
|
|
|
Sedlak AJ, Mettenburg J, Basena M, Petta I, McPherson K, Greene A, Li S (2010). Fourth national incidence study of child abuse and neglect (NIS-4).
Crossref
|
|
|
|
|
Sharma S (1996). Applied Multivariate Techniques. USA: John Wiley and Sons, Inc.
|
|
|
|
|
Svensson J, Baer N, Silva T (2018). Adolescents' level of knowledge of and supportive attitudes to sexual crime in the Swedish context, Journal of Sexual Aggression.
Crossref
|
|
|
|
|
Sweet T, Welles S (2012). Associations of sexual identity or same-sex behaviours with history of childhood sexual abuse and HIV/STI risk in the United States. Journal of Acquired Immune Deficiency Syndromes 59(4):400:408.
Crossref
|
|
|
|
|
Townsend C, Rheingold AA (2013). Estimating a child sexual abuse prevalence rate for practitioners: studies. Charleston, S.C., Darkness to Light. Retrieved from
View.
|
|
|
|
|
Ullman SE (2007). Relationship to perpetrator, disclosure, social reactions, and PTSD symptoms in child sexual abuse survivors. Journal of Child Sexual Abuse 16(1):19-36.
Crossref
|
|
|
|
|
Wells R, McCann J, Adams J, Voris J, Dahl B (1997). A validational study of the structured interview of symptoms associated with sexual abuse using three samples of sexually abused, allegedly abused, and nonabused boys. Child abuse & neglect 21:1159-1167.
Crossref
|
|
|
|
|
Whealin J (2007). Child Sexual Abuse. National Center for Post Traumatic Stress Disorder, US Department of Veterans Affairs.
|
|
|
|
|
Young MS, Harford K, Kinder B, Savell JK (2007). The relationship between childhood sexual abuse and adult mental health among undergraduates: Victim gender doesn't matter, Journal of Interpersonal 22:1315-1331.
Crossref
|
|