Full Length Research Paper
ABSTRACT
Hepatocellular carcinoma (HCC) is the most common primary malignant tumor of the liver. The lack of efficient and precise HCC biomarkers prevents early detection resulting in a poor prognosis. Recently, mean platelet volume (MPV) and MPV/platelet count (PC) ratio have been proposed as potential markers of HCC. This study was carried out to verify MPV and MPV/PC ratio in diagnosis of HCC in Egyptian patients with chronic hepatitis C related liver cirrhosis. One hundred and fifty chronic hepatitis C (CHC) patients with chronic hepatitis, cirrhosis or HCC were enrolled in the study. The levels of alphe feto protein (AFP), MPV and MPV/PC ratio were determined compared to 50 healthy persons. MPV and MPV/CP ratio were higher in patients with cirrhosis and those with HCC. The cut off level for MPV for detection of HCC was 10.1 fl, with sensitivity of 70% and specificity of 57%. At a cut off level of 0.82, the sensitivity of MPV/CP ratio was 79.6% and specificity was 72.7%. AFP showed sensitivity 80% and specificity 82% at cut-off level of 16.9 ng/dl. MPV and MPV/PC ratio are less sensitive and specific than AFP as markers for HCC; they may be used only in association with other markers to improve sensitivity of tumor detection.
Key words: Hepatocellular carcinoma, mean platelet volume, platelet count, cirrhosis, hepatitis C.
INTRODUCTION
Hepatocellular carcinoma (HCC) is the most common primary malignant tumor of the liver and remains a leading cause of death worldwide (Torre et al., 2012). The diagnosis of HCC can be difficult as patients usually have no symptoms other than those related to their chronic liver disease. The most commonly used marker for HCC is the serum alpha-fetoprotein (AFP) concentration. However, analysis of recent studies showed that AFP determination lacks adequate sensitivity and specificity for diagnosis (Lok et al., 2010). The lack of efficient and precise HCC biomarkers prevents early detection resulting in a poor prognosis.
Disorders of platelets count are common in various stages of liver diseases. Thrombocytopenia tends to predominate in patients with cirrhosis whereas normal, or even higher counts, including thrombocytosis are more common in patients with HCC (Carr et al., 2014; Carr and Guerra, 2013).
Mean platelet volume (MPV) is a parameter of routine blood count that provides an insight into platelet function and activation (Bath and Butterworth, 1996). Changes of MPV have been actively investigated in many liver diseases (Ceylan et al., 2014; Cho et al., 2013). MPV values were found to be elevated in patients with nonalcoholic fatty liver disease, intrahepatic cholestasis of pregnancy, chronic hepatitis, and liver cirrhosis (Cho et al., 2015; Kocabay et al., 2014; Karagoz and Tanoglu, 2014; Purnak et al., 2013; Celikbilek et al., 2013; Balta et al., 2013; Ozhan et al., 2010; Kebapcilar et al., 2010). MPV had been found to be correlated positively with the severity of histological grade in patients with primary biliary cirrhosis (PBC) (Tahtaci et al., 2015). Recently, MPV and MPV/platelet count (PC) ratio have been proposed as candidate markers for the diagnosis of HCC in patients with chronic liver disease (Cho et al., 2012; Kurt et al., 2011).
This study was carried out to verify the value of MPV and MPV/PC ratio in diagnosis of HCC in Egyptian patients with chronic hepatitis C (CHC) related liver cirrhosis.
MATERIALS AND METHODS
One hundred and fifty CHC patients plus fifty healthy volunteers were enrolled in the study. Patients were classified according to their clinical, laboratory and imaging characteristics into 3 equal groups: 50 patients with CHC without liver cirrhosis, 50 patients with liver cirrhosis due to CHC and 50 HCC patients on top of CHC liver cirrhosis. 50 healthy volunteers were also recruited as a control group. All control subjects were confirmed to have normal liver with no viral hepatitis, significant alcohol consumption or other chronic liver diseases.
The diagnosis of cirrhosis was based on clinical, laboratory, and imaging findings. The diagnosis of HCC was made by the presence of HCC radiological hallmarks in imaging technique (computed tomography (CT) and/or dynamic magnetic resonance imaging (MRI)) ± histopathological examination if needed (Bruix and Sherman, 2011; European Association, 2012).
Inclusion criteria included age above 18 years and positive PCR for hepatitis C virus (HCV) RNA. Patients with other causes of liver disease, sepsis, malignancy other than HCC, diabetes mellitus, dyslipidemia, rheumatologic diseases, advanced cardiac, renal or other chronic disease were excluded from this study.
The study was conducted with the approval of the Ethics Committees of National Liver Institute, Menoufiya University, Egypt. All contributors gave written informed consent prior to participation. The work has been carried out in accordance with the code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments in humans.
All patients were subjected to full history taking and complete physical examination, laboratory tests including complete blood count particularly platelets count (PC) and mean platelet volume (MPV), liver profiles, serum AFP level, hepatitis markers (HCV Ab, HBsAg, HBc total Ab) and HCV RNA PCR. Abdominal ultrasonography, triphasic abdominal CT and/or dynamic MRI were performed stressing on liver size, texture, focal lesion, portal vein diameter and patency, spleen size and presence of ascites.
Statistical analysis
Data were statistically analyzed using IBM® SPSS® Statistics® version 21 for Windows. Data were expressed as mean ± standard deviation for numerical data and number with percentage for ordinal and nominal variables.
Comparisons between two groups of HCC regarding lesions number and presence of portal vein thrombosis were performed using Mann-Whitney test. Comparisons between all studied groups were performed by one-way analysis of variance (ANOVA) test. If p<0.05, sub-analysis was done using Scheffé's method for post hoc test.
Chi-squared test (c2) and Fisher exact test were used for categorical data analysis. The receiver operating characteristic (ROC) curve analysis was used for detection of the cutoff value of AFP, MPV and MPV/PC ration.
All p-values are 2 tailed, with values <0.05 considered statistically significant.
RESULTS
Patients characteristics
The demographic and biochemical characteristics of the 3 groups of patients and controls are shown in Table 1. No significant differences regarding age or gender distribution existed between groups.

Platelets markers and AFP
The levels of AFP, MPV and MPV/PC ratio were determined in all patients and compared with 50 healthy persons. MPV levels and MPV/PC ratios showed significant difference among groups (P<0.001). Mean level of MPV was 8.9±1.8 in chronic hepatitis, 10.8±1.4 in patients with liver cirrhosis, 10.9±1.7 in HCC patients and 9.9±0.9 fl in controls (Figure 1). MPV/PC ratio was 0.49±0.14 in chronic hepatitis, 1.48±0.79 in patients with liver cirrhosis, 1.33±0.7 in HCC patients and 0.37±0.13 fl 10−4 μl−1 in controls (Figure 2).


By post hoc test, MPV and MPV/CP ratios were higher in patients with HCC and in patients with liver cirrhosis (P<0.001) when compared with controls and patients with CHC. However, no significant differences were found between patients with LC and those with HCC regarding platelets count (P=0.98), MPV (P=0.94) and MPV/PC ratio (P=0.69). Marked elevation of AFP level was observed in patients with HCC in comparison with healthy control subjects, patients with CHC and patients LC (P<0.001) (Figure 3).

AFP was significantly higher in patients with multiple focal lesions than in patients with single HCC (p<0.01). MPV and MPV/PC ratio had no association with local lesion number in HCC patients (p =0.97 and 0.76, respectively). No correlation was found between levels of studied markers and presence of portal vein thrombosis (Table 2).

Using receiver operating characteristic (ROC) curve analysis, the cut off level for MPV for detection of HCC was 10.1 femtolitre (fl), with sensitivity 70%, specificity 57.3%, area under the curve (AUC): 0.67 (0.579 to 0.760), p <0.001. At a cut off level of 0.82 fl 10−4 μl−1, the sensitivity of MPV/PC ratio was 79.6%, specificity was 72.7%, AUC was 0.777 (0.710 – 0.844), p <0.001 (Table 3).

Both MPV level and MPV/PC ratio showed lower sensitivity and specificity for diagnosis of HCC than AFP which showed sensitivity 80.1% and specificity 82% at cut-off level of 16.9 ng/dl, AUC: 0.884 (0.832 to 0.936), p <0.001 (Table 4 and Figure 4).
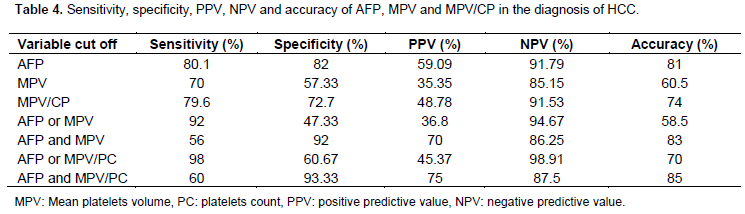

When the cut off levels for both AFP and MPV were used together, had a specificity of 92%, while when used separately, they had a sensitivity of 92%, but specificity dropped to 47.3%. Similarly, concurrent use of AFP and MPV/PC ratio cut off levels showed sensitivity of 60% and specificity of 93.3%, whereas discrete use of either of them revealed higher sensitivity (98%) and lower specificity of 60.7% (Table 4).
DISCUSSION
Determination of mean platelet volume (MPV) is a routine measure that is part of a complete blood count. MPV has been investigated in various clinical fields including chronic liver diseases.
In the literature, there are only a few studies examining the relationship between MPV or MPV/PC and HCC (Cho et al., 2013; Kurt et al., 2011). Hence, this cross-sectional study conducted involves 150 patients with various clinical spectrums of HCV infection including patients without cirrhosis, with liver cirrhosis and those with HCC on top of HCV related liver cirrhosis, aiming to explore the validity of MPV and MPV/PC as diagnostic tool for HCC.
Increased interleukin-6 (IL-6) production is implicated in the pathogenesis of hepatocellular carcinoma (HCC) (Wong et al., 2009). IL-6 is strong inflammatory indicator that seems to be useful in predicting the development of HCC and treatment outcome in patients receiving loco-regional therapy (Wong et al., 2009; Jang et al., 2012). High serum levels of IL-6 are associated with independent increase in HCC risk (Ohishi et al., 2014).
On the other hand, high IL-6 levels enhance platelet generation in the bone marrow. Thus, MPV values increase because of the increase in the number of young platelets entering into circulation and rapid activation and growth of platelets (Kaser et al., 2001). For these reasons, we would expect to find increased MPV in patients with HCC.
Chronic hepatitis caused by hepatitis C virus (HCV) has been documented as a possible cause of thrombocytopenia, even in the absence of cirrhosis (Fouad, 2013; Osada et al., 2012). This was demonstrated in the present study as the mean platelet counts were significantly lower in patients with CHC than control subjects. Additionally, mean platelet count in patients with liver cirrhosis was significantly lower than non-cirrhotic patients and the control subjects. This is the expected abnormality of platelet count in cirrhosis. The mechanisms responsible for thrombocytopenia in chronic liver disease include suppression of platelet production in the bone marrow (Wang et al., 2004), decreased activity of the hematopoietic growth factor, thrombopoietin (Rios et al., 2005) and splenic sequestration of platelets in portal hypertension (Rios, 1966; Peck-Radosavljevic, 2000; Afdhal et al., 2008), which is produced primarily in the liver. There is also increased destruction of platelets in patients with chronic liver disease by immunological mechanisms that result from increased levels of platelet-associated immunoglobulins (PAIgG) (Pereira et al., 1995; Sanjo et al., 2003).
Mean platelet count in patients with HCC was higher than that in cirrhosis in our study, but did not reach significant level. High platelet count and even thrombocytosis is common in many malignant diseases (Carr, 2014) including those of the ovary (Stone et al., 2012), gastrointestinal tract (Voutsadakis, 2014), and liver (Carr and Guerra, 2013; Hwang et al., 2004).
Increased platelet count in patients with malignancies may be explained by the link between platelets and angiogenesis (Pinedo et al., 1998; Olas et al., 1999; Banks et al., 1998). Certain types of malignancy can activate platelets in vitro through direct contact, release of ADP, production of thromboxane A2 or cancer procoagulant, generation of thrombin, or activation of the tumor-associated proteinases (Olas et al., 1999). In the presence of vascular endothelial growth factor (VEGF), which is a platelet-derived cytokine, endothelial cells promote platelet aggregation (Verheul et al., 2000). Adhesion and aggregation of activated platelets are accompanied by the release of many potential angiogenesis regulators such as VEGF-A (Ukropec et al., 2000), VEGF-C (Wartiovaara et al., 1998) and platelet-derived endothelial cell growth factor (PD-ECGF) (Griffiths and Stratford, 1997). These observations suggest that platelets may play an active and causative role in tumor angiogenesis (Pinedo et al., 1998).
Carr et al. (2014) reported that extracts from normal human platelets could stimulate growth in vitro in several human HCC cell lines. The extracts also inhibited apoptosis and stimulated HCC cell migration and invasion. Platelets therefore can be considered a micro-environmental factor in HCC cell growth (Carr et al., 2014).
Our study showed that the patients with HCC have higher AFP rather than cirrhotic patients; however, MPV and MPV/PC ratio values failed to show significant difference between patients with LC and HCC. Both values had higher levels in patients with liver cirrhosis than CHC non-cirrhotic patients. These findings suggest that MPV and MPV/PC may be potential markers for liver fibrosis in CHC patients. Similarly, Purnak et al. (2013) reported that MPV is increased in CHC patients with advanced fibrosis. In patients with cirrhosis, splenomegaly-induced platelet sequestration has been considered to be the main reason for the decrease in platelet survival, and hence, increase in MPV (Aster, 1966).
The cut-off value for MPV in our study for the detection of HCC in cirrhotic patients was 10.1 fl using ROC analysis (sensitivity: 70%, specificity: 57.3%). On the other hand, Kurt et al. (2011) calculated the cut-off value for MPV for the detection of HCC as ≥ 9.2 fl with sensitivity of 68.3% and specificity of 69.2% (Kurt et al., 2011). Additionally, they reported that serum MPV levels showed higher sensitivity for diagnosis of HCC than AFP (Kurt et al., 2011). On the contrary, we showed that serum MPV level was less sensitive (70%) for diagnosis of HCC than AFP (78%). Kurt et al. (2011) reported lower specificity of serum MPV levels (69.2%) for diagnosis of HCC than that of AFP (89.5%) and this agrees with our result that shows also lower specificity of serum MPV levels (57.33%) than AFP (82%).
In our study when the cut off levels for both AFP and MPV were put together; the specificity increased to 92%, while when used separately, they had also a higher sensitivity of 92%. On the other hand, using both AFP and MPV/PC ration had a high specificity (93.3%), while when used independently, sensitivity improved to 98%. Comparable results were reported by Kurt et al. (2011).
There are a few limitations in the current study. The cross-sectional nature of this study provides only a snapshot; it may provide different results if another time frame had been chosen and prevalence-incidence bias is expected in this study. Thrombopoietin levels were not done in the present study, as well as other inflammation markers such as neutrophil–lymphocyte ratio and serum C-reactive protein level.
MPV values may be affected by smoking habits, hypertension, diabetes, dyslipidemia, atherosclerotic diseases, venous thromboembolism, rheumatologic diseases, and inflammatory bowel diseases (Gasparyan et al., 2011). Although, patients with most of the aforementioned factors were not included in our study. The possibility that the presence of subclinical aspects that may affect our results cannot be ignored.
CONCLUSION
MPV is quick, easy and cheap to measure. However, MPV and MPV/PC ratio are less sensitive and specific than AFP as markers for HCC. Therefore, they may be used only in association with other markers like AFP to improve sensitivity of tumor detection.
Further studies with larger samples should evaluate them as non-invasive markers for fibrosis and as adjunctive indicator for HCC in patients with chronic liver disease. Further follow-up of the patients with CLD and higher MPV values (>10.1) to observe the development of HCC would provide more reliable data.
ACKNOWLEDGEMENT
The authors thank all staff members of Hepatology and Clinical Pathology Departments in National Liver Institute, Menoufiya University for their help in collection of our data.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Afdhal N, McHutchison J, Brown R, Jacobson I, Manns M, Poordad F, Weksler B, Esteban R (2008). Thrombocytopenia associated with chronic liver disease. J. Hepatol. 48(6):1000-1007. |
|
|
Aster RH (1966). Pooling of platelets in the spleen: role in the pathogenesis of "hypersplenic" thrombocytopenia. J Clin. Invest. 45(5):645-657. |
|
|
Balta S, Demirkol S, Akgul EO (2013). Mean platelet volume as a surrogate marker of inflammation in patients with chronic hepatitis B. Eur. J Gastroenterol. Hepatol. 25(11):1364. |
|
|
Banks RE, Forbes MA, Kinsey SE, Stanley A, Ingham E, Walters C, Selby PJ (1998). Release of the angiogenic cytokine vascular endothelial growth factor (VEGF) from platelets: significance for VEGF measurements and cancer biology. Br. J. cancer 77(6):956. |
|
|
Bath PM, Butterworth RJ (1996). Platelet size: measurement, physiology and vascular disease. Blood Coagul. Fibrinolysis 7(2):157-161. |
|
|
Bruix J, Sherman M (2011). American Association for the Study of Liver D. Management of hepatocellular carcinoma: an update. Hepatology 53(3):1020-1022. |
|
|
Carr BI (2014). Guest editorial: Platelets and cancer. Semin Oncol.41(3):300-301. |
|
|
Carr BI, Cavallini A, D'Alessandro R, Refolo MG, Lippolis C, Mazzocca A, Messa C (2014). Platelet extracts induce growth, migration and invasion in human hepatocellular carcinoma in vitro. BMC cancer 14(1):1. |
|
|
Carr BI, Guerra V (2013). Thrombocytosis and hepatocellular carcinoma. Dig. Dis. Sci. 58(6):1790-1796. |
|
|
Carr BI, Lin CY, Lu SN (2014). Platelet-related phenotypic patterns in hepatocellular carcinoma patients. Semin. Oncol. 41(3):415-421. |
|
|
Celikbilek M, Gursoy S, Deniz K, Karaman A, Zararsiz G, Yurci A (2013). Mean platelet volume in biopsy-proven non-alcoholic fatty liver disease. Platelets 24(3):194-199. |
|
|
Ceylan B, Fincanci M, Yardimci C, Eren G, Tözalgan Ü, Müderrisoglu C, Pasaoglu E (2014). Mean platelet volume in chronic viral hepatitis. Eur. J. Gastroenterol. Hepatol. 26(2):240-241. |
|
|
Cho SY, Lee A, Lee HJ, Suh JT, Park TS (2012). Mean platelet volume in Korean patients with hepatic diseases. Platelets 23(8):648-649. |
|
|
Cho SY, Lee HJ, Park TS (2015). Mean platelet volume in patients with increased gamma-glutamyl transferase. Platelets 26(3):283-284. |
|
|
Cho SY, Yang JJ, You E, Kim BH, Shim J, Lee HJ, Lee WI, Suh JT, Park TS (2013). Mean platelet volume/platelet count ratio in hepatocellular carcinoma. Platelets 24(5):375-377. |
|
|
European Association (2012). European Association For The Study Of The L, European Organisation For R, Treatment Of C. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J. Hepatol. 56(4):908-943. |
|
|
Fouad YM (2013). Chronic hepatitis C-associated thrombocytopenia: aetiology and management. Trop Gastroenterol. 34(2):58-67. |
|
|
Gasparyan AY, Ayvazyan L, Mikhailidis DP, Kitas GD (2011). Mean platelet volume: a link between thrombosis and inflammation? Curr. Pharm. Des. 17(1):47-58. |
|
|
Griffiths L, Stratford IJ (1997). Platelet-derived endothelial cell growth factor thymidine phosphorylase in tumour growth and response to therapy. Br. J Cancer 76(6):689-693. |
|
|
Hwang SJ, Luo JC, Li CP, Chu CW, Wu JC, Lai CR, Chiang JH, Chau GY, Lui WY, Lee CC, Chang FY (2004). Thrombocytosis: a paraneoplastic syndrome in patients with hepatocellular carcinoma. World J. Gastroenterol. 10(17):2472-2477. |
|
|
Jang JW, Oh BS, Kwon JH, You CR, Chung KW, Kay CS, Jung HS (2012). Serum interleukin-6 and C-reactive protein as a prognostic indicator in hepatocellular carcinoma. Cytokine 60(3):686-693. |
|
|
Karagoz E, Tanoglu A (2014). Prognostic role of mean platelet volume in patients with chronic hepatitis C. Clin. Res. Hepatol. Gastroenterol. 38(6):e113. |
|
|
Kaser A, Brandacher G, Steurer W, Kaser S, Offner FA, Zoller H, Theurl I, Widder W, Molnar C, Ludwiczek O, Atkins MB (2001). Interleukin-6 stimulates thrombopoiesis through thrombopoietin: role in inflammatory thrombocytosis. Blood 98(9):2720-2725. |
|
|
Kebapcilar AG, Taner CE, Kebapcilar L, Bozkaya G (2010). High mean platelet volume, low-grade systemic coagulation, and fibrinolytic activation are associated with pre-term delivery and low APGAR score in intrahepatic cholestasis of pregnancy. J. Matern. Fetal Neonatal Med. 23(10):1205-1210. |
|
|
Kocabay G, Karabay CY, Kalayci A, Colak Y (2014). Mean platelet volume in patients with non-alcoholic fatty liver disease: is mean platelet volume ready as a surrogate marker? Clin. Chem. Lab. Med. 52(11):e249-252. |
|
|
Kurt M, Onal IK, Sayilir AY, Beyazit Y, Oztas E, Kekilli M, Turhan N, Karaman K, Akdogan M (2011). The role of mean platelet volume in the diagnosis of hepatocellular carcinoma in patients with chronic liver disease. Hepato-gastroenterology 59(117):1580-1582. |
|
|
Lok AS, Sterling RK, Everhart JE, Wright EC, Hoefs JC, Di Bisceglie AM, Morgan TR, Kim HY, Lee WM, Bonkovsky HL, Dienstag JL (2010). Des-γ-carboxy prothrombin and α-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma. Gastroenterology 138(2):493-502. |
|
|
Ohishi W, Cologne JB, Fujiwara S, Suzuki G, Hayashi T, Niwa Y, Akahoshi M, Ueda K, Tsuge M, Chayama K (2014). Serum interleukinâ€6 associated with hepatocellular carcinoma risk: A nested case–control study. Int. J. Cancer 134(1):154-163. |
|
|
Olas B, Mielicki WP, Wachowicz B, Krajewski T (1999). Cancer procoagulant stimulates platelet adhesion. Thromb. Res. 94(3):199-203. |
|
|
Osada M, Kaneko M, Sakamoto M, Endoh M, Takigawa K, Suzuki-Inoue K, Inoue O, Satoh K, Enomoto N, Yatomi Y, Ozaki Y (2012). Causes of thrombocytopenia in chronic hepatitis C viral infection. Clin. Appl. Thrombosis/Hemostasis. 2012. |
|
|
Ozhan H, Aydin M, Yazici M, Yazgan O, Basar C, Gungor A, Onder E (2010). Mean platelet volume in patients with non-alcoholic fatty liver disease. Platelets 21(1):29-32. |
|
|
Peck-Radosavljevic M (2000). Thrombocytopenia in liver disease. Can. J. Gastroenterol. 14:60D-66D. Hematol. 50(3):173-178. |
|
|
Pereira J, Accatino L, Alfaro J, Brahm J, Hidalgo P, Mezzano D (1995). Platelet autoantibodies in patients with chronic liver disease. Am. J. |
|
|
Pinedo HM, Verheul HM, D'Amato RJ, Folkman J (1998). Involvement of platelets in tumour angiogenesis? Lancet 352(9142):1775-1777. |
|
|
Purnak T, Olmez S, Torun S, Efe C, Sayilir A, Ozaslan E, Tenlik I, Kalkan IH, Beyazit Y, Yuksel O (2013). Mean platelet volume is increased in chronic hepatitis C patients with advanced fibrosis. Clin. Res. Hepatol. Gastroenterol. 37(1):41-46. |
|
|
Rios R, Sangro B, Herrero I, Quiroga J, Prieto J (2005). The role of thrombopoietin in the thrombocytopenia of patients with liver cirrhosis. Am. J. Gastroenterol. 100(6):1311-1316. |
|
|
Sanjo A, Satoi J, Ohnishi A, Maruno J, Fukata M, Suzuki N (2003). Role of elevated platelet-associated immunoglobulin G and hypersplenism in thrombocytopenia of chronic liver diseases. J. Gastroenterol. Hepatol. 18(6):638-644. |
|
|
Stone RL, Nick AM, McNeish IA, Balkwill F, Han HD, Bottsford-Miller J, Rupaimoole R, Armaiz-Pena GN, Pecot CV, Coward J, Deavers MT (2012). Paraneoplastic thrombocytosis in ovarian cancer. N. Engl. J. Med. 366(7):610-618. |
|
|
Tahtaci M, Yurekli OT, Bolat AD, Balci S, Akin FE, Buyukasik NS, Ersoy O (2015). Increased mean platelet volume is related to histologic severity of primary biliary cirrhosis. Eur. J. Gastroenterol. Hepatol. 27(12):1382-1385. |
|
|
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2012). Global cancer statistics. CA Cancer J. Clin. 65(2):87-108. |
|
|
Ukropec JA, Hollinger MK, Salva SM, Woolkalis MJ (2000). SHP2 association with VE-cadherin complexes in human endothelial cells is regulated by thrombin. J. Biol. Chem. 275(8):5983-5986. |
|
|
Verheul HM, Jorna AS, Hoekman K, Broxterman HJ, Gebbink MF, Pinedo HM (2000). Vascular endothelial growth factor-stimulated endothelial cells promote adhesion and activation of platelets. Blood 96(13):4216-4221. |
|
|
Voutsadakis IA (2014). Thrombocytosis as a prognostic marker in gastrointestinal cancers. World J. Gastrointest. Oncol. 6(2):34-40. |
|
|
Wang CS, Yao WJ, Wang ST, Chang TT, Chou P (2004). Strong association of hepatitis C virus (HCV) infection and thrombocytopenia: implications from a survey of a community with hyperendemic HCV infection. Clin. Infect Dis. 39(6):790-796. |
|
|
Wartiovaara U, Salven P, Mikkola H, Lassila R, Kaukonen J, Joukov V, Orpana A, Ristimaki A, Heikinheimo M, Joensuu H, Alitalo K (1998). Peripheral blood platelets express VEGF-C and VEGF which are released during platelet activation. Thromb. Haemost. 80(1):171-175. |
|
|
Wong VW, Yu J, Cheng AS, Wong GL, Chan HY, Chu ES, Ng EK, Chan FK, Sung JJ, Chan HL (2009). High serum interleukinâ€6 level predicts future hepatocellular carcinoma development in patients with chronic hepatitis B. Int. J. cancer 124(12):2766-2770. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


