ABSTRACT
Post-operative pain is a common problem after surgical procedure. Undertreated and uncontrolled post-operative pain reduce physical and social performance, impaired quality of life and patient dissatisfaction, delayed discharge, increased use of health care resources and high cost on their hospital stay. Even if the problem is vast, researches on the area lack adequate data. This study aimed to assess knowledge, attitude and perceived barriers to post-operative pain management among anesthetists in Addis Ababa Governmental Hospitals, Ethiopia 2015. An institution based cross-sectional study was conducted. A survey method was undertaken to include a total of 150 anesthetists working in 11 government hospitals found in Addis Ababa, Ethiopia. Pretested structured self-administered questionnaire was used to collect the data. Data were entered and analyzed through SPSS version 20. Tables, graphs and frequencies were used to report the descriptive result. In total, 102 (68%) participants participated in the research. The mean score of correctly answered questions by the participants was 4.9 SD ±2.3, out of 12 items ranging from a minimum of 1 to a maximum of 11. Inadequate post-operative pain assessment, absence of pain management guideline and least priority for post-operative pain control are the major mentioned barriers by the participants. Anesthetist’s pain management knowledge and attitude level was found to be low. Strengthening educational strategy for surgical pain management and working on standard guidelines plays major role in alleviating the problem.
Key words: Attitude, Ethiopia, knowledge, perceived barriers, post-operative pain.
International Association for the Study of Pain (IASP) define pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage (Brennan et al., 2007).
The importance of post-operative pain management has been repeatedly demonstrated in the past two decades Adequate post-operative pain management (POPM) can reduce the patients’ length of hospitalization and reduce post-operative complications (Suwanraj, 2010). Pain causes an increase in the sympathetic response of the body with subsequent rise in heart rate, cardiac work, difficulty in breathing and oxygen consumption. Prolonged pain can reduce physical activity and lead to venous stasis and an increased risk of deep vein thrombosis and consequent pulmonary embolism (American Society of Anesthesiologists Task Force on Acute Pain, 2012; Gallagher et al., 2004). However, many researchers reported that unsatisfactory pain management were practiced in different countries (Taylor et al., 2008; Rejeh et al., 2008; Windsor et al., 1996).
Survey study from Malaysia and Ghana reported that the reason for poor management of acute pain in developing countries is absence of institutional training and national policy for pain management (Jawaid et al., 2009). In a study in Helsinki university hospital, proper management of post-operative pain was challenging to establish due to poor communication, insufficient assessment and the individual differences in the experience of pain (Kumar, 2007; Madenski, 2014).
In a study in Ethiopia, even though delivery of adequate pain control during the post-operative period is the responsibility and duty of health care providers, mainly anesthetists, they were not assigned in post-operative pain management recovery room and wards (Woldehaimanot et al., 2014).
Post-operative pain is not merely unpleasant for the patients and his/her relatives, but increases post-operative morbidity and possibly mortality and the number of unanticipated readmissions. In addition, it may cause chronic pain conditions which may be very difficult to treat. Therefore, in terms of patient safety and satisfaction, good post-operative pain control is important and is part of good clinical practice (Windsor et al., 1996;McDonnell et al., 2007; Aziato and Adejumo, 2013). Though the problem is broad, literatures on this area lack adequate data. Therefore, this study assesses knowledge, attitudes and perceived barriers to post-operative pain management among anesthetists working in Addis Ababa Governmental Hospitals, Ethiopia.
Institution based cross sectional study was conducted from May to June 2015 in 11 hospitals in Addis Ababa which is the capital city of Ethiopia. These hospitals are Tikur Ambessa Specialized Hospital, St Paul Specialized Hospital, Gandi Specialized Hospital, Army Specialized Hospital, Alert Specialized Hospital, Zewditu Specialized Hospital, Rasdesta Specialized Hospital, Tirunesh Beijing Specialized Hospital, Minilik Specialized Hospital, Yekatit Specialized Hospital and Police Specialized Hospital. All anesthetists working in the 11 government hospitals were included in the study through preliminary survey and those who were in any kind of leave were excluded. Data were collected through self-administer structured and pretested English language prepared questionnaire, which is adopted from British journals, the known Pain 50 tool and WHO pain management guidelines, 2008 and 2007 respectively (Brennan et al., 2007). Data were checked, cleaned manually, coded and entered into Epi Info version 5 and exported to SPSS version 20 for analysis. Percentage and frequencies calculated tables and graphs were used to report the descriptive result.
Participants were considered as knowledgeable if their answer to the knowledge related questions is greater or equal to 80% and those with good attitude were participants whose answer to the attitude questions was greater or equal to 80%.
Ethical consideration
Ethical clearance was obtained from Institution Review Board of Addis Ababa University and permission letter from Addis Ababa Health Office and from each government hospital, and finally after information provision, consent was obtained from each participant.
A total of 102 anesthetists with response rate of 68% participated in the study.
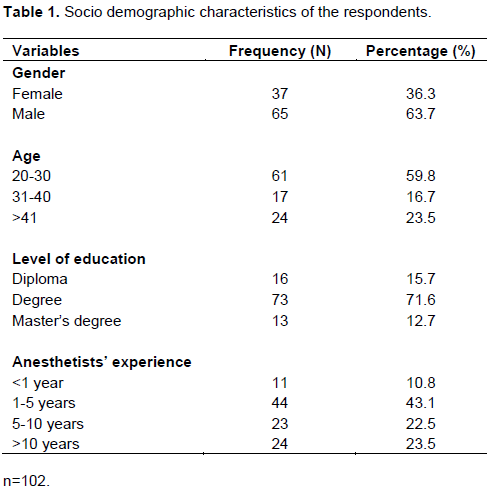
Socio demographic characteristics
Majority of the participants were male (65; 63.7%) and in the age group of 20 to 30, 61 (59.8%) with mean age of 32.2 and 73 (71.6%) were degree holders with regards to educational level. Forty-four (43.1%) of the participants had 1 to 5 years’ experience (Table 1).
Knowledge of participants on pain management
In this survey, majority (82; 80.4%) of the respondents had knowledge on paracetamol as NSAID (Table 2).
Knowledge score of participants
The mean score of correctly answered questions by the participants were 4.9 with standard deviation of ±2.3 out of 12 items ranging from a minimum of 1 to a maximum of 11 (Figure 1).
Attitude of participants
Majority (97; 95.1%) of the participants responded positively to the question, performing nerve blocks for surgical patients is effective in reducing complication and in early return to activities (Table 3).
Perceived barriers to pain management
In this study, major barriers to post-operative pain management are inadequate post-operative pain assessment (90; 88.2%), absence of pain management guideline (89; 87.3%) and post-operative pain control is not given priority (86; 84.3%) (Table 4).
Knowledge score of anesthetists’ in this study was found to be low as compared to other studies conducted in Ireland and UK (Vickers, 2011; Powell et al., 2009). This may be due to socio demographic, life style and educational background difference. The study also showed knowledge difference among anesthetists regarding their educational status. Masters level participants had better knowledge than Bsc. and diploma level anesthetists. This finding is consistent with study conducted in Ireland (McCAFFERY and Robinson, 2002)and different systematic review results (Powell et al., 2009). On the other hand, most incorrectly answered question by anesthetists was changes in vital signs are reliable indicators of pain severity (83.3%). This result is comparable to other similar literatures (Aziato and Adejumo, 2013; Vickers, 2011; McCAFFERY and Robinson, 2002). In addition, half the sample of respondents (49% of respondents) in this sample wrongly believed that patients’ cannot sleep in spite of severe pain. This result possibly shows anesthetists’ inadequate pain assessment skills (McDonnell et al., 2007).
Attitudes of anesthetists in this survey were found to be low. Significant attitude difference was seen among anesthetists in their educational status and work experience. Thirty-six (35.3%) of the respondents believed that working in collaboration with other professionals do not bring effective post-operative pain control. It was found that those who had diploma and longer working experience had a positive attitude towards collaboration and communication with other professionals than those who have Bsc, Msc and shorter working experience in effective pain control. This finding is in line with other studies (Kumar, 2007; Woldehaimanot et al., 2014). About 72% of anesthetists wrongly agreed that analgesic tolerance and addiction to opioids usually occurs following post-operative treatment, even though opioids have <1% risk of tolerance and addiction (Ariyanuchitkul and Petchdee, 2011). The result is relatively high as compared to other studies (American Society of Anesthesiologists Task Force on Acute Pain, 2012; Madenski, 2014; Woldehaimanot et al., 2014; Vickers, 2011; McCAFFERY and Robinson, 2002). This variance might be due to educational difference among participants.
Inadequate post-operative pain assessment and post-operative pain control are not given priority, and absence of pain management guideline was most frequently cited barriers by anesthetists. Most of the anesthetists who had low score on the knowledge section quoted lack of knowledge as most frequent barrier in the perceived barriers section of this survey.
Previous studies have shown that improving pain assessment procedures requires the caregiver to acknowledge and have faith in the patient's report (Jho et al., 2014).
CONCLUSION AND RECOMMENDATION
Knowledge and attitude level of respondents in this study was low. Inadequate post-operative pain assessment, absence of pain management guideline and giving least priority to post-operative pain control are major reasons mentioned as barrier. Working on the listed barriers with improved education and on job training plays major role in improving the utilization.
The authors declare that there is no conflict of interests.
REFERENCES
|
American Society of Anesthesiologists Task Force on Acute Pain Management (2012). Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology 116:248-273.
Crossref
|
|
|
|
Ariyanuchitkul T, Petchdee N (2011). Attitude, Knowledge and Practice of Nurse Anesthetist, Maharat Nakhon Ratchasima Hospital for Postoperative Pain Assessement and Treatment in Recovery Room. Maharat Nakhon Ratchasima Hospital Med. Bull. 32(1):S54-S61.
|
|
|
|
|
Aziato L, Oluyinka A (2013). "Perspectives of the Surgeons, Anaesthetists, and Pharmacists on Post-Operative Pain Management Roles in the Ghanaian Context." Afr. J. Phys. Health Educ. Recreation Dance 19(3):678-691.
|
|
|
|
|
Brennan F, Carr DB, Cousins M (2007). Pain management: a fundamental human right. Anesthesia & Analgesia 105(1):205-221.
Crossref
|
|
|
|
|
Gallagher R, Hawley P, Yeomans W (2004). A survey of cancer pain management knowledge and attitudes of British Columbian physicians. Pain Res. Manage. 9(4):188-194.
Crossref
|
|
|
|
|
Jawaid MA, Muhammad SH, Shafiq FA, Malik KA (2009). "Acute Post-operative Pain Management by a Surgical Team in a Tertiary Care Hospital: Patients Satisfaction." Middle East J. Anesthesiol. 20(3):405-410.
|
|
|
|
|
Jho HJ, Kim Y, Kong KA, Kim DH, Choi JY, Nam EJ, Koh S, Hwang KO, Baek SK, Park EJ (2014). "Knowledge, Practices, and Perceived Barriers Regarding Cancer Pain Management among Physicians and Nurses in Korea: A Nationwide Multicenter Survey." PloS One 9(8):e105900.
Crossref
|
|
|
|
|
Kumar N (2007). "WHO Normative Guidelines on Pain Management." Geneva: World Health Organization. pp. 3-4.
|
|
|
|
|
Madenski AD (2014). "Improving Nurses' Pain Management in the Post Anesthesia Care Unit (PACU)."
|
|
|
|
|
McCAFFERY MARGO, Eileen SR (2002). "Your Patient Is in Pain-here's How You Respond." Nursing2016 32(10):36-45.
|
|
|
|
|
McDonnell JG, O'donnell B, Curley G, Heffernan A, Power C, Laffey JG (2007). "The Analgesic Efficacy of Transversus Abdominis Plane Block after Abdominal Surgery: A Prospective Randomized Controlled Trial." Anesthesia Analgesia 104(1):193-197.
Crossref
|
|
|
|
|
Powell AE, Davies HT, Bannister J, Macrae WA (2009). "Challenge of Improving Post-operative Pain Management: Case Studies of Three Acute Pain Services in the UK National Health Service." Br. J. Anaesthesia 102(6):824-831.
Crossref
|
|
|
|
|
Rejeh N, Ahmadi F, Mohammadi E, Anoosheh M, Kazemnejad A (2008). "Barriers To, and Facilitators of Postâ€operative Pain Management in Iranian Nursing: A Qualitative Research Study." Int. Nurs. Rev. 55(4):468-475.
Crossref
|
|
|
|
|
Suwanraj M (2010). "Current Practice, Perceived Barriers, and Perceived Facilitators of Thai Nurses on Using Evidence-Based Pactice on Pain Assessment and Pain Management in Older Adults." The University of Iowa.
|
|
|
|
|
Taylor AL, Gostin LO, Pagonis KA (2008). "Ensuring Effective Pain Treatment: A National and Global Perspective." JAMA 299(1):89-91.
Crossref
|
|
|
|
|
Vickers N (2011). "Knowledge and Attitudes Regarding Pain among Surgical Nurses in Three Teaching Hospitals in Ireland."
|
|
|
|
|
Windsor AM, Glynn CJ, Mason DG (1996). "National Provision of Acute Pain Services." Anaesthesia 51(3):228-231.
Crossref
|
|
|
|
|
Woldehaimanot TE, Eshetie TC, Kerie MW (2014). "Post-operative Pain Management among Surgically Treated Patients in an Ethiopian Hospital." PloS One 9(7):e102835.
Crossref
|
|