ABSTRACT
Women’s poor socio-economic status (SES) is linked to multiple contributing factors, most of which are related to performing multiple roles that include family, childcare and reproductive responsibilities in general. However, the relationship between women’s reproductive factors and household SES remains uncertain. This study explored the association between selected reproductive factors and households’ SES among rural households with women of reproductive age. A cross-sectional study, involving six randomly selected villages from three wards of Morogoro district, Tanzania, was used. A total of 542 participants consisting of women from male and female-headed households were involved in the study. Data analyses were performed using the IBM SPSS® software. Ordinal logistic regression model was used to estimate the relationship of the study variables. The number of children a woman wished to have had negative association with SES, whereby wishing to have more than 5 children was associated with less likelihood to attain the higher SES. The mean age at first pregnancy was 18.5 years, with 56.5% of the participants becoming pregnant for the first time at age 18 or below, which indicates predominance of teenage pregnancies. The age at first pregnancy had significant and positive relationship with SES, whereby being pregnant at the age of more than 18 years increases the chance of attaining a higher SES. In conclusion, teenage pregnancies and the desire for relatively many children (>5) constrain the attainment of higher SES. The study recommends strengthening reproductive health education particularly family planning and advocacy on teenage pregnancies in rural communities.
Key words: Women, socio-economic status, reproductive factors, rural, Tanzania.
Socio-economic status (SES) remains one of the areas of interest for researchers in the area of economic development. The phenomenon (SES), is an indicator of well-being of the members of households that is commonly used to depict an economic difference in society as a whole (Abraham, 2016). Since in the 1960s, gender issue has surfaced substantially in analyzing SES in societies particularly when explaining poverty levels (Moser, 2012; Pressman, 2002, 2003; Chant, 2006). The gender concern with regard to socio-economic status is based on the paradigms explaining disproportionate level of poverty among men and women particularly with regard to female-headed households (FHHs) and male-headed households (MHHs). Gender poverty gap is experienced in both developed and under-developed countries. Literature shows that in the world, most of the poor households are those headed by women (Chant, 2012; Cawthorne, 2008). For example, literature shows that by 2008, the gap in poverty rates between men and women was wider in America than anywhere else in the western world (Cawthorne, 2008). In sub-Saharan Africa, Tanzania inclusive, poverty levels take similar trend whereby majority of the poor are households headed by females (Macro, 2011; Kehler, 2013).
For a long time, researchers have made effort to establish the link between gender and SES. The explanation that women and their households consists majority of the poor is widespread (Peterson, 1987; Pressman, 2002, 2003; Chant, 2003, 2006; Cawthorne, 2008; Moser, 2012). One of the prominent theories is the Feminist Explanations for the Feminization of Poverty (Pressman, 2003); the theorist associate women and poor SES with poor participation in the labor market. Gender poverty disparity is apparent, the debate remains on whether the factors that link women and poor SES as reported in the existing literature apply across different socio-economic groups.
Women are linked with poor SES through a variety of factors such as inequality in wages, segregation of employment in paying occupations and domestic sexual-related violence, whereby women are paid less than men even when they have the same qualifications and work same hours (Cawthorne, 2008; Hejase et al., 2013, 2015). The main argument explaining the link between women and poor SES is that women spend more time in performing reproductive roles that usually are not associated with economic gain (Pressman, 2003). Reproductive role is defined as activities related to the creation and sustaining the family and the household (Komatsu et al., 2015; Bibler and Zuckerman, 2013). Women are known to perform multiple roles in societies that are productive role, reproductive role, and the role of community management (Moser, 2012), because of these multiple roles women are constrained in their involvement in productions (Pressman, 2003; Cawthorne, 2008; Moser, 2012).
The link between reproductive roles and household SES is complex, and it involves several factors, most of which have not been studied. The factors vary from one socio-economic group to another across different communities. Studies explaining women factors that lead to poor household SES were conducted mainly in developed countries (Pressman, 2002, 2003; Cawthorne, 2008; Chant, 2012; Moser, 2012) and thus may not be directly extrapolated to under-developed African communities like Tanzania. For example, number of children, which is likely to influence the time that a woman spends for childcare, differs among rural and urban societies even within the same region like Tanzania (Macro, 2011).
Therefore, this study aimed to examine the relationship between women reproductive factors and household SES in Morogoro district, Tanzania. The key reproductive factors in this study included the number of biological children of the study participants, birth interval, and number of unplanned pregnancy(ies) a participant had experienced as well as the age when a participant conceived for the first time. Specifically, the study intended to (i) determine the association between the number of children per woman and household SES, (ii) examine the relationship between the birth interval and household SES, (iii) relate unplanned pregnancies and household SES in the study area, and (iv) analyze the link between the age at first pregnancy and household SES.
Participation of women in socio economic development is inevitable if higher SES is to be attained. This is because they make higher proportion in the productive workforce. In agricultural sectors in Tanzania, women constitute majority (54%) of the work force (Leavens and Anderson, 2011; Palacios-Lopez et al., 2015), meaning that their contribution on economic development is important in order to realize positive change in development not only in their households but also in the whole community. Moreover, the government of Tanzania is committed to transform the economic status of its citizens. This is demonstrated in the development plans formulated that include the frameworks of the first Five Year Development Plan (FYDP I, 2011/2012-2015/2016) and the National Strategy for Growth and Reduction of Poverty (NSGRP/MKUKUTA II, 2010/2011-2014/2015). Findings from this study will provide valuable information concerning the reproductive factors in relation to household SES in rural context, which can be used by development stakeholders to design appropriate interventions for improving living standards of rural residents.
Description of the study area
The study was conducted in Morogoro district because of the prevalence of poverty in the area, where 55% of households (HH) in the district are considered as poor based on headcount ratio (Lusambo, 2016). The district is one of the rural areas where fertility rate is very high. The Total Fertility Rate (TFR) for women 15 to 49years of age in Tanzania was 6.1 in rural areas compared to 3.7 in urban (Macro, 2011). This indicates existence of potential reproductive issues in rural areas. Six villages were involved in this study. The villages were Kinonko and Maseyu from Gwata ward, Madamu and Kibwaya from Mkuyuni ward, as well as Tandai and Ludewa from Kinole ward.
Sampling procedure
The sample size was calculated by considering the standard normal deviation set at 95% confidence level (1.96) and 55% as the estimated prevalence of poverty in the study population (Lusambo,
2016). Using the formula:
where ‘z’ = 1.96 for 95% CI, ‘p’ is expected true proportion (55%) and ‘e’ is the desired precision (0.05), the minimum sample size was estimated to be 381 participants to achieve the desired statistical power (Hejase and Hejase, 2013). However, in order to increase statistical power and precision, 65% of the calculated minimum sample was added to the minimum sample, hence 627 women were included in the study.
The study population was women of reproductive age that is between 15 and 49 years as defined by the Tanzania Demographic and Health Survey report (Macro, 2011). The study participants were those who were residents in the study villages, with at least two children and willing to take part in the study. Majority of the study participants were of the Muslim religion. The units of analysis were both households and individual women. In consultation with local leaders, using available village registers, purposive sampling was used to list down women with the required age from each of the study villages. From the lists, all women who were heads of household were included in the study and those from male-headed households were randomly sampled. All women from female-headed households were included in the study because they are usually fewer (Macro, 2011). Three hundred and twenty-three (59.6%) of the sampled women came from male-headed households while 219 (40.4%) came from female-headed households. After data cleaning, 542 participants were qualified for the analysis. Therefore, the response rate was 86.44%.
Definition of the study variables
Outcome variables
The dependent variable for this study was household SES (wealth index) computed from housing characteristics and asset possession using the Polychoric Principle Component Analysis (PCA). PCA can be defined as a linear combination of optimally weighted observed variables. PCA is used to create a single index variable from a set of correlated variables (Vyas and Kumaranayake, 2006). The main idea of PCA is to reduce the dimensionality of a data set consisting of many variables correlated with each other, either heavily or lightly, while retaining the variation present in the dataset, up to the maximum extent.
Household characteristics that is ownership of the house and material used to build the house and the toilet facility were also used to determine the outcome variable household SES as previously described (Macro, 2011). Another indicator was possession of any of the following assets: motorbike, radio, bicycle, generator, and solar power equipment as recommended by other studies (Filmer and Pritchett, 2001; Sahn and Stifel, 2003; Rutstein and Johnson, 2004; Azzarri et al., 2006). The first component of polychoric PCA was used to generate wealth scores and the scores were then classified using cluster analysis as described in previous studies (Vyas and Kumaranayake, 2006). Cluster analysis attempts to group the most similar cases in one group while maximizing difference between groups. By using this technique, it was possible to create the dependent variable household SES by categorizing wealth scores. The resulting two categories were low and medium-high. The ultimate units of the analysis were individual women.
Data collection methods
Assorted methods were employed in collecting information concerning the study participants and corresponding households. Focus Group Discussions (FGDs) and observations were used to collect primary data. Documentary review was used to collect secondary data. Primary data included demographic information, reproductive factors (number of children, birth interval, unplanned pregnancy and age at first pregnancy), as well as household SES (housing characteristics, toilet facility and assets owned by the household). Secondary data from the national, regional, district and village statistics included poverty distribution in Tanzania, population size per participating village and socio-economic characteristics of the study population.
Explanatory variables and their definitions
The explanatory variables were the selected reproductive factors. They included number of biological children of the study participants, birth interval, and number of unplanned pregnancy(ies) a participant had experienced as well as the age when a participant conceived for the first time. For this study, birth interval refers to the interval between the last two consecutive live births (Koenig et al., 1990; Macro, 2011). On the other hand, unplanned or unintended pregnancies are terms used interchangeably which refer to pregnancies that are reported to have been either unwanted (that is, they occurred when no more children were desired) or mistimed (that is, they occurred earlier or later than desired) (Santelli et al., 2003).
Data collection tool
Data on all study participants were obtained using a structured questionnaire through face to face interview. The questionnaire used in this study was developed by the PhD candidate. Validity and reliability of the questionnaire were determined. It was first piloted on ten respondents before the actual study and these respondents were excluded during actual data collection and analysis. After the pre-test, necessary adjustments in phrasing were made. While the questionnaire was used to collect quantitative data, a separate checklist was used to collect qualitative data through FGDs. The questionnaire was organized into four sections to enable capturing of information about demographic, household and reproductive factors as well as household SES. The checklist was designed to capture information about issues that either needed supplementary explanation, or was not known to normal respondents. Such issues include reasons for low level of education among women, instability of marriages, teenage pregnancy and occurrence of unplanned pregnancies among women in the study area.
Statistical analysis
Quantitative data
After data entry, data cleaning was done. Data were compiled and analyzed using the Statistical Product and Service Solutions, SPSS (Armonk, NY: IBM Corp) version 23.0, an IBM software acquired since 2009 (Hejase and Hejase, 2013). Quantitative analysis involves computations of measures of central tendency (means and/or medians with SD and IQR), frequencies and percentages. Ordinal logistic regression models were applied to test associations and the effect of each explanatory (independent) variable on the outcome variable Odds ratio (ORs) with 95% Confidence Interval (95% CI) for reproductive factors associated with household SES were estimated. A p-value’ of <0.05 was considered to be the cut-off for statistical significance.
Qualitative data
Analyzing qualitative data involved the use of content analysis as recommended by Krueger et al. (2001). Field notes were reviewed and the information from individual focus groups was summarized. Themes were aligned based on guiding questions to indicate different opinions about research issues. Important points were illustrated by quotes.
Descriptive statistics of household and demographic characteristics of respondents
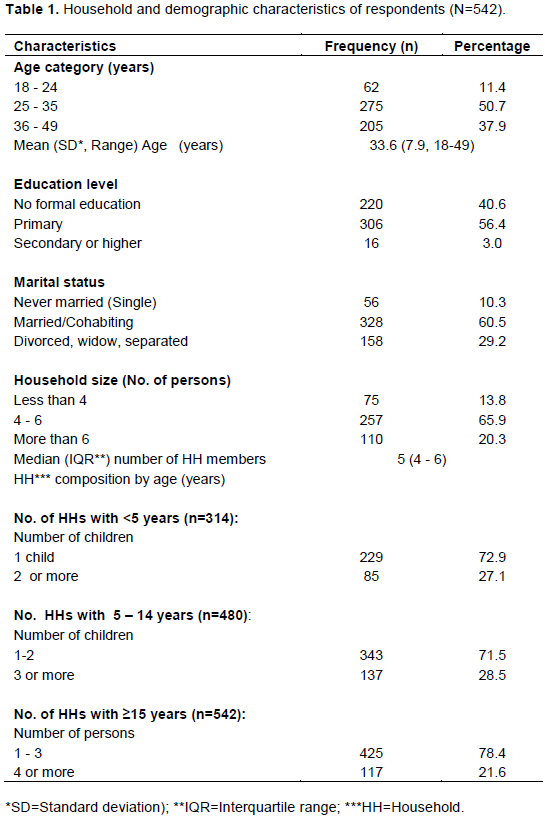
Analysis of data on demographic and household characteristics of the participants was performed. Results for this analysis are shown in Table 1. The age range of participants was between 18 and 49 years, with a mean age of 33.6 (SD= 7.9). About sixty percent (60.5%) of the participants were either married or co-habiting while about a third (29.2%) of participants was widowed, separated, or divorced. The rest of the interviewed women were never married. Sixty-six percent (65.9%) of households involved in the survey consisted of between 4 and 6 persons with the median of 5 persons, whereas one-fifth (20.3%) had more than 6 members. About seventy-three percent (72.9%) consisted of at least one child aged below 5 years; and another big proportion of interviewed women came from households consisting of 1 to 2 children aged 5 to 14 years.
Other characteristics concerning household composition are shown in Table 1.
Descriptive statistics of reproductive factors of study participants
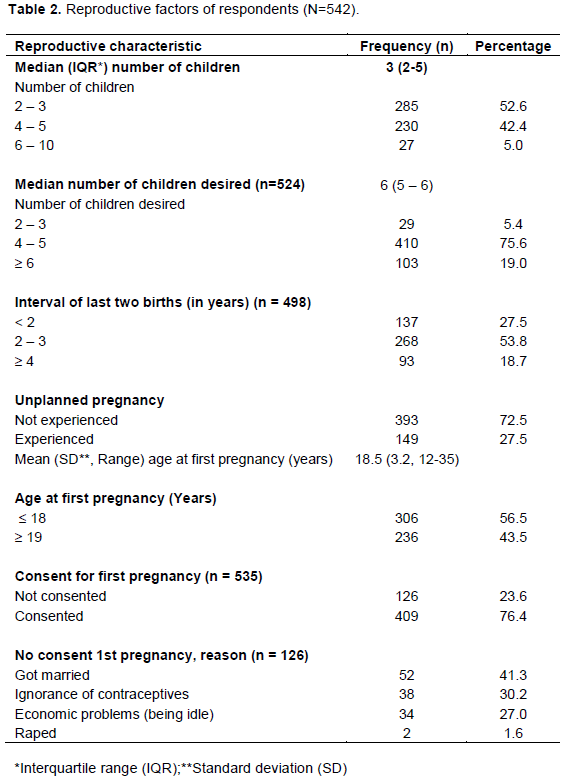
Here, presents reproductive factors of the study participants. Results are shown in Table 2. More than half of the respondents (52.6%) had 2 to 3 children. The median (IQR) number of children per woman participating in the study was 3 (2-5). Nineteen percent of them desired to have more than 6 children while 27.5% of participants had experienced unplanned pregnancies. The mean age at first pregnancy was 18.5 (SD=3.2; Range=12-35), with 56.5 and 43.5% of participants becoming pregnant for the first time at age below 18 and above 19 years, respectively.
FGDs results showed that reasons for conceiving at young age included getting marriage at that age, poverty, family instability resulting to separation of couples as well as culture associated with matrilineal system. About one third (27.5%) of the study women had experienced unplanned pregnancies. The contributing factors for unplanned pregnancies included lack of family planning education particularly for male partners hence not supporting their wives in birth control and poor family planning services in the study area (FGDs). Seventy-six percent (76.40%) of the participants consented for the first pregnancy while the rest of the women did not consent for first pregnancy. Reasons for conception included getting married (41.3%), ignorance of birth-control methods (30.2%), being idle (27.0%) and being raped (1.6%).
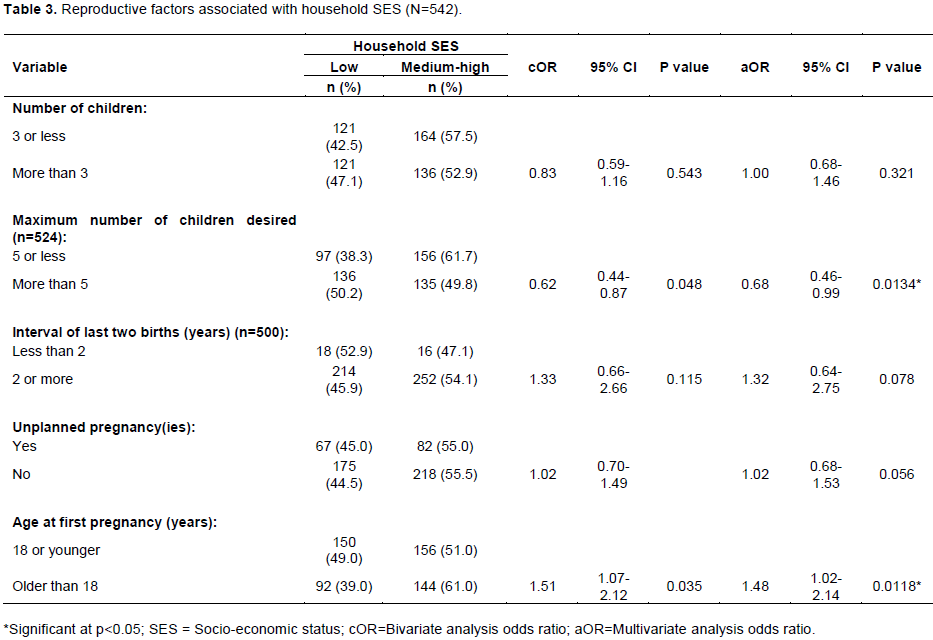
Association between explanatory reproductive factors and household SES
Five explanatory variables that were contemplated to influence the outcome variable (household SES) were subjected to ordinal logistic regression models to analyze the association between the study variables. The explanatory variables were namely: number of children per woman, maximum number of children a woman desired to have, interval of last two births, number of unplanned pregnancies, and the age of a woman at first pregnancy. Out of these variables, three variables did not show significant relationships with the outcome variable (Table 3). Two variables, that is, maximum number of children a woman desired to have and the age at first pregnancy showed significant association with the outcome variable. While the number of children a woman desired to have showed negative relationship with SES, the age of a woman at first pregnancy showed a positive significant association with the outcome variable. Women who wished to have more than 5 children were significantly less likely to be in the higher (medium-high) SES category compared to those who wished to have fewer children (≤5 children) [OR 0.68; 95% CI: (0.46-0.99), p<0.05].
Women who conceived while older than 18 years of age, were almost fifty percent (48%) more likely to be in the higher (medium-high) SES category compared to those conceiving for the first time while they were 18 years or younger [OR 1.48; 95% CI: (1.02-2.14), p<0.05]. A birth interval of 2 or more years between the last two births showed a weak association with SES. Women who spaced their children for 2 years or more showed 32% more likely to attain medium-high SES compared to their counterparts who spaced their last two births for less than 2 years apart. However, this relationship was not statistically significant neither in bivariate or multivariate logistic regression analysis.
The mean age of respondents was 33.6 years, ranging from 18 to 49 years, with the age category of between 25 and 35 years forming the majority of participants. This implies that most of the women who participated in the survey bear children within this age range. In this study, 40.6% of women had not attained formal education. This proportion shows a considerable rate of illiteracy among women in the study area. The observed illiteracy rate was high compared to the average national illiteracy rate of 22 and 18% in 2010 and in 2012, respectively (Macro, 2011). The level of education has been reported as an important factor with impact on reproductive and SES issues. Education empowers women by increasing their autonomy and understanding of family planning issues, which often results into bearing fewer children (Levine et al., 2001). Concerning the number of children per woman, our findings show that majority of women had 2 to 5 children, though 19% of them desired to have more than 6 children. The desired number of children for each woman is in line with findings from the Tanzania Demographic and Health Survey 2012 (URT, 2016), which reported a Total Fertility Rate (TFR) in rural Tanzanian women aged 15 to 49 years to be 6.1 compared to 3.7 in urban areas (Macro, 2016).
In this study and consistent with the Tanzania Demographic and Health Survey data (Macro, 2016), the number of children a woman desired to have, a likely predictor of family size, was negatively associated with SES. Congruent to our finding, a study that involved American women revealed a negative association between a woman’s own income and her number of children, regardless of education (Huber et al., 2010). Previous studies in the Republic of Korea indicated that individuals with the highest education level and better incomes had significantly fewer children compared with the group with the lowest education. Significantly, the non-manual labor group was found to have fewer children compared with those working as homemakers (Kim and Sung, 2013).
This negative relationship has previously been proposed to operate through a diverse set of ways including early pregnancy hence early parenthood and close spacing of children, which compromises economic productivity (Peterson, 1987; Budig and England, 2001; Cawthorne, 2008). According to Kamuzora and Mkanta (2000), the mainstream approach to effects of family size on wellbeing is based on a neo-malthusian ceteris paribus assumption of negative effects of high fertility which collaborates with the argument of savings for investment derived from lower proportions of children, following reduction of fertility. A study in Morogoro region of Tanzania show that large-sized households tended to be income-poor, despite the lack linearity consistence (Mutabazi et al., 2015).
Findings from this study therefore underscore the importance of family planning education among women that will enable them to effectively plan for appropriate number and spacing of their children. The World Health Organization recommends the spacing between consecutive children to be at least 2 years (World Health Organization, 2005). Appropriate planning of the number and spacing of children will enhance economic and development plans, including planning for costs of child education.
More than a half of study participants had their first conception below the age of 18 years, reflecting the predominance of early (teenage) pregnancies and motherhood in the study area. The age at first pregnancy showed a significant positive association with household SES. Participants who had their first pregnancy at or above 18 years were more likely to be in the higher (medium-high) household SES category. Teenage pregnancies and motherhood have been reported to be interlocked with poverty through discontinued education, reduced employment opportunities, un-stable marriages, low incomes and heightened health and developmental risks (Rindfuss et al., 1984).
Findings from this study therefore explain the high degree of vulnerability of the study community, especially women, to poverty through childhood pregnancies and motherhood as previously suggested elsewhere (Varga, 2003; Jaiyeoba, 2009; Hofferth et al., 2001). FGDs attributed teenage pregnancies to early marriages as well as poverty and family instability that forces girls to take responsibility of caring families. Cultural believes associated with matrilineal societies, to which the study community belongs, societies, to which the study community belongs, was reported to encourage early pregnancies by believing that getting children for a girl was important in ensuring perpetuation of the clan.
Through FGDs, participants explained their experience of schoolgirls becoming pregnant and fail to complete secondary education. As expressed by participants during FGDs, community members had the opinion that the education system in the country is likely contributing to the early pregnancies. A woman in Kibwaya village made the following remark; ‘…Lack of accommodation (hostels) in secondary schools forces students to stay in private residential apartments with no proper care, which tend to subject the girls to risks of engaging in unsafe sex, with consequences of unplanned pregnancies...’.
The findings underscore the need to conduct studies to establish empirical evidence on incidence of pregnancies in schools in the study area to suggest entry points for intervention considering that only 3% of participants showed to have attained post-primary school education. Participants expressed their views that the teaching on reproductive health in schools makes youths to ignore traditional training about reproductive matters, while it drives the youth to engage in sexual activities without knowing the consequences.
A woman from Maseyu village had this comment to make ‘... “Current education system exposes girls to sexuality prematurely and thus accelerates their involvement in sexual activities. While the school syllabus for reproductive health is incomplete, it makes girls lose interest of what their parents teach them..”. The study findings from the current study were in line with the report of the WHO (McIntyre and World Health Organization, 2006), that a quarter of all women in Tanzania begin childbearing as adolescents before reaching the age of 20 years (Ngallaba et al., 1993).
A handful of un-consented pregnancies among participating women were observed. The most common reasons were ‘getting married’, ‘ignorance on contraception’ and ‘being idle’. All of the mentioned reasons are linked to family poverty. Poor households tend to force their teenage children into marriages as a means of economic gain (Varga, 2003). Ignorance of contraception and being jobless are both results of failure to access education and secure an income generating activity. Most of the study women had their last two births spaced at most 36 months apart. This birth interval is in accordance with the WHO recommendation of 2 to 3 years (World Health Organization, 2005). The health benefits of longer birth intervals of at least 2 years apart have been reported by several studies (Morley, 1977; Setty-Venugopal and Upadhyay, 2002; Marston, 2006; Macro, 2011).
CONCLUSIONS AND RECOMMENDATIONS
This study has found that the number of children has negative relationship with household SES such that women who wished to have relatively many children, more than five, were less likely to belong to higher (Medium - High) SES. The desire for many children (>5) constrain the attainment of higher SES. Women who conceived while older than 18 years of age, were more likely to attain higher SES compared to those who conceived while they were younger; but majority of women in the study area conceived for at the age of 18 years or younger. Early pregnancy and motherhood restrict the households from attaining higher SES. Factors promoting early pregnancies and motherhood are many with different nature including but not limited to economic and cultural factors. Based on the conclusions, the government through the Ministry of Health is urged to promote reproductive health education in Morogoro district. Early pregnancies and motherhood should be strongly discouraged as part of reproductive health interventions specially tailored to suit low literacy group so that the intended messages are delivered effectively.
The results of this study are subject to the limitation that respondents may not have reported honestly about their reproductive information, income, desire for children or other sensitive topics. Several methods were used to minimize such potential biases including the use of native Swahili language to increase the rapport with respondents and to minimize language barriers. Although respondents were not asked to provide their names or other personal identifiers to observe privacy, a possibility exists that some respondents may have intentionally altered their responses in order to impress the interviewers.
The authors have not declared any conflict of interests.
The authors thank the community leaders of Morogoro District, the District Executive Officer, the ward and village leaders for their cooperation during data collection process. Also, critical revisions of this paper by Professor Jaffu Chilongola along with the financial and logistic support from the Stefano Moshi Memorial University College during the study are highly appreciated.
REFERENCES
|
Abraham EM (2016). Determinants of household socio-economic status in an urban setting in Ghana. Ghana Journal of Development Studies 13:97-114.
Crossref
|
|
|
|
Azzarri C, Carletto G, Davis B, Zezza A (2006). Monitoring poverty without consumption data: an application using the Albania panel survey. Eastern European Economics 44(1):59-82.
Crossref
|
|
|
|
|
Bibler S, Zuckerman E (2013). The care connection: The World Bank and women's unpaid care work in select sub-Saharan African countries. WIDER Working Paper.
|
|
|
|
|
Budig MJ, England P (2001). The wage penalty for motherhood. American Sociological Review 66(2):204-225.
Crossref
|
|
|
|
|
Cawthorne A (2008). The straight facts on women in poverty. Center for American Progress 8:1-3.
|
|
|
|
|
Chant S (2003). Female household headship and the feminisation of poverty: Facts, fictions and forward strategies.
View site visited on 15/2/2019.
|
|
|
|
|
Chant S (2006). Re-thinking the 'feminization of poverty in relation to aggregate gender indices. Journal of Human Development 7:201-220.
Crossref
|
|
|
|
|
Chant S (2012). The disappearing of 'Smart economics'? The World Development Report 2012 on Gender Equality: Some concerns about the preparatory process and the prospects for paradigm change. Global Social Policy 12:198-218.
Crossref
|
|
|
|
|
Filmer D, Pritchett LH (2001). Estimating wealth effects without expenditure data GÇöor tears: An application to educational enrollments in states of India. Demography 38:115-132.
Crossref
|
|
|
|
|
Hejase AJ, Hejase HJ (2013). Research Methods A Practical Approach for Business Students. (2nd edition). Philadelphia, PA, USA: Masadir Incorporated.
|
|
|
|
|
Hejase AJ, Hejase HJ, Hejase AH (2015). Gender Wage Gap in Lebanon: Explorative Analysis. Journal of Applied Economics and Business Research JAEBR 5(1):1-19.
|
|
|
|
|
Hejase H, Haddad Z, Hamdar B, Massoud R, Farha G (2013). Female leadership: An exploratory research from Lebanon. American Journal of Scientific Research 86:28-52.
|
|
|
|
|
Hofferth SL, Reid L, Mott FL (2001). The effects of early childbearing on schooling over time. Family Planning Perspectives, pp.259-267.
Crossref
|
|
|
|
|
Huber S, Bookstein FL, Fieder M (2010). Socioeconomic status, education, and reproduction in modern women: An evolutionary perspective. American Journal of Human Biology 22(5):578-587.
Crossref
|
|
|
|
|
Jaiyeoba AO (2009). Perceived impact of universal basic education on national development in Nigeria. International Journal of African and African-American Studies 6:113-120.
|
|
|
|
|
Kamuzora CL, Mkanta W (2000). Poverty and household/family size in Tanzania: Multiple responses to population pressure?.
|
|
|
|
|
Kehler J (2013). Women and poverty: the South African experience. Journal of International Women's Studies 3:41-53.
|
|
|
|
|
Kim J, Sung J (2013). Socioeconomic status and number of children among Korean women: the healthy twin study. Journal of Preventive Medicine and Public Health 46(1):50.
Crossref
|
|
|
|
|
Koenig MA, Phillips JF, Campbell OM, D'Souza S (1990). Birth intervals and childhood mortality in rural Bangladesh. Demography 27:251-265.
Crossref
|
|
|
|
|
Komatsu H, Malapit HJ, Theis S (2015). How does women's time in reproductive work and agriculture affect maternal and child nutrition? Evidence from Bangladesh, Cambodia, Ghana, Mozambique, and Nepal. (No. 1486). International Food Policy Research Institute (IFPRI).
Crossref
|
|
|
|
|
Krueger RA, Casey MA, Donner J, Kirsch S, Maack JN (2001). Social analysis: Selected tools and techniques. Social Development Paper 36p.
|
|
|
|
|
Leavens MK, Anderson CL (2011). Gender and Agriculture in Tanzania EPAR Brief. Seattle, USA: Evans School Policy Analysis and Research, University of Washington. Volume 134.
|
|
|
|
|
Levine JA, Pollack H, Comfort ME (2001). Academic and behavioral outcomes among the children of young mothers. Journal of Marriage and Family 63:355-369.
Crossref
|
|
|
|
|
Lusambo LP (2016). Households' income poverty and inequalities in Tanzania: Analysis of empirical evidence of methodological challenges'. Journal of Ecosystem and Ecography 6(2):183.
Crossref
|
|
|
|
|
Macro ICF (2011). Tanzania demographic and health survey 2010. National Bureau of Statistics, Dar es Salaam, Tanzania; Calverton, Maryland, USA.
|
|
|
|
|
Macro ICF (2016). Tanzania Demographic and Health Survey 2016. Dar es Salaam, Tanzania: National Bureau of Statistics.
|
|
|
|
|
Marston C (2006). Report of a WHO Technical Consultation on Birth Spacing Geneva Switzerland pp. 13-15.
|
|
|
|
|
McIntyre P, World Health Organization (2006). Pregnant adolescents: delivering on global promises of hope. WHO Press, World Health Organization, Geneva.
|
|
|
|
|
Morley D (1977). Biosocial advantages of an adequate birth interval. Journal of Biosocial Science 9:69-81.
Crossref
|
|
|
|
|
Moser CO (2012). Gender planning and development: Theory, practice and training Routledge Publishers. Washington, DC. 298p.
Crossref
|
|
|
|
|
Mutabazi KD, Sieber S, Maeda C, Tscherning K (2015). Assessing the determinants of poverty and vulnerability of smallholder farmers in a changing climate: The case of Morogoro region, Tanzania. Regional Environmental Change 15(7):1243-1258.
Crossref
|
|
|
|
|
Ngallaba S, Kapiga SH, Ruyobya I, Boerma JT (1993).Tanzania Demographic and Health Survey 1991/1992.
|
|
|
|
|
Palacios-Lopez A, Christiaensen L, Kilic T (2015). How much of the labor in African agriculture is provided by women? The World Bank.
Crossref
|
|
|
|
|
Peterson J (1987). The feminization of poverty. Journal of Economic 21:329-337.
Crossref
|
|
|
|
|
Pressman S (2002). Explaining the gender poverty gap in developed and transitional economies. Journal of Economics 36:17-40.
Crossref
|
|
|
|
|
Pressman S (2003). Feminist explanations for the feminization of poverty. Journal of Economics 37:353-361.
Crossref
|
|
|
|
|
Rindfuss RR, John C, Bumpass LL (1984). Education and the timing of motherhood: Disentangling causation. Journal of Marriage and Family 46(4):981-984.
Crossref
|
|
|
|
|
Rutstein SO, Johnson K (2004). The DHS wealth index. DHS comparative reports No. 6. Calverton: ORC Macro.
|
|
|
|
|
Sahn DE, Stifel DC (2003). Urban-rural inequality in living standards in Africa. Journal of African Economies 12:564-597.
Crossref
|
|
|
|
|
Santelli J, Rochat R, Hatfield É, Timajchy K, Gilbert BC, Curtis K, Cabral R, Hirsch JS, Schieve L (2003). The measurement and meaning of unintended pregnancy. Perspectives on Sexual and Reproductive Health 35:94-101.
Crossref
|
|
|
|
|
Setty-Venugopal V, Upadhyay UD (2002). Birth spacing: three to five saves lives. Population Reports. Series L: Issues in World Health 13:1-23.
|
|
|
|
|
URT (2016). Household Budget Survey 2017-18: Key indicators Report. Dodoma, Tanzania: National Bureau of Statistics and Ministry of Finance and Planning.
|
|
|
|
|
Varga CA (2003). How gender roles influence sexual and reproductive health among South African adolescents. Studies in Family Planning 34:160-172.
Crossref
|
|
|
|
|
Vyas S, Kumaranayake L.(2006). Constructing socio-economic status indices: how to use principal components analysis. Health Policy and Planning.
Crossref
|
|
|
|
|
World Health Organization (2005). Addressing violence against women and achieving the Millennium Development Goals. WHO Press. Geneva.111:
|
|