Full Length Research Paper
ABSTRACT
Hypertension and Hypertensive Heart Failure (HHF) constitutes a growing burden of non-communicable forms of cardiovascular disease (CVD) in Africa. This work was designed to investigate Electrocardiogram (ECG) parameters in HHF subjects. A cross-sectional study involving 100 subjects of equal number of HHF and normal subjects were used. Questionnaires were administered; socio-demographic and medical profiles of the subjects were obtained. ECG of each of the participants was conducted and results read for P duration, PR interval, QRS duration, QTc and Sokolow-Lyon index. Among the subjects with HHF, 56% were elderly and 44% were middle-aged. 60% were farmers; 42% had no formal education. The systolic blood pressure (SBP) was 125.40±20.37 mmHg and 117.62±9 in HHF and normal subjects respectively while diastolic blood pressure (DBP) were 80.88±19.04 mmHg in HHF subjects and 71.84±6.48 mmHg in normal subjects. Heart rate on ECG was 87.66±18.31 and 70.08±8.472 bpm in HHF and normal subjects respectively. QRS duration was 0.13±0.12 and 0.07±0.017 s in the HHF and normal subjects respectively. The corrected QTc was 0.47±0.04 and 0.38±0.024 s in HHF and normal subjects respectively. The Sokolow-Lyon index was 3.81±1.73 and 2.09±0.56 s in HHF and normal subjects respectively. The mean QRS duration was 0.14±0.018 in male and 0.12±0.022 s in female HHF subjects. Sokolow-Lyon index was 3.90±1.68 and 3.56±1.80 s in the male and female HHF subjects respectively. The mean QTc was 0.44±0.036 in male and 0.49±0.036 s in female HHF subjects respectively. ECG heart rate was 92.09±21.204 bpm in the middle-aged and 84.17±15.178 bpm in the elderly HHF subjects. The corrected QT interval was 0.44±0.041 s in the middle-aged group and 0.50±0.031 s in the elderly. The study shows that most of the values of electrocardiogram parameters were higher in the HHF subjects than in the normal population. Also, there were gender and age-specific differences in electrocardiogram parameters obtained in HHF subjects.
Key words: Hypertension; heart disease; electrocardiogram
INTRODUCTION
Hypertension is responsible for about 7.5 million deaths worldwide every year. More than 80% of these deaths occur in young and middle-aged men and women in low-income countries. It has been projected that hypertension will increase by 89% in countries in sub-Saharan Africa compared with a rate of 24% in advanced countries (Patel and DiPette, 2015). 20 million adult Nigerians were hypertensive in 2010 with prevalence rate of 28.9%.This staggering figure is projected to rise to 39 million in 2030 with a prevalence rate of 30.8% (Ogah et al., 2015). Hypertension is defined as a systolic blood pressure (SBP) of ≥140 mmHg or a diastolic blood pressure (DBP) of ≥90 mmHg or both (Ani et al., 2017).
Much of the cardiovascular burden of hypertension is due to the complication of hypertension. Heart failure is a disease condition characterized by the inability of the heart to pump adequate blood to meet the demands of the body and/or doing so at increased filling pressures (Owusu and Adu-Boakye, 2013). It is broadly defined as a clinical syndrome characterized by dyspnea and fatigue, at rest or with exertion, due to structural and/or functional abnormalities of the heart. Hypertensive heart failure is the clinical manifestation of cardiac dysfunction caused by hypertension (Francis and Tang, 2003). Hypertension is the most common cause of heart failure in many parts of sub-Saharan Africa and it has been reported to account for up to 30% of hospital admissions for heart failure in West Africa. Systemic hypertension exerts chronic pressure overload on the heart leading to both structural and functional changes in the heart namely left ventricular hypertrophy and ventricular diastolic and systolic dysfunction, eventually culminating in clinically overt heart failure. Heart failure is also defined as a constellation of signs and symptoms resulting from the inability of the heart to pump blood forward at a sufficient rate to meet the metabolic demands of the body or the ability to do so only if the cardiac filling pressures are abnormally high, or both (Yelle and Chaudhry, 2010). Hypertensive heart failure is a significant cause of cardiovascular morbidity and mortality in Africa.
The ultimate goal in the management of the hypertensive patient is to achieve the maximum reduction in the long-term total risk of morbidity and mortality from hypertensive heart failure. This involves accurate assessment of the condition of the heart in patients with HHF. The electrocardiogram is an essential test in the evaluation of patients with hypertensive heart failure as it assesses structural changes for example left ventricular hypertrophy (LVH) conduction defects such as arrhythmias and atrial fibrillation in the heart (McMurray et al., 2012). Electrocardiogram remains an important keystone for the care of patients with cardiac diseases. It is painless, highly reproducible procedure with minimal or no risk to the patients. Compared with many other procedures, it is relatively inexpensive procedure (Schlant et al., 1992).
Despite the widespread use of ECG in clinical practice, there are limited data on the values of ECG parameters in patients with HHF in Nigeria. Heart failure is a disease condition characterized by the inability of the heart to pump adequate blood to meet the demands of the body and/or doing so at increased filling pressures (Owusu and Adu-Boakye, 2013). It is broadly defined as a clinical syndrome characterized by dyspnea and fatigue, at rest or with exertion, due to structural and/or functional abnormalities of the heart. Hypertensive heart failure is the clinical manifestation of cardiac dysfunction caused by hypertension (Francis and Tang, 2003).
Hypertensive heart disease (HHD) leads to three recognizable stages in evolution of heart failure: LVH, diastolic dysfunction, and systolic dysfunction. 16% of hypertensive patients were found to have depressed LV systolic function (de Simone, 1994). Abnormalities of left ventricular (LV) diastolic filling are observed in various forms of hypertension in adults (Vasan and Levy, 1996) and the prevalence may be as high as 22% in asymptomatic hypertensive patients with a BP of >140/ 90 mmHg. Diastolic filling abnormalities have been shown to generally correlate with LV mass, and BP (Ren et al., 1994). In hypertensive patients, diastolic heart failure is increasingly being recognized as a cause of Congestive heart failure (CHF). Common precipitants of overt heart failure in patients with diastolic dysfunction include old age, tachycardia, sudden severe increase in overload such as a hypertensive crisis (Shah and Pai, 1992). For example, in heart failure patients with preserved systolic function, the annual mortality was reported to be 8.7% v. 3.0% for matched controls, and in patients with LV systolic dysfunction, the annual mortality was 18.9% v. 4.1% for matched controls in the Framingham cohort (Vasan et al., 1999). Hence, treatment is required before the onset of clinical heart failure. Lowering of blood pressure is effective in preventing LVH and CHF, regardless of the agent used (Moser and Hebert, 1996). Hence, the main objective of this study was to achieve the maximum reduction in the long-term total risk of morbidity and mortality from hypertensive heart failure. This involves accurate assessment of the condition of the heart in patients with HHF.
MATERIALS AND METHODS
Study center
This study was conducted in the cardiology unit at the Department of Internal Medicine, Federal Teaching Hospital, Abakaliki (FETHA), Nigeria. The center is a tertiary institution located in the capital of
Ebonyi State in the South-Eastern region of Nigeria, which is one of the 36 states that make up the Federal Republic of Nigeria. The State has a population of about 2.17 million and a land area of about 12,502.46 km2 .The city itself has an estimated population of about 600,000 inhabitants. The center receives referrals from primary and secondary healthcare facilities within the state and neighboring states (Benue, Enugu, Abia and Cross River states).
Design and setting
This was a hospital-based cross-sectional survey study. 100 subjects comprising equal numbers of patients with HHF and normal non-hypertensive subjects were recruited. Hypertensive subjects were recruited from the cardiology unit at the Department of Internal Medicine, Federal Teaching Hospital, Abakaliki (FETHA), Nigeria while the normal subjects were recruited from among the staff of the hospital and outside the hospital after signing an informed consent.
Sample size
The sample size (N) was determined using the formula below:
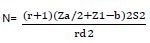
N=no of samples, Za/2=1.96 for 5% level of significance, Z1-b=0.84 at 80%statistical power, r=n1/n2 ratio of sample size for 2 groups of equal sample size.
S=common standard deviation=15, d=difference between values in previous study (Nwachukwu et al., 2015).
Computing the values above, Sample size (N) =81. To make room for 10% non-responders (calculated to be 9); the total sample size =90 for both cases and control subjects. However, 100 subjects of equal number of subjects with HHF and normal subjects were consecutively recruited.
Inclusion criteria
Only those patients who were given informed consent were enrolled in the study. A standardized diagnosis of hypertensive heart failure was made using Framingham criteria and those patients who met the criteria were recruited. Clinically unstable patients were excluded from the study.
Exclusion criteria
Pregnant women and individuals with clinical evidence of secondary hypertension were not included in the study. Patients with chronic diseases like renal failure, diabetes mellitus were also excluded from the study. Hypertensive patients who also had other complications of hypertension and other chronic diseases were excluded. Patients with clinically overt renal failure or on dialysis therapy were excluded from the study. Patients with Heart failure primarily caused by ischemic heart disease were also excluded.
Data collection
A standard case report forms (appendices I/II) were used in data collection. Patients’ baseline clinical and demographic variables such as age, sex, occupation, educational background, history of cardiovascular risk factors such as hypertension, family history, and cigarette smoking were collected. Signs and symptoms, and clinical diagnoses were also obtained.
Measurement of blood pressure
Blood pressure was recorded according to standard guidelines with the use of a mercury sphygmomanometer (Accuson, Siemens UK, London, United Kingdom) and stethoscope (3M™ Littmann®; USA). Systolic and diastolic BPs were measured at Korotkoff sounds phases I and V, respectively. BP was measured in right arm with the patient in the sitting position and cuff size was determined by the size of the patient’s arm. An average of two readings was taken after 5 min of rest.
A diagnosis of hypertensive HF (HHF) was made if the following criteria were met: clinical-confirmed diagnosis of HF in a known hypertensive or persistent BP ≥140/90 mm Hg in those who were not previously known hypertensive.
The patients recruited for this study met three or more of Framingham Heart Failure Diagnostic Criteria which include: Major criteria: cardiomegaly, hepatojugular reflex, neck vein distention, paroxysmal nocturnal dyspnea or orthopnea, third heart sound (S3 Gallop Rhythm). Minor criteria: bilateral ankle edema, dyspnea on exertion hepatomegaly, nocturnal cough, tachycardia (Heart Rate > 120 beats per minute).
Measurement of electrocardiogram
Electrocardiographic recording of each participant was obtained in supine position after about 5 min of rest during quiet respiration using the standard 12-leads Electrocardiogram (Schiller AG, Baar, Switzerland). The participants were enlightened about the protocol and their written consent obtained. Materials like wrist watch, jewelry, mobile phones were removed from the body to reduce electromagnetic interference. The limbs and chest were exposed and electrodes placed according to internationally approved protocol.
The chest lead recordings (V1-V6) were obtained by the attachment of six electrodes to the precordium according to the conventional methods; V1 at 4th intercostal space right sternal edge, V2 at 4th intercostal space left sternal edge, V3 at the point midway between V2 and V4, V4 at 5th intercostal space left mid-clavicular line, V5 and V6 were placed respectively at left anterior axillary line and mid-axillary line at same horizontal line with V4. An electrode was attached to each of the limbs to record limb leads. Before acquisition of the ECG, identification number, age, sex, weight, height and blood pressure were entered into the electrocardiograph. Standard 12-leads ECGs were recorded at a speed of 25 mm/s and calibration signal of 10 mm/mV. The results were printed out. ECG reports were analyzed given attention to ventricular rate, P duration, QT interval, corrected QT interval and Sokolow-Lyon index.
Statistical analysis
Data were presented as mean ±standard deviation, percentages and tables and were analyzed using statistical package for social sciences (SPSS) version 20 (SPSS, Inc., Chicago, Illinois).One way analysis of Variance (ANOVA) was used to compare the statistical significant difference. P <0.05 was considered significant.
RESULTS
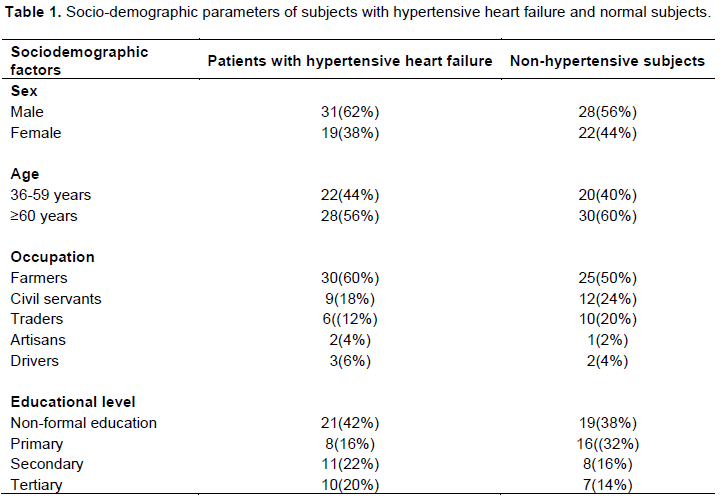
Table 1 depicts a total of 100 subjects comprising 50 patients with HHF and 50 normal subjects who were recruited for the study. Among the patients with HHF, those in the middle- aged group constituted 44% while the elderly constituted 56% while among the non-hypertensive normal subjects, those in the middle-aged group constituted 40% and the elderly constituted 60%. Among the HHF patients, 60% were farmers and those with non-formal education constituted 42%. The socio-demographic parameters in both the case and controls were comparable.
The mean Systolic BP in patients with HHF was 125.40±20.37 mmHg while it was 117.62±9.74 mmHg in the normal subjects. The mean diastolic BP among patients with HHF was 80.88±19.04 and 71.84±6.48 mmHg in the normal population. Blood pressure (systolic and diastolic) and heart rate were significantly higher in patients with hypertensive heart failure than in the normal non-hypertensive subjects as seen in Table 2.

The mean heart rate on ECG in Patients with HHF was 87.66±18.31 bpm while it was 70.08±8.472 bpm in the normal population. Heart rate on ECG was significantly higher in the patients than in the normal subjects (P<0.05). The mean QRS duration was 0.13±0.12s in patients with HHF and 0.07±0.017s in the normal subjects. The corrected QTc were 0.47±0.04s and 0.38±0.024s in patients with HHF and normal subjects respectively. The Sokolow-Lyon index was 3.81±1.73s and 2.09±0.56s in patients with HHF and normal subjects respectively.
Heart Rate, QRS duration, corrected QT and Sokolow-Lyon values were significantly higher in the patients with HHF than in the normal subjects (P<0.05). P Duration, PR interval and QT interval showed no significant differences between the case and control groups as seen in Table 3.

Among the patients with HHF, the mean (±SD) QRS duration was 0.14±0.018 s in male subjects and 0.12±0.022 s in female subjects. The mean (±SD) Sokolow-Lyon index was 3.90±1.68 and 3.56±1.80s in the male and female subjects respectively. The mean (±SD) QTc was 0.44±0.036 s in male patients and 0.49±0.036s in female patients. QRS duration and Sokolow-Lyon index were significantly higher in male subjects with HHF whereas QTc was longer in the female subjects with HHF (P<0.05). Other parameters showed no significant difference between the sexes as seen in Table 4.

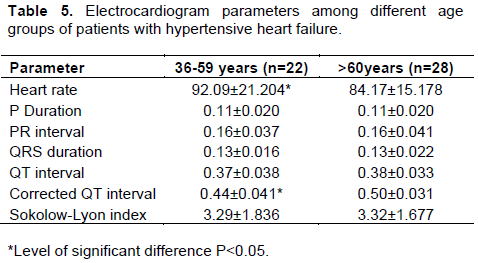
In Table 5, among the patients with HHF, the mean heart rate on ECG was 92.09±21.204bpm in middle-aged group and 84.17±15.178 bpm in the elderly. The corrected QT interval was 0.44±0.041 s in the middle-aged group and 0.50±0.031 s in the elderly. Heart rate was significantly higher in the middle age group (36-59 years) than in the elderly (≥60 years). Corrected QT interval was significantly higher in the elderly subjects (P<0.05).
DISCUSSION
In this study, the authors determined the values for ECG parameters in adult patients with hypertensive heart failure and compared them with ECG values in the normal population. Values of some ECG parameters were significantly higher in patients with HHF than those in the normal subjects. Our data also showed that age- and sex-dependent differences were apparent for some of the ECG parameters and may have clinical consequences. The 56% of the subjects with HHF were elderly while 44% were in the middle-aged group. The incidence of hypertension and hypertensive heart failure and risk of sudden cardiac death increases as a function of age (Verdecchia et al., 2019). This finding may be related to the fact that sodium sensitivity, systemic vascular resistance and stiffness of the vasculature increase with age (Foex and Sear, 2004). The risk of developing LVH, systolic dysfunction and clinically overt failure is higher above 60 years of age (Levy et al., 1996). In the present study, there were a greater number of men compared with women (62%vs 38%, respectively); most of the subjects with HHF had non-formal education (42%), and were farmers (60%). The burden of manual labor on already diseased heart in these farmers with non-formal education likely worsens the clinical outcome in this population. Countries with low-income status have substantially higher rates of cardiovascular morbidity and mortality compared with high-income countries (Patel and DiPette, 2015). In the present study, the values for mean systolic and diastolic BP in patients with HHF were 125 and 80 mmHg respectively compared with 117 and 71 mmHg respectively in the normal subjects. In a similar study, higher values of systolic and diastolic blood pressure of 143 and 91 mm Hg, respectively were reported (Patel and DiPette, 2015). Another study found even higher mean systolic BP and diastolic BP of 162 and 92 mmHg respectively (Owusu and Adu-Boakye, 2013). The lower values of systolic and diastolic BP which are close to the values in the normal population may be due to the use of anti-hypertensive in this population. It is also possible that most of the patients are already in type III hypertensive heart failure with cardiac decompensation characterized by recalcitrant lower blood pressure.
Also, heart rate was found to be significantly higher in patients with HHF than in the normal subjects. This finding agrees with that found in a similar study (Ogah et al., 2015). The mean heart rate of 80 beats per minute in this study was lower than mean heart rate of 96 beats per minute found in 80% of the patients in hypertensive heart failure of another study (Patel and DiPette, 2015). Higher heart rate in patients with HHF initially is beneficial as it helps to improve ejection fraction. However, raised resting heart rate in heart failure is a marker of cardiovascular risk (Bohm et al., 2015). QRS duration was found to be significantly higher in the heart failure patients compared to the control group (P<0.05). In a similar study conducted by Kashani and Barold (2005) it was noted that Prolongation of QRS which signifies intraventricular conduction delays occurs in 47% of heart failure (HF) patients and was associated with increased risk of left ventricular systolic dysfunction, ventricular tachyarrhythmias, poorer prognosis, and a higher rate of early mortality compared with narrow QRS duration. In another similar study by Wang et al. (2008), a higher mortality rate of 28.1% for patients with a prolonged baseline QRS duration (≥0.12 s) compared to 18.7% in patients with a normal baseline QRS duration(<0.12s) was noted. The mean ±SD of the QTc was 0.47 ±0.04 s which is significantly higher than mean QTc value of 0.38s ±0.024 in the normal population. In a related study, Rautaharju et al. (2007) derived normal limit of QTc interval as 0.42 s in the normal population. The prolonged QTc interval in patients with HHF likely represents a prolonged repolarization in ventricular conduction and this electrical abnormality may be due to disruption of cardiac conduction pathway by hypertension. QTc prolongation is considered an independent predictor of sudden cardiac deaths (SCD) in adults. Straus et al. (2006) studied the relationship between QTc interval and the probability of sudden cardiac death and found that as the degree of QTc prolongation worsened so too did the incidence of cardiovascular co-morbidities. In the present study, Sokolow-Lyon index was noted to be substantially higher in the patients with HHF than in the control (p<0.05).This observation is likely due to larger left ventricular mass due to chronic pressure overload imposed by hypertension on the left ventricle in hypertensive patients with heart failure. This finding is corroborated by other similar studies like the one done by Mandic et al. (2010) which also found that The Sokolow-Lyon voltage index as an ECG indicator of left ventricular chamber was significantly greater in males compared to females. P duration, PR interval and QT interval showed no significant differences in the case and control groups.Gender has significant influence on the ECG variables. The QRS duration was significantly longer in men than in women (P < 0.05). A greater QRS duration in men was also found by Gowda et al. (2006). It seems that sex differences in the amplitude of ventricular polarization reflected on the surface electrocardiogram are secondary to differences in left ventricular (LV) mass. Men have larger ventricular mass. In the same vein, QTc interval showed sex-specific differences. The mean corrected QT (QTc) interval was significantly higher in women than in men (p<0.05). Rijnbeek et al. (2014) who studied ECG values in the normal population also found female preponderance in QTc intervals. Longer QTc in females is observed both in the normal population and in patients with HHF. Androgen and estrogen levels may explain the gender differences in QTc interval. Estrogens facilitate prolongation of the corrected QT interval. The male corrected QT interval shortens at puberty and remains shortened until about 50 years of age; a period coinciding with the highest androgen levels (Rabkin, 2014). The Sokolow–Lyon voltage criterion which measures LV mass was increased in both sexes but was found to be higher in the male adults with HHF than in the female counterparts. The higher value in men is likely due to the larger left ventricular mass compared to women. Although men have higher voltage sum, there is survival disadvantage conferred by LVH in women. In the presence of ECG LVH, women have a substantially higher risk of dying from stroke and other cardiovascular events (Antikainen et al., 2006). In the present study, PR interval was a trifle longer in male patients than in female counterparts but there was no significant difference between the sexes. In contrast, Mandic et al. (2010) noted a significantly higher PR interval in male subjects than in the female subjects. Middle-aged group have higher heart rate than the elderly subjects. In contrast, Rijnbeek et al., (2014) in their study in normal population found no significant difference in heart rate between the normal middle-aged and elderly individuals. A much higher heart rate in middle-aged population with HHF may have clinical significance since increased heart rate is a cardiovascular risk factor and this may account for increasing burden of HHF in middle-aged group especially in blacks (Ogah et al., 2015). The QTc was notably higher in the elderly than in the middle-aged group. QTc increases in duration with increasing age (Rabkin, 2014). According to the population-based Rotterdam Study, a prolonged corrected QT interval was found to be an independent predictor for increased risk of cardiovascular mortality in older men and women. Other ECG parameters showed no significant difference between the two age groups studied.
CONCLUSION
The data of this study show that heart rate, QRS duration, QTc interval and Sokolow-Lyon index were significantly higher in the subjects with HHF than in normal subjects. Also, this study demonstrates important gender differences in ECG parameters in patients with HHF; women have longer QTc interval while men have longer QRS duration and higher Sokolow-Lyon index. Our study also showed age differences in heart rate and QTc which were higher in the middle-aged group and the elderly respectively. This work furnishes information for astute clinical judgment when interpreting ECG in patients with hypertensive heart failure as it provides a frame of reference of ECG parameters and evaluates the impact of gender and age on ECG in this population.
RECOMMENDATION
Establishment of reference values of ECG in all facets of population with hypertension may be needed. Cohort study evaluating the relationship between ECG values and clinical outcome in patients with HHF may also be needed. There is the need to improve the awareness of HHF as a complication of hypertension. The use of reference ranges of ECG established in this work and awareness of impact of age and sex on ECG parameters in HHF by clinicians will improve management in these patients.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors sincerely acknowledge the management and staff of Federal Teaching Hospital Abakalikki Nigeria for granting them the privilege to use the hospital facilities in the research. Our gratitude also go to Prof Nwachukwu Daniel who initiated as well supervised this research work. Authors also appreciate the entire Technologist (Ani Celestine) who technical knowledge led to the success of this research.
REFERENCES
|
Ani CO, Augustine AO, Chinemerem NC, Jide UU, Pamela OO, Francis AU, Daniel NC (2017). Investigation of antihypertensive effect of Nigerian varieties of Solanum lycopersicon on rats. African Journal of Pharmacy and Pharmacology 11(34):419-425. |
|
|
Antikainen RL, Grodzicki T, Palmer AJ, Beevers DG, Webster J, Bulpitt CJ (2006) Left ventricular hypertrophy determined by Sokolow-Lyon criteria: a different predictor in women than in men? Journal of Human Hypertension 20(6):451-459.. |
|
|
Bohm S, Madamili L, Mersmann F, Adamantios A (2015). Predictive and Reactive locomotor adaptability in healthy elderly: A systematic review and meta-analysis. Sports Medicine 45:1759-1777 |
|
|
De Simone G, Devereux RB, Roman MJ, Ganau A, Saba PS, Alderman MH (1994) Assessment of left ventricular function by midwall fractional shortening/end-systolic stress relation in human hypertension. Journal of American College of Cardiology 23:1444-1451. |
|
|
Foex P, Sear JW (2004). Hypertension: Pathophysiology and treatment. Continuing Education in Anaesthesia Critical Care and Pain 4(3):71-75. |
|
|
Francis GS, Tang WHS (2003). Pathophysiology of Congestive Heart Failure. Review of Cardiovascular Medicine 4(2):14-20. |
|
|
Kashani A, Barold SS (2005). Significance of QRS complex duration in patients with heart failure. Journal of American College of Cardiology, 46(12):2183-2192. |
|
|
Levy D, Larson MG, Vasan RS, Kannel WB, Ho KK (1996). The progression from hypertension to congestive heart failure. The Journal of the American Medical Association 275(20):1557-1562 |
|
|
Mandic S, Fonda H, Dewey F, Lev S, Wheeler M, Ashley E (2010). Effect of Gender on Computerized Electrocardiogram Measurements in college athletes. The Physician and Sports Medicine 38(2):1-9. |
|
|
McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M (2012). ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. European Heart Journal 33:1787-1847 |
|
|
Moser M, Hebert PR (1996). Prevention of disease progression, left ventricular hypertrophy and congestive heart failure in hypertension treatment trials. Journal of American College ofl Cardiology 27:1214-1218. |
|
|
Nwachukwu DC, Aneke EI, Nwachukwu NZ, Obika LF, Nwagha UI, Eze AA (2015). Effect of hibiscus sabdarifa on blood pressure and electrolyte profile of mild to moderate hypertensive Nigerian: A comparative study with hydrochlorothiazide. Nigerian Journal of Clinical Practice 18(6):762-770. |
|
|
Ogah OS, Sliwa K, Akinyemi JO, Falase AO, Stewart S (2015). Hypertensive heart failure in Nigerian Africans: Insights from the Abeokuta heart failure registry. The Journal of Clinical Hypertension 17(4):263-272. |
|
|
Owusu IK, Adu-Boakye Y (2013). Prevalence and Aetiology of Heart Failure in Patients Seen at a Teaching Hospital in Ghana. Journal of Cardiovascular Diseases and Diagnosis 1(5):1-4. |
|
|
Patel P, Donald J, DiPette DJ (2015). Hypertension-Related Congestive Heart Failure in West Africa:A Framework for Global Blood Pressure Control. Journal of Clinical Hypertension 17(4):260-262. |
|
|
Rabkin SW (2014). Aging effects on QT interval: Implications for cardiac safety of antipsychotic drugs. Journal of Geriatric Cardiology 11(1):20-25. |
|
|
Rautaharju PM, Prineas RJ, Kadish A, Larson JC, Hsia J, Lund B (2006). Normal standards for QT and QT subintervals derived from a large ethnically diverse population of women aged 50-79. American Journal of Cardiology 97(5):730-737. |
|
|
Ren JF, Pancholy SB, Iskandrian AS, Lighty GW, Mallavarapu C, Segal BL (1994). Doppler echocardiagraphic evaluation of the spectrum of left ventricular diastolic dysfunction in essential hypertension. American Heart Journal 127(4):906-913 |
|
|
Rijnbeek PR, HerpenGV, Bots ML, Mans S, Verweij N, Hofman A (2014). Normal values of the electrocardiogram for ages 16-90 years. Journal of electrocardiology 47(6):914-921. |
|
|
Schlant RC, Adolph RJ, Dimarco JP (1992). Guidelines for electrocardiography. A report of the American college of Cardiology/American Heart Association Task force on Assessment of Diagnostic and Therapeutic Cardiovascular procedures. Circulation 859(3):1221-1228. |
|
|
Shah PM, Pai RG (1992). Diastolic heart failure. Current Problem in Cardiology 17:781-868. |
|
|
Straus SM, Kors JA, De Bruin ML (2006). Prolonged QTc interval and risk of sudden cardiac death in a population of older adults. Journal of American College of Cardiology 47(2):362-367. |
|
|
Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D (1999). Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. Journal American College of Cardiology 33(7):1948-1955. |
|
|
Vasan RS, Levy D (1996). The role of hypertension in the pathogenesis of heart failure: A clinical mechanistic overview. Archives of Internal Medicine 156:1789-1796. |
|
|
Verdecchia P, Fabio A, Claudio C, Adolfo A, Dario T, Michelantonio D, Gianpaolo R (2019). Sudden Cardiac death in hypertensive Patients. Hypertension 73(5):1071-1078. |
|
|
Wang NC, Maggioni PA, Konstam MA, Zannad F, Krasa HB, Burnett JC (2008). Clinical Implications of QRS Duration in Patients Hospitalized With Worsening Heart Failure and Reduced Left Ventricular Ejection Fraction. Journal of American Medical Association 299(22):2656-2666. |
|
|
Yelle D, Chaudhry S (2010). Heart Failure. New England Journal of Medicine 348(20):2007-2018. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


