Full Length Research Paper

ABSTRACT
Diabetes mellitus (DM) is one of the most chronic and dangerous diseases worldwide and in the Saudi society in particular. Swabs (168) from DM injuries were collected from inpatient and outpatient departments. Analysis of variance revealed the high incidence of diabetic foot infections compared to other injuries by an average of 51 and 33, respectively. Adults’ category was significantly the highest age category in the incidence. Inpatients have recorded the highest incidence than outpatients, while routine cases have recorded the highest rates of infection compared to the urgent and very urgent cases. Etiology was confined in 210 bacterial isolates belonging to gram negative (G-ve), gram-positive (G+ve), aerobic and anaerobic bacteria. The study detected a high incidence in one genus/swab compared to two, three, four genera and polymicrobial/swab, with 67, 14, 1, 0.5 and 1.5% respectively. Aerobic bacteria reached 98.5% compared to anaerobic bacteria (1.5%). G-ve aerobic bacteria were highly significant compared to the G+ve. The dominant bacterial species in diabetic injuries was Pseudomonas aeruginosa followed by Staphylococcus aureus with a rate of 28 and 17%, respectively. It is worth noting that the antibacterial ability was evident in Ps. aeruginosa for the most bacterial isolates tested, and this reinforces the result found in the study of Ps. aeruginosa’s dominance in diabetes compared to the rest of the isolated bacterial genera. Results of the study are considered unique in the epidemic spread of diabetic injuries for inpatients, outpatients, as well as the antagonistic relations of each bacterial etiology of diabetic injuries in Saudi Arabia.
Key words: Epidemiology, etiology, bacteria, diabetic injuries, age, in-outpatients, priority, polymicrobial, aerobic, anaerobic, Ps. aeruginosa, S. aureus.
INTRODUCTION
Diabetes mellitus (DM) is a chronic disease that is widespread in the world. In Saudi society, in particular, the rate of diabetes in 1985 was estimated to be 5%, which reached 13% in 2000. Recent data from Saudi Arabia shows that the prevalence of type-2 DM reached 25.4% in 2014 (Al-Rubeaan et al., 2015). Moreover, there were 3.4 million cases of diabetes in 2015 (IDF, 2015), which means it is a continuous increase in Saudi Arabia, due to the lifestyle leading to higher incidence of DM (Al-Sobayel et al., 2014). Many studies have been conducted on the Saudi populations with risk factors for complications from diabetic foot (Al-Wakeel et al., 2009; Hu et al., 2014; Zahrani et al., 2014). Diabetic foot injuries are the most frequent (Currie et al., 2009), and lead to more severe complications for diabetic patients, by progressing to foot ulcers at some time in their lives (Singh et al., 2005). Moreover, diabetic injuries exposed to bacterial infection (Espinosa et al., 1999) mainly, compared to injured persons who are not diabetics (Reiber, 2001) lead to inflammation and destruction of the tissue, and can lead to amputation of the lower limbs.
The current research aims to study bacterial infections of diabetic injuries in a group of Saudi Arabia patients, represented in the Riyadh region by assessing the relationship between these injuries and the status of the patients from various aspects. The study also includes isolation and identification of bacteria associated with diabetic injuries in general, in addition to the production of “Bacteriocin” from bacterial species isolated from diabetic ulcers, for studying the dominance of these bacterial species in diabetic injuries.
MATERIALS AND METHODS
Swabs were collected from 168 injuries who are suffering from diabetes mellitus in Riyadh Medical Complex, Ministry of Health, Central Region - Riyadh, Saudi Arabia, from September 5th, 2005 to January 30th, 2006.
Recommended methods in Medical Complex were followed such as sterilizing the place of taking the sample by using 70% of ethylic alcohol or iodine or quaternary ammonium compounds or chlorine hexedine. Swabs were cultured immediately at their arrival to Central bacteriological Laboratory on the following media: Blood agar, chocolate agar, MacConky in CO2; the plates were incubated overnight at 37ËšC in O2 incubator. Pure colonies were checked in morphology, microscopic examination (gram stain, spores, and motility). Also, biochemical tests based on API-Staph system and API-tests 20E and API-20Strep (GHL, 2013) were used to identify the bacterial species. Furthermore, some differentiating tests were used such as: Catalase, Optochin Disk, Staphrex, Bile Aesculin hydrolysis, and Oxidase test by the methods used by Holt et al. (2000), and Murray et al. (2003).
It is worth mentioning, that wound swabs include the following data: Sex, age, place of isolation, hospital departments and bacterial isolates from injuries and on this basis we examined the different relationships associated with the epidemiological spread of the disease in the central region, Riyadh, Saudi Arabia.
Genera and species have been tested for their antagonistic effect depending on the method of Shoeib (1995). The antagonistic effect of the isolated bacterial species from the diabetics’ injuries was measured as the inhibition area resulting from growth.
Data were analyzed by SPSS (2006) Program: frequencies and percentages, the means and standard deviations, the analysis of variance and Duncan test.
RESULTS
The relationship between diabetic injuries and the general state of the patients
Gender and DM foot infection
Regarding the gender difference in the study, the results showed that the number of the males suffering from diabetic injuries was more than the females; where the number of males was 137 out of 168; while the number of females was 31 out of 168, at a rate of 4.4:1 respectively.
Patients’ reports also pointed the high incidence of diabetic foot injuries compared to the injuries in other areas of the body, where the incidence of diabetic foot reached 102 out of 168 representing 60.7%; while other injuries reached 66, representing 39.2% (Table 1).

Amputations cases reached 13 cases out of 168 representing 7.14%; 10 cases of them were males, and 3 were females; 10 cases were below the knee amputation and 3 cases of toe amputation.
Analysis of variance refers to the existence of significant difference P<0.01 where the incidence of diabetic foot was significantly more than other injuries by an average ratio of 51 and 33 respectively. The number of males was significantly P<0.0001 outperforming the number of females with an average ratio of 68.5 and 15.5, respectively (Table 1).
Age categories
Statistical analysis of the data showed that the proportion of males with diabetic injuries was significantly higher (P <0.01) than the proportion of females (27.4% and 6.2% respectively). There was also a significant effect (P <0.001) for age categories (Table 2), where the adult category was higher- according to the incidence (%55.5). Moreover, then came the four categories (adolescent, children, elderly, suckling) with an equal average statistically proportions (14.5, 7, 5.5 and 1.5%, respectively).
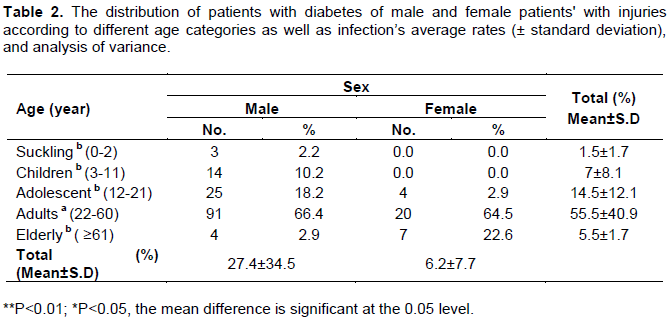
Considering the results of the analysis of variance, it was found that the number of infected males was significantly higher (P<0.05) than the number of females with an average of 27.6 and 6% respectively.
It was noted that the number of infected males was higher than the number of infected females in all age categories except the elderly category in which the number of females outranked the number of males at the rate of 1.75:1.
Inpatients and outpatients
According to the obtained results, it was found that there was a significant difference (P<0.05) in the incidence of diabetic injuries between inpatients (83.5%) and outpatients (0.5%) (Table 3). The number of male inpatients was 136 out of 167, and it was higher than the number of female inpatients (31 out of 167).

Priority
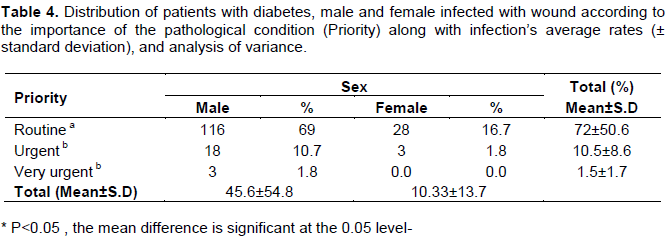
Patients’ cases were divided in terms of their importance into three categories of cases: Routine, urgent, and very urgent. Analysis of variance (Table 4) has shown that there is a significant difference (P<0.01) in the proportion of the importance of the condition of patients with diabetes in Riyadh Medical Complex. The routine cases were significantly higher (72%) followed by the other two types (Urgent and Very Urgent) in static equal proportions (10.5 and 1.5%, respectively) where there is no significant difference between these two categories. It has been observed that the number of infected males was significantly higher (P<0.05) than the number of infected females (45.6 and 10.3%, respectively).
The relationship between diabetic injuries and bacterial etiology
Multiple bacterial species for each swab
Statistical analysis has shown that the incidence of one genus of aerobic bacteria/swab was highly significant (67%). Then came the incidence of two, three, four aerobic bacterial species and polymicrobial (Mixed from aerobic and anaerobic bacteria)/swab, with an equal average of proportions statistically (14, 1, 0.5 and 1.5%, respectively) (Table 5).

Aerobic and anaerobic bacteria
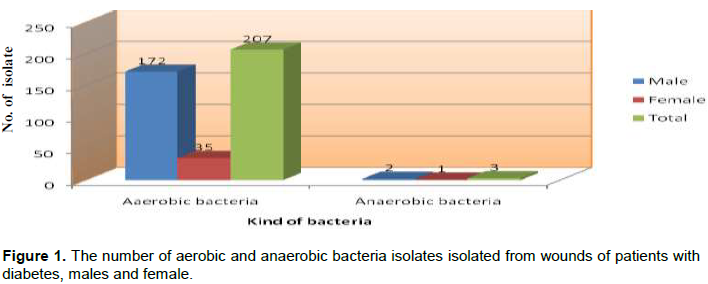
All tested 168 swabs contained aerobic bacteria, where the number of aerobic isolates was 207 out of 210 represented by 98.5%; while the number of anaerobic isolates reached 3 represented by 1.5%. It is worth mentioning that anaerobic bacteria are isolated independently, but are associated with aerobic bacteria as well (Figure 1).
Aerobic G-ve and G+ve bacteria
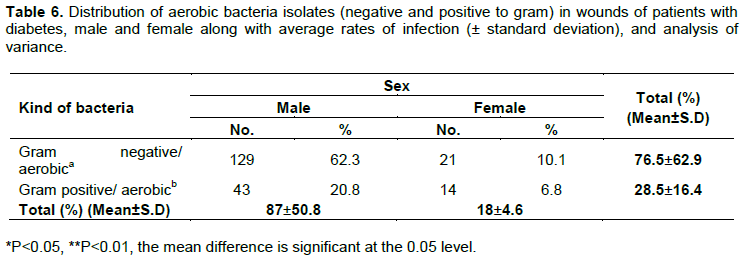
Analysis of variance indicates a significant difference (P<0.05) between the incidence of aerobic G-ve bacteria (76.5%) and the incidence of aerobic G+ve bacteria (28.5%). Analysis of variance also refers to the high incidence for males than females significantly, and is also P<0.01, with an average represented by 87% compared to 18% for male and females respectively (Table 6).
The dominance of bacterial species
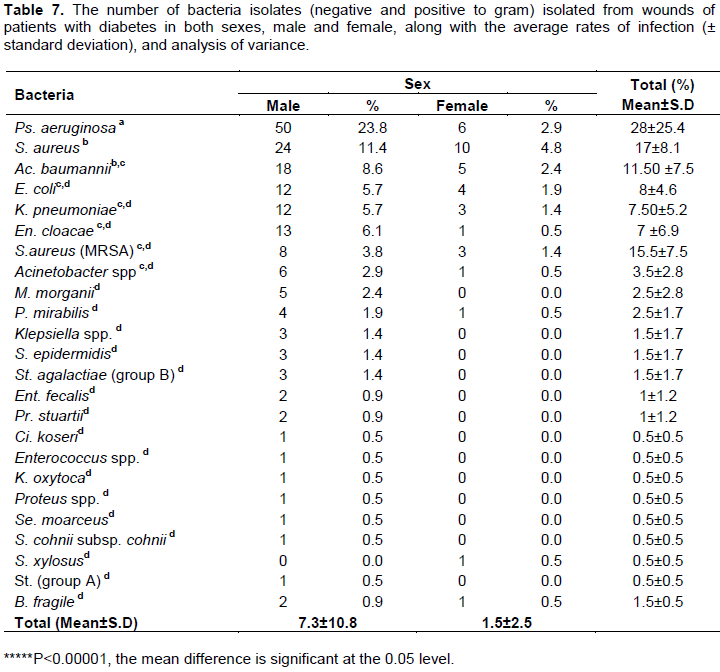
According to the standard tests recommended, G-ve and G+ve bacteria genera and species had been identified (Table 7); also the fungus Candida tropicalis of the yeasts was isolated. Throughout the study, it was found that the bacterial species mostly associated with injuries was the rod bacterium of Ps. aeruginosa (G-ve); it amounted to 56 out of 210 isolates with an average of 26.7%, followed by spherical bacteria of S. aureus (G+ve), comprising 34 isolates out of 210 with an average of 16.2% (Table 7).
Diabetic injuries and its associated genera with Ps. aeruginosa
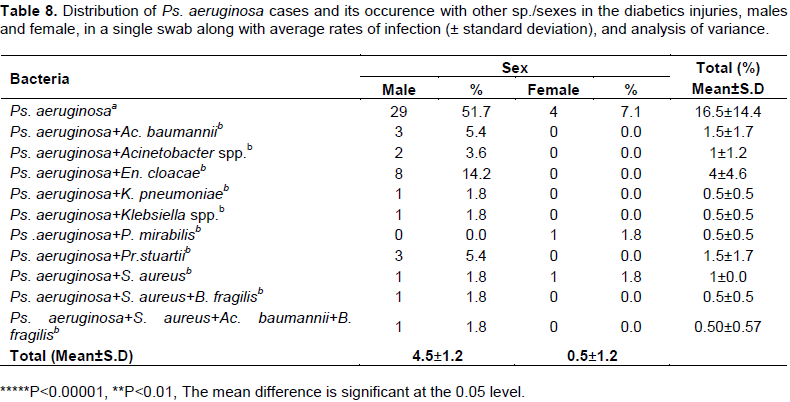
Due to the dominance of Ps. aeruginosa in diabetic injuries, species associated with it have been studied (Table 8). Analysis of variance showed significant difference (P<0.00001) of the presence of Ps. Aeruginosa by repeating 33 cases out of 56 cases in this bacterium alone (58.8%). Ps. aeruginosa was associated with En. cloacae, where the number of cases was 8 cases representing 14.2%. This bacterium was accompanied by other bacterial species (K. pneumonia, Klebsiella spp, P. mirabilis, S. aureus + Bacteroides fragilis, S. aureus + Ac. baumannii + B. fragilis) separately in one case at a rate of 1.8% and in equal proportions that were statistically significant. The high incidence in males than female significantly (P<0.00001) [average incidence in males (4.5) compared to 0.5 in females] was recorded (Table 8).
Diabetic injuries and its associated genera with S. aureus
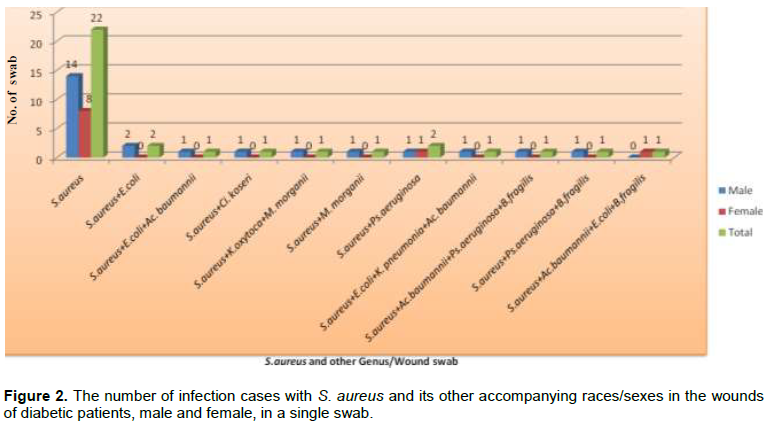
S. aureus (G+ve) was the second genus that recorded the highest rates of bacterial diabetic injuries significantly (Table 7), where it was isolated solely by repeating 22 cases out of 34 cases, with a percentage of 65.1%. Moreover, while it was associated with other species it ranged between 5.9% and 2.9% (Table 9).
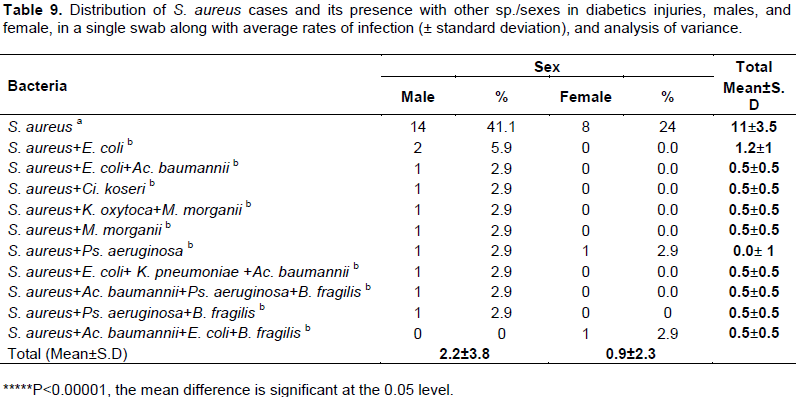
Results of the analysis of variance showed that the percentage of the presence of spherical bacteria (G+ve) of S. aureus solely is significantly higher (P<0.00001) than its presence associated with other bacterial species with an equal average ratio of 11%. While, the other species was associated with an equal average statistic of 1% and 0.5%. There was a higher incidence for males than females (P<0.00001) with an average infection rate of 2.2% and 0.9% respectively (Table 9, Figure 2).
The antagonistic effect and dominance of bacteria isolated from diabetic injuries:
The antagonistic effect of isolated bacteria from diabetic injuries showed inhibition zone of some other isolated bacteria (Table 10) as follows: S. aureus (MRSA) showed antagonistic ability against K. pneumoniae, and the inhibition area was estimated by 5 mm; while K. pneumoniae showed antagonistic ability against S. aureus with an estimated inhibition area of 10 mm. En. cloacae showed antagonistic ability against K. pneumoniae by the emergence of the inhibitory area, and that was estimated by 4 mm. Proteus spp. showed antagonistic ability against Klebsiella spp. that was estimated by 17 mm..
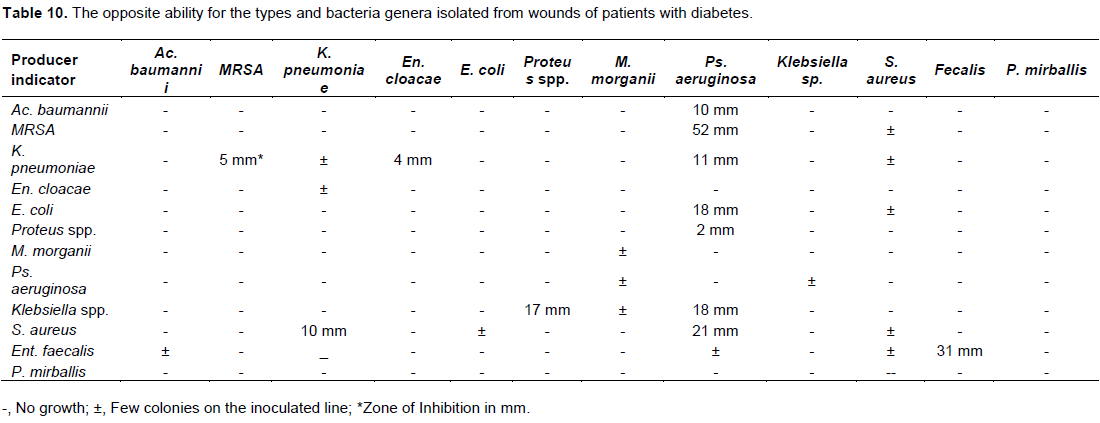
While Ps. aeruginosa showed different antagonistic ability against many tested genera namely: S. aureus, Proteus spp, K. pneumoniae, E. coli, Ac. baumannii, S. aureus (MRSA), Klebsiella spp, while the antagonistic ability of Ent. faecalis was estimated by 31 mm. Moreover, some tested Genera showed antagonistic ability against other isolates represented in the emergence of a limited number of bacterial colonies along the inoculation line (Table 10).
DISCUSSION
The results of the statistical analysis indicated that the highest infection rates of injuries for both males and females were confined in the adult category, while there was no significant difference between the other categories (Abdulrazak et al, 2005; Pemayun and Naibaho, 2017). A high incidence of diabetic foot compared to other injuries was in agreement with the findings of previous studies (Pecoraro et al, 1990; Reiber et al, 1995; Karchmer and Gibbons 1994; Boulton et al, 2006; Gonzalez et al, 2003; Pemayun and Naibaho, 2017).
The current study has shown that the number of inpatients and routine cases for patients scored significantly higher than the number of outpatients and both urgent and very urgent cases. The etiology of bacteria associated with diabetic injuries coincided with previous studies in the dominance of aerobic bacteria over the anaerobic ones (Ako-Nai et al, 2006; Akhi et al, 2015; Haldar et al, 2017) and that the G-ve were the most prevalent ones, followed by the G+ve aerobic bacterial species (Espinosa et al, 1999, Haldar et al, 2017).
Isolation of anaerobic B. fragilis with few repetition agrees with Ward (1982), and they were not isolated autonomously (Louie et al, 1976; Scher and Steel, 1988; Young et al, 1993).
Detection of Polymicrobial/swab in this study agreed with Brook and Frazier, (2000); Mottola et al (2016) and Haldar et al (2017). While, Cunha (2000) said that the most diabetic foot injuries, that are gravity ranging between being moderate to severe were caused by Polymicrobial which requires treatment with wide-ranging antibiotics.
Ps. aeruginosa and S. aureus were the dominant in diabetic injuries; this is in agreement with a study of Abdulrazak et al. (2005), Bansal et al. (2008) and Sánchez-Sánchez et al. (2017) who mentioned that S. aureus was isolated more frequently regarding individual species; however, it disagreed with Proteus mirabilis (Espinosa et al., 1999), E. coli (Ako-Nai et al., 2006) Streptococcus sp. and Enterococcus sp. (Gonzalez et al., 2003).
Antagonistic ability of Ps. aeruginosa for the most tested isolates namely: S. aureus, Proteus spp., K. pneumoniae, MRSA, Klebsiella spp., E. coli, Ac. baumannii were recorded, and what enhances the obtained result during the research is Ps. aeruginosa in diabetic injuries was dominant. Results from Hosono et al (2011) agreed with our findings which indicated that Ps. aeruginosa has antimicrobial activities against G-ve bacteria, including E. coli and K. pneumoniae, as well as P. aeruginosa itself. Moreover, Chacon et al. (1986) indicated that 90% of the isolates Ps. aeruginosa have the ability to produce “Bacteriocin”. Bauernfeind et al. (1981) also showed that K. pneumoniae has the ability to produce antioxidants and the inhibition of some genera. However, this result was explained partially with the current study, which showed that K. pneumoniae isolated from the diabetic injuries has antagonistic ability against S. aureus only. In addition, our results recorded the ability of MRSA, En. cloacae and Proteus sp., separately, to inhibit the growth of K. pneumoniae, while Ent. faecalis has antagonistic ability against itself.
CONCLUSION
The increased number of males with diabetic injuries than females is probably due to the nature of the Saudi society, particularly the different activities of males, which exposes them to more injuries. Previous studies did not address the epidemic spread of diabetic injuries for inpatients, outpatients and priority, as well as the antagonistic relations of each bacterial etiology of diabetic injuries, subsequently dominance of its genus/genera. Therefore, data obtained from this study covered for first time the missing information in epidemic spread of inpatients, outpatients and priority, as well as the antagonistic relations of each bacterial etiology of diabetic injuries in Central Region of Riyadh, Saudi Arabia.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors extend their appreciation to the Deanship of Scientific Research at King Saud University for funding this work.
REFERENCES
|
Abdulrazak A, Bitar ZI, Al-Shamali AA, Mobasher LA (2005). Bacteriological study of diabetic foot infections. Journal of Diabetes Complications 19(3):138-141. |
|
|
Ako-Nai A, Ikem I, Akinloye O, Aboderin A, Ikem R, Kassim O (2006). Characterization of bacterial isolates from diabetic foot infections in Ile-Ife, Southwestern Nigeria. The Foot 16(3):158-164. |
|
|
Akhi MT, Ghotaslou R, Asgharzadeh M, Varshochi M, Pirzadeh T, Memar MY, Bialvaei A, Sofla HSY, Alizadeh N (2015). Bacterial etiology and antibiotic susceptibility pattern of diabetic foot infections in Tabriz, Iran. GMS Hygiene and Infection Control 10:2. |
|
|
Alâ€Rubeaan K, Alâ€Manaa HA, Khoja TA, Ahmad NA, Alâ€Sharqawi AH, Siddiqui K, Alnaqeb D, Aburisheh KH, Youssef AM, Alâ€Batel A, Alotaibi MS (2015). Epidemiology of abnormal glucose metabolism in a country facing its epidemic: SAUDIâ€DM study. Journal of Diabetes 7(5):622-632. |
|
|
Al-Sobayel H, Aleisa E, Buragadda S, Ganeswara RM (2014). Rehabilitation Services in Saudi Arabia: An Overview of its Current Structure and Future Challenges. Journal of General Practice 2(6):1-6. |
|
|
Al-Wakeel JS, Hammad D, Al Suwaida A, Mitwalli AH, Memon NA, Sulimani F (2009). Microvascular and macrovascular complications in diabetic nephropathypatients referred to nephrology clinic. Saudi Journal of Kidney Diseases and Transplantation 20(1):77-85. |
|
|
Al-Zahrani MK, Elnasieh AM, Alenezi FM, Almoushawah AA, Almansour M, Alshahrani F, Rahman SU, Al-Zahrani A (2014). A 3-month oral vitamin D supplementation marginally improves diastolic blood pressure in Saudi patients with type 2 diabetes mellitus. International Journal of Clinical and Experimental Medicine 7(12):5421-5428. |
|
|
Bansal E, Garg A, Bhatia S, Attri AK, Chander J (2008). Spectrum of microbial flora in diabetic foot ulcers. Indian Journal of Pathology and Microbiology 51:204-208. |
|
|
Bauernfeind A, Petermüller C, Schneider R (1981). Bacteriocins as tools in analysis of nosocomial Klebsiella pneumoniae infections. Journal of Clinical Microbiology 14(1):15-19. |
|
|
Brook I, Frazier EH (2000). Aerobic and anaerobic microbiology in intra-abdominal infections associated with diverticulitis. Journal of Medical Microbiology 49(9):827-830. |
|
|
Chacon JD, Sancho CA, Solvas JF, Ruiz GB (1986). Possibility of using purified pyocins for typing Pseudomonas aeruginosa: purification of pyocins and sensitivity of p. aeruginosa in different tests. Annales de l'Institut Pasteur Microbiologie 137(1):253-266. |
|
|
Boulton AJM, Cavanagh PR, Rayman G (2006). The Foot in Diabetes, 4th Edition, Wiley, New York. pp. 363-366. |
|
|
Cunha BA (2000). Antibiotic selection for diabetic foot infections: a review. The Journal of Foot and Ankle Surgery 39(4):253-257. |
|
|
Currie C, Gabhainn SN, Godeau E (2009). The Health Behaviour in School-aged Children: WHO Collaborative Cross-National (HBSC) study: origins, concept, history and development 1982–2008. International Journal of Public Health 54(2):131-139. |
|
|
Espinosa Y, Nieves B, Quintana A (1999). Aerobic and anaerobic bacteria in diabetic foot disease. Anaerobe 5(3-4):405-407. |
|
|
Global Health Laboratories (GHL) (2013). Microbiology Standard Operating Procedure-Bacterial Identification Using BioMerieux API Kits. |
|
|
Gonzalez FJ, Alramadan M, Matesanz M, Diaz A, Gonzalez-Romo F, Candel I, Calle A, Picazo JJ (2003). Infections in Diabetic Foot Ulcers. European Journal of Internal Medicine 14(5):341-343. |
|
|
Haldar J, Mukherjee P, Mukhopadhyay S, Maiti PK (2017). Isolation of bacteria from diabetic foot ulcers with special reference to anaerobe isolation by simple two-step combustion technique in candle jar. The Indian Journal of Medical Research 145(1):97-101. |
|
|
Holt JG, Krieg NR, Sneath PH, Staley JT, Williams ST (2000). Bergey's Manual of Determinative Bacteriology 9th ed. Lippincott Williams and Wilkins, A wolters Kluwer Company Philadelphia, Baltimore, New York, London pp. 527-545. |
|
|
Hosono Honda N, Kimura S, Tateda K, Horikawa M, Ueda C, Ishii Y, Ishiguro M, Miyairi S, Yamaguchi K (2011). Roles of Pseudomonas aeruginosa autoinducers and their degradation products, tetramic acids, in bacterial survival and behavior in ecological niches. Microbes and Environments 26(2):160-164. |
|
|
Hu Y, Bakhotmah BA, Alzahrani OH, Wang D, Hu FB, Alzahrani HA (2014). Predictors of diabetes foot complications among patients with diabetes in Saudi Arabia. Diabetes Research and Clinical Practice 106(2):286-294. |
|
|
International Diabetes Federation (IDF) (2015). International Diabetes Federation, Middle East and North Africa. |
|
|
Karchmer AW, Gibbons GW (1994). Foot infections in diabetes: evaluation and management. Current Clinical Topical Infections Disease 14:1-22. |
|
|
Louie TJ, Bartlett JG, Tally FP, Gorbach SI (1976). Aerobic and anaerobic bacteria in diabetic foot ulcers. Annals of Internal Medicine 85(4):461-463. |
|
|
Mottola C, Mendes JJ, Cristino JM, Cavaco-Silva P, Tavares L, Oliveira M (2016). Polymicrobial biofilms by diabetic foot clinical isolates. Folia Microbiologica 61(1):35-43. |
|
|
Murray PR, Baron EJ, Jorgensen JJ, Pfaller MA, Yolken RH (2007). Manual of Clinical Microbiology, 9th ed. ASM Press: Washington, DC. |
|
|
Pecoraro GE, Reiber GE, Burgess EM (1990). Pathways to diabetic limb amputation: basis for Prevention. Diabetes Care 13(5):513-521. |
|
|
Pemayun TGD, Naibaho RM (2017). Clinical profile and outcome of diabetic foot ulcer, a view from tertiary care hospital in Semarang, Indonesia. Diabetic Foot and Ankle 8(1):1-8. |
|
|
Reiber GE, Boyko EJ, Smith DG (1995). Lower extremity foot ulcers and amputations in diabetes. Diabetes in America pp. 409-427. |
|
|
Reiber GE (2001). Epidemiology of foot ulcers and amputations in the diabetic foot. In: Levin ME, Bowker JH, Pfeifer MA (eds.), Levin and O'Neal's the diabetic foot, Elsevier Health Sciences pp. 13-32. |
|
|
Sánchez-Sánchez M, Cruz-Pulido WL, Bladinieres-Cámara E, Alcalá-Durán R, Rivera-Sánchez G, Bocanegra-García V (2017). Bacterial Prevalence and Antibiotic Resistance in Clinical Isolates of Diabetic Foot Ulcers in the Northeast of Tamaulipas, Mexico. The International Journal of Lower Extremity Wounds 16(2):129-134. |
|
|
Scher KS, Steele FJ (1988). The septic foot in patients with diabetes. Surgery 104(4):661-666. |
|
|
Shoeib AA (1996). Bacteriocin production by Erwinia amylovora strains. In VII International Workshop on Fire Blight 411:229-236. |
|
|
Singh N, Armstrong DG, Lipsky BA (2005). Preventing foot ulcers in patients with diabetes. JAMA 293(2):217-228. |
|
|
Statistical Package for Social Science (SPSS) (2006). Guide to data analysis, by Norus MJ. SPSS Inc, Publisher: Upper Saddle River, N. J., Prentice Hall 2006. |
|
|
Ward JD (1982). The diabetic leg. Diabetologia 22(3):141-147. |
|
|
Young MJ, Veves A, Boulton AJ (1993). The diabetic foot: aetiopathogenesis and management. Diabetes/Metabolism Research and Reviews 9(2):109-127. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


