Full Length Research Paper
ABSTRACT
Cervical malignancy is still the leading cause of death for middle-aged women in the developing world. In Uganda, literature has shown that, cervical cancer incidence and death rates was 45.6 and 25 per 100,000 women respectively. However, the actual magnitude of cervical malignancy in Uganda might be higher since most of the cases are never reported. This study assessed the prevalence of cervical intraepithelial neoplasia among women from hospitals in Eastern Uganda. This was a longitudinal study, with follow-up until diagnosis of high-grade cervical intraepithelial neoplasia (CIN). One thousand and seventy seven women aged 15-55 years were recruited into the study. Pap-smear tests were conducted on all study participants. Women who had abnormal cytology were referred for immediate colposcopic and histological assessment. Surveillance was maintained on these women, and treatment postponed, until there was histological evidence of high-grade CIN (CIN2 or CIN3). At that point women were treated. Those that were pap smear negative were advised to return for screening for three consecutive negative smears before they were allowed to leave the study. Factors associated with cervical cancer were obtained by use of questionnaires. The general prevalence of CIN among women in Eastern Uganda was 416/1077 (38.6%). Two hundred and fourteen, 214/1077(19.9%) had severe CIN3, 180/1077(16.7%) had moderate CIN2, and 22/1077(2.0%) had mild CIN1. Older women aged 45-55-years were frequently diagnosed with the advanced disease stage as compared with young adults aged 15-24 who were less commonly diagnosed with the disease. The study showed that age, use of contraceptives, history of STI and HIV status had statistical significant association with development of cervical intraepithelial neoplasia among the studied participants. There is need for routine surveillance of precancerous lesions and treatment in a timely manner.
Key words: Cervical intraepithelial neoplasia, risk factors, cervical cancer.
INTRODUCTION
Cervical intraepithelial neoplasia is still a public health problem among women in less developed countries in the world (Banura et al., 2008; Ferlay et al., 2015). In the first world, like the United States, and Scandinavian countries, the decline in incidence and mortality has been well registered (Parkin et al., 2002, 2003; Forman et al., 2013; Ferlay et al., 2015), but this is not yet the case for developing nations, Sub-Saharan Africa. This is in part due to lack of information about the disease, and lack of screening services for detection of preinvasive and early invasive disease (de Oliveira et al., 2013; Bingham et al., 2003; Banura et al., 2008). Because of lack of efficient prevention and early detection services to complement treatment of the malignancy (Forman et al., 2013; Ferlay et al., 2015), over 200,000 deaths are reported annually in both developing and developed countries in the world (Ferlay et al., 2015). Estimates on cervical cancer incidence in 2012 showed that, Uganda had the highest age-standardized incidence rate in the world of 44.4/100,000, while East Africa had age-standardized rate (ASR) of 42.7/100,000, and the World had ASR of 14.0/100,000.It was further reported by WHO in 2014, that 3915 women in Uganda were positive for cervical cancer and that 2160 had died of the disease (ICO, 2016). Cervical cancer was documentedas the main cause of mortality among economically disadvantaged women of reproductive age in Uganda (Mutyaba et al., 2007).
Various agents in association with the cause of cervical intraepithelial neoplasia and cervical cancer development have been outlined. These include age at first intercourse (Camargo et al., 2011), circumcision (Cook et al.,1994; Deacon et al., 2000), history of sexually transmitted infections (STI) (Szaba and Short, 2000; Mosciki et al., 2001; Muñoz et al., 2004; Tobian et al., 2009), use of oral contraceptives (Muñoz et al., 2004; Baldwin and Jensen et al., 2013), infection with HIV (Stanley, 2010; Denny et al., 2012), and multiple sexual partners (Walker et al., 2002). The commonest risk factor is infection with human papillomavirus (HPV) (Banura et al.,2008).It has been estimated that, 33.6% of women in the Uganda are infected with human papillomavirus, and that 47.5 per 100,000 women every year develop cervical cancer (Bruni et al., 2014; Nakisige et al., 2017).Previous reports by Uganda Cancer registry from2003-2007 showed that, the prevalence of cervical cancer by histological type was as follows: squamous carcinoma, 22.7%, and Adeno carcinoma, 2.3%.Currently, there is no detailed data that outlines the burden of cervical intraepithelial neoplasia and associated factors among women in Eastern Uganda. Cervical cancer related studies that were previously conducted involved selected groups, and small numbers (Mukama et al., 2017), not sufficient enough to provide data on the burden of cervical intraepithelial neoplasia and its clinical presentations in the general population in Uganda. Yet this information is crucial and important to support the implementation of HPV vaccination and cervical cancer screening programs among women in Uganda (Ferlay et al., 2015). Because HPV vaccines do not protect against all types of HPV that cause cervical cancer, vaccinated persons may become infected with HPV types against which vaccines do not offer protection. For this reason, vaccinated persons should be encouraged to be screened for cervical cancer later in life according to national policies. Screening should continue to prevent cancer in both non-vaccinated women and vaccinated women to provide protection from oncogenic HPV types for which HPV vaccines do not offer protection (WHO, 2014). The current study was designed to serve as a national baseline data to support the implementation of HPV vaccination and to help in planning for cervical cancer screening programs in Uganda by estimating the burden of CIN, and associated factors among the studied population in Eastern Uganda, Uganda. Our study adopted the Standard World Health Organization cytologic nomenclature for condyloma and cervical intraepithelial neoplasia (CIN) grades 1-3 and Bethesda system for rating cytology using the nomenclature LSIL and HSIL (Mark et al., 2018; Canepa et al., 2019). According to the CIN histological classification system, lesions were graded primarily according to the proportion of the epithelium which was occupied by basaloid, undifferentiated cells (Mark et al., 2018; Canepa et al., 2019). CIN1or CIN grade 1 was when the upper two thirds of the epithelium showed good differentiation, although some nuclear abnormalities persisted up to the surface. CIN2 or CIN grade 2 was whenthe upper half of the epithelium showed differentiation and maturation, again when nuclear abnormalities (atypia) persisted to the surface. CIN3 or CIN grade 3 was whenthe maturation was confined to the superficial third of the epithelium, or nuclear abnormalities were marked throughout the whole thickness of the epithelium.
MATERIALS AND METHODS
Study area
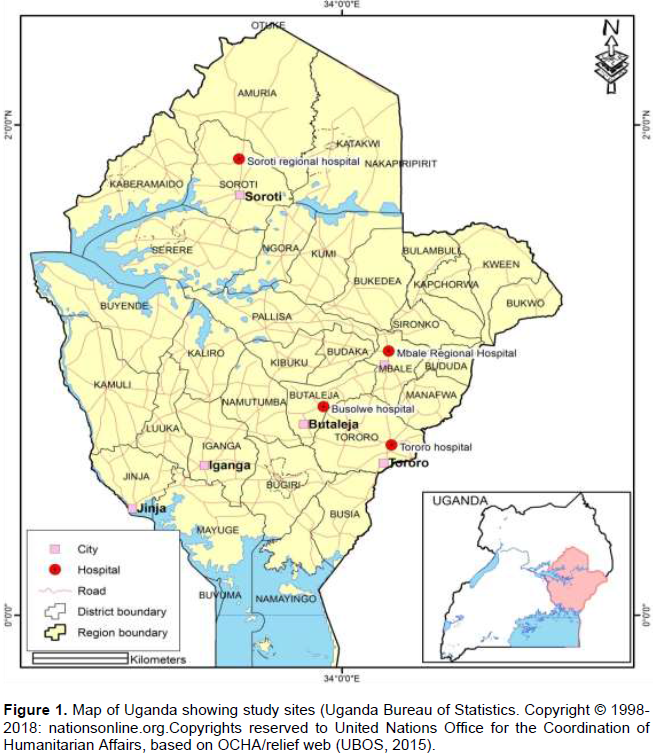
This study was conducted at selected regional referral hospitals in Eastern Uganda. These hospitals include; Tororo, Mbale, Butalejja, Kumi, and Soroti referral hospitals. Availability of established cancer screening facilities, trained oncologists and technologist in cancer diagnosis and treatment for both inpatients and outpatients within these hospitals, have turned them into referral centers for cervical cancer screening for the neighboring districts that lack these facilities. Districts like Moroto, Katakwi, Amuria, Kaberamaido, Ngora, Serere, Namalu, and Nakapiripirit with inadequate cancer screening units and oncologists entirely rely on these selected referral hospitals for all their diagnostic and treatment programs (Figure 1).
Study design
This is a longitudinal study, with follow-up until there was diagnosis of high-grade cervical intraepithelial neoplasia (CIN). A total of 1,077 women aged 15-55 years and seeking health services at the cancer screening health facilities of Mbale, Tororo, and Butalejja and Soroti referral hospitals in Eastern Uganda were invited to participate in the screening project after qualifying for inclusion criteria. The study protocol adopted in this study was with minor modifications of the method as previously described by Collins (2010) and all results were reported by using the Bethesda system for reporting cervical cytology and WHO dysplasia reporting system (Mark et al., 2018; Nayar et al., 2015; Singhal et al., 2018; Canepa et al., 2019). Follow-up of the study participants was in two main phases. Firstly, in the absence of cervical cytological abnormality, allow men were asked to return after six months for three consecutive negative smears before they were allowed to leave study, while women with inadequate smear were immediately requested to return for a repeat smear; secondly, in the presence of cervical cytological abnormality, all women who were referred for immediate colposcopy and histological examination. This was maintained for six months until there was no evidence of that abnormality. This was defined as three consecutive negative colposcopic assessments and three consecutive negative smears.
If another cervical cytological abnormality was detected; the same procedure would be applied. Finally, at the end of the follow-up, the study protocol called for treatment to be postponed in women detected with cervical cytological abnormality until there was histological evidence of CIN3, and then recalled later for treatment, and thereafter left the study. Factors associated with cervical Intraepithelial neoplasia were obtained by use of questionnaires. These factors included the study participants’ age at first intercourse, being circumcised, and history of sexually transmitted infections, usage of oral contraceptives, infection with HIV, and their sexual behavior if they had multiple sexual partners. After meeting with the patients, written informed consent was obtained and a brief oral questionnaire was administered.
Retention and follow-up of the studied participants
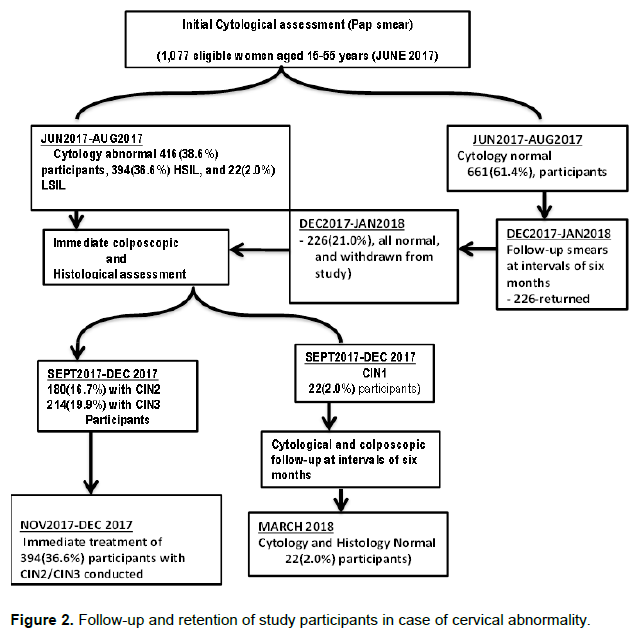
A total of 1,077 women aged 15-55 years and seeking health services at the cancer screening health facilities of Mbale, Tororo, and Butalejja and Soroti referral hospitals in Eastern Uganda were invited to participate in the screening project after qualifying for inclusion criteria. Follow up schedules were in months. Between June 2017- August 2017, 416/1,077(38.6%) women were detected with abnormal cytology, of which 394/1,077(36.6%) had HSIL, and 22/1077(2.0%) had LSIL. All were subjected for immediate colposcopy and histological assessment between September, 2017-Oct 2017; their histological assessment showed that, 180/1,077(16.7%) had moderate CIN2, and 214/1,077(19.9%) severe CIN3, while 22(2.0%) participants had mild CIN1.Between November 2017-December2017, 394 (36.6%) participants who had developed CIN2/CIN3 neoplasia were treated, and the participants who did not respond to treatment were asked to return for further review (Figure 2).
Inclusion and exclusion criteria
The study included all women aged between 15-55 years, who resided and attended Healthcare services at the hospitals in Eastern Uganda. The study also included all women who consented and were willing to comply with the stipulated follow-up schedule. The study excluded all women who were <15 and ≥ 55years. Also women in menstruation cycle were excluded because blood discharge during the menstrual cycle would interfere with visual activity of the cervix and would give false positive results. The study also excluded all women aged 15-55 years who failed to give their consent for the study
Sample collections from patients
Cytological samples
Cytological samples were collected by minor modifications of the method as previously described by Collins (2010). Two cytological samples were collected at each visit, using independent Ayres’s wooden spatula for each patient. The first sample was obtained by performing a 360º rotation of the transformation zone; the specimen collected was then applied to a slideto prepare a cervical smear for immediate cytological evaluation and reporting. The second sample was taken by performing a 360º rotation of the transformation zone as in the first sample collection. The spatula end was then broken-off into a 15-mL holding tubes containing 5 mL of PBS (pH 7.2), and then stored for future virological examination. Samples were kept temporarily at 4°C for an average of 6 h and then stored in a freezer at -20°C for further studies. All cervical cytological materials were examined and reported by our laboratory cytologist using the WHO dysplasia reporting system (Mark et al., 2018; Nayar et al., 2015; Singhal et al., 2018; Canepa et al., 2019).
Histological samples
Histological samples were collected by the method previously described by Collins (2010). Two histological specimens were taken. The first specimen was taken upon colposcopic evidence of abnormal epithelium by performing a punch biopsy for immediate histological examination; and the second histological specimen was taken from an area of abnormal epithelium, and stored for further histological studies. All cervical histological samples were examined and reported by our laboratory pathologist using original CIN terminology (Nayar et al., 2015; Canepa et al., 2019; Barut et al., 2015).
Quality assurance/quality control
There was strict monitoring of the quality and quantity of specimens, turnaround time, sample preparation and testing, decontamination, reagents and equipment, and reviewing test results and control using standard laboratory operation procedures of microbiologyby Cheesbroughet (2006).
Sample destruction plan
National Standard Operating Procedures (SOP) on health care waste management (Sapkota et al., 2014; Bessesen et al., 2015) was adopted and used for sample destruction and management after the study. All materials used in the assay, including reagents and specimens, were disposed of in a manner that would inactivate infectious agents. Solid wastes were autoclaved. Liquid wastes were treated with sodium hypochlorite to a final concentration of 1.0% (1:5 dilution of household bleach) and allowed 30 min for decontamination before disposal.
Ethical consideration
The ethical approval of the study was sought from Kampala International University (KIU), Mbarara University of Science and Technology (MUST) Institutional Research and Ethics Committee (IREC) on Human Research (Approval No. 06/01-17) and Uganda National Council for Science and Technology (Approval No. HS2246). All research protocols were performed in accordance with the ethical standards of the committees on human experimentation laid down in the Helsinki declaration of 1975 as revised in 2000. The participants were requested to sign the informed consent form before participating in the study. No participant was forced to participate in the study. Participants were coded instead of reflecting their real names. The participants were respected in relation to their right of their cultural beliefs and rights and were allowed to withdraw from the study without any condition. All research protocols were performed in accordance with the ethical standards of committees on human experimentation laid down in the Helsinki declaration of 1964 revised in WMA (2000).
Data management and statistical analyses
Data were analyzed by the use of descriptive statistics and regression using IBM SPSS version 20. Descriptive statistics was used to obtain socio-demographic characteristics of the study participants, histologic prevalence of cervical cancer and age-specific histologic prevalence of cervical cancer and disease stages during the screening period. The outcome of high grade cervical histological transformation was dichotomized as presence or absence of the cervical cancer and tested against suspected factors associated with high grade cervical histological transformation to assess for associations. Univariable analysis was used, and all the variables with a p ≤ 0.2 were entered into stepwise forward multiple logistic regression model. Interaction and confounding were assessed, and values of p ≤ 0.05 were regarded as statistically significant relationships.
RESULTS
Socio-demographic characteristics of participants
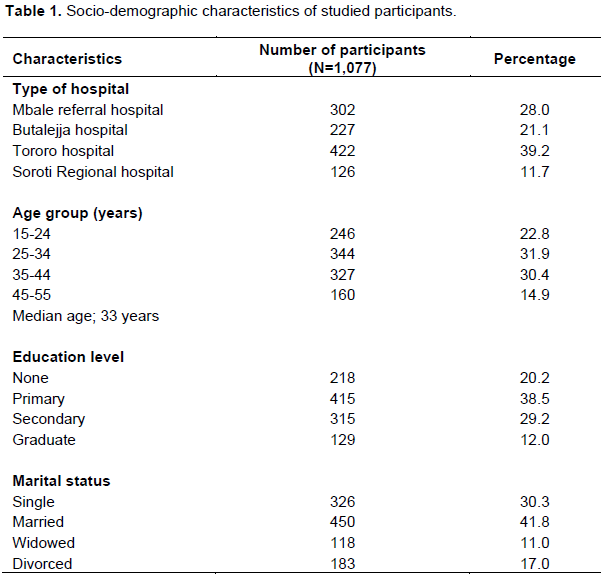
Study participants were classified in relation to the hospital type, age, educational level, and marital status. In relation to hospital types, Soroti Regional Hospital registered the least number of participants 126(11.7%), while Butalejja Hospital had 227(21.1%), Mbale Regional Hospital 302 (28.0%) and Tororo Hospital had the highest 422(39.2%).In relation to age, the participants with 45-55 years represented the lowest number,160(14.9%) compared with those having 25-35yearswith 344(31.9%) respectively. The median age of the study participants was 33 years with the median range of 15-55 years and interquartile range (IQR) = 14-36 years. In relation to the educational level, graduates had the lowest number 129(12.0%) compared to primary scholars with the highest 415(38%). In relation to marital status, the widowed participants were the least registered 118(11.0%), followed by divorced participants183 (17.0%), then singles 326(30.3%); the highest were married 450 (41.8%) (Table 1).
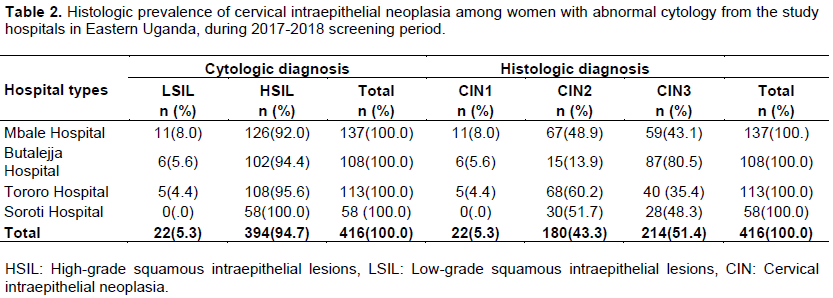
Histologic prevalence of cervical intraepithelial neoplasia among women with abnormal cytology from the study hospitals in Eastern Uganda, during 2017-2018 screening period
Four hundred and sixteen women were diagnosed with abnormalcytology; 22/416(5.3%) hadLSIL, and 394/416 (94.7%) had HSIL. Histological assessment was immediately performed and a punch biopsy was removed for histological examination. The results showed that 22/416(5.3%) had CIN1, 180/416(43.3%) moderate CIN2, and 214/416(51.4%) severe CIN3. Table 2 shows the cytological and histologic findings of women with cervical abnormalities within the respective study hospitals in Eastern Uganda.
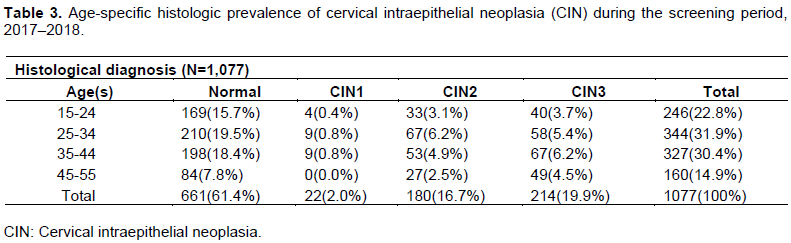
Age-specific histologic prevalence of cervical intraepithelial neoplasia during the screening period, 2017–2018
Cervical intraepithelial neoplasia (CIN) were graded according to the CIN histological classification system (modified, 1990).The lesions were graded primarily according to the proportion of the epithelium which was occupied by basaloid, undifferentiated cells (Mark et al., 2018; Canepa et al., 2019). Of the 1,077(100%) women who participated in the screening process, 661(61.4%) were histologically diagnosed with normal epithelium, while 22(2.0%) women were diagnosed with mild CIN1, 180(16.7%) with moderate CIN2, and 214(19.9%) with severe CIN3. Table 3 shows the comprehensive age-specific histologic prevalence of cervical intraepithelial neoplasia among the participants.
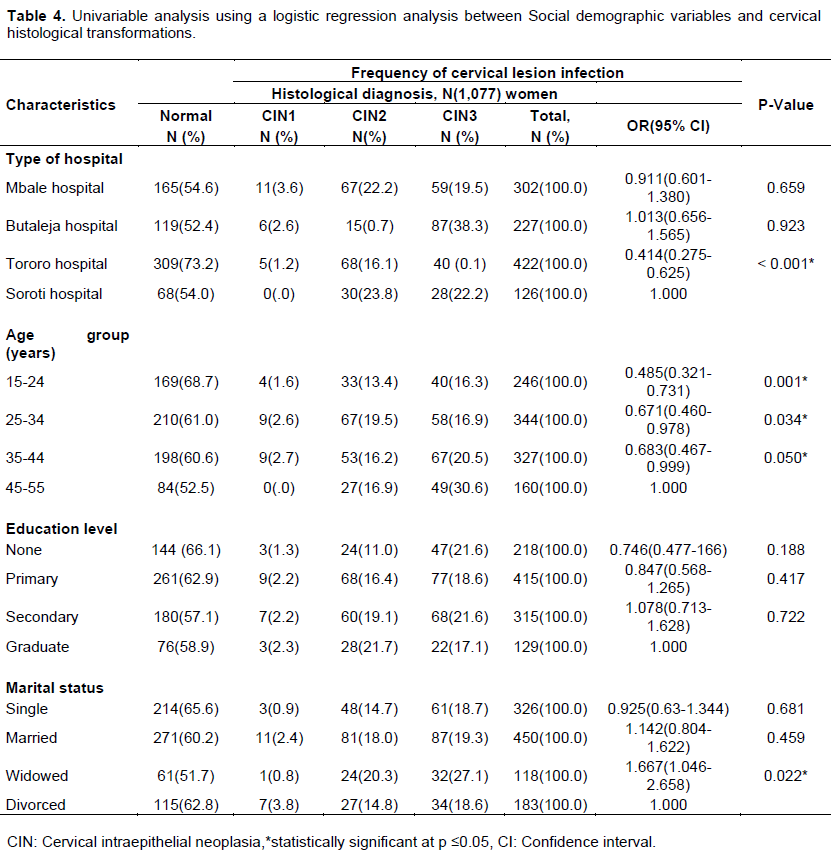
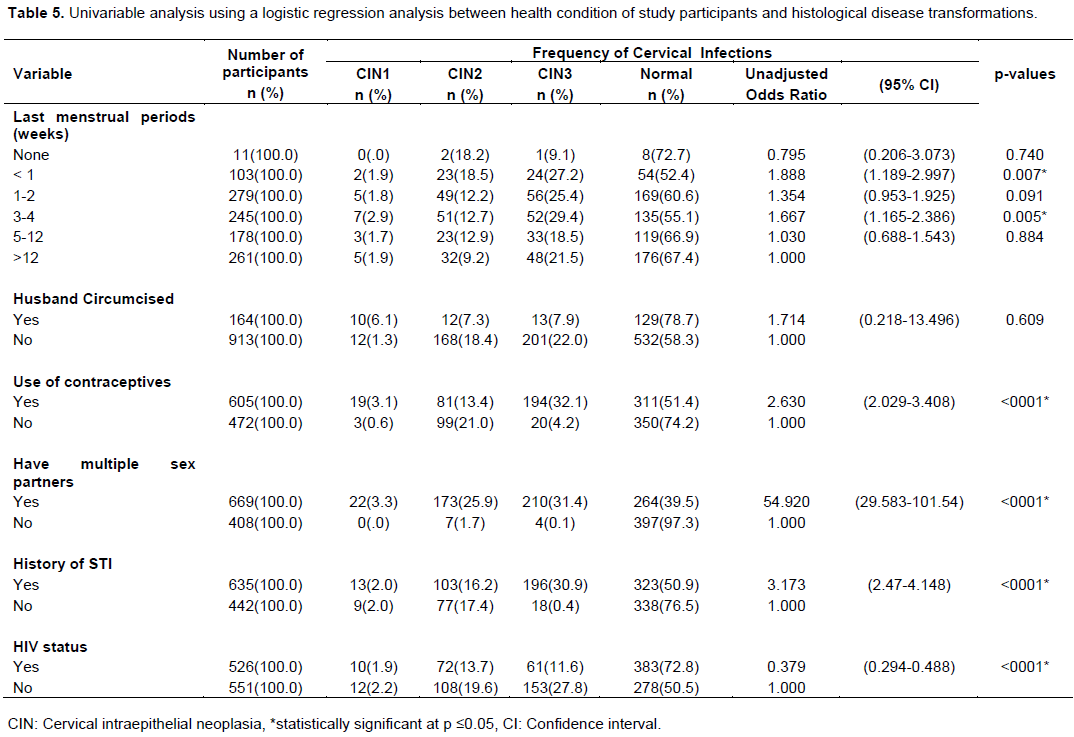
Univariable analysis between social demographic variables and cervical histological transformations in women from four selected hospitals in Eastern Uganda
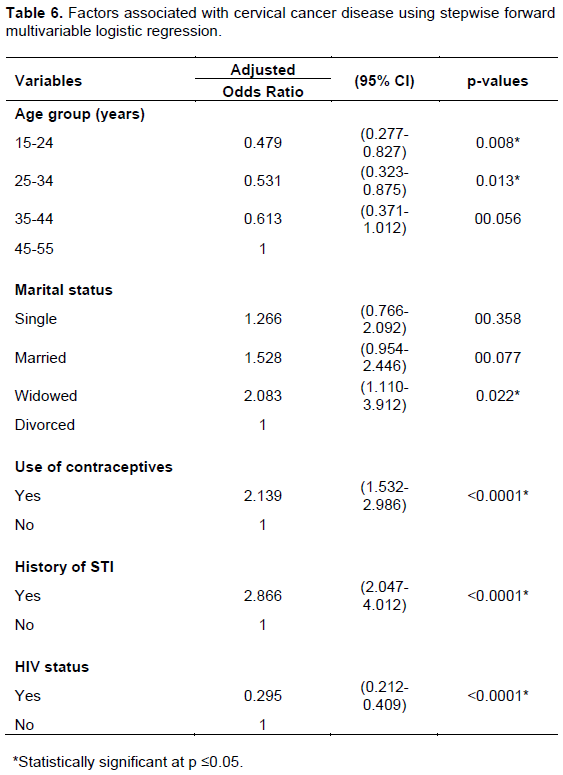
When the predictor variables for cervical histological transformation were subjected to univariable analysis using a logistic regression analysis, they had the following logistic regression values: Tororo Hospital (OR=0.414; 95% CI: 0.275-0.625; p < 0.05), age group 15-24 (OR=0.485; 95% CI: 0.321-0.731; p < 0.05), age group 25-34 (OR=0.671; 95% CI: 0.460-0.978; p < 0.05), age group 35-44 (OR=0.683; 95% CI: 0.467-0.999; p = 0.05), widowed (OR=1.667; 95% CI: 1.046-2.658; p < 0.05), last menstrual period <1-week (OR=1.888; 95% CI: 1.189-2.997; p < 0.05), last menstrual period 3-4 weeks (OR=1.667;95% CI: 1.165-2.386; p < 0.05 ), use of contraceptives (OR=2.630; 95% CI: 2.029-3.408; p < 0.05), multiple sex partners (OR=54.920; 95% CI: 29.583-101.54; p < 0.05), history of STI (OR= 3.173; 95% CI: 2.47-4.148; p < 0.05) and HIV (OR=0.379; 95% CI: 0.294-0.488, p < 0.05) were found to be statistically significant (p ≤ 0.05) with cervical histological transformation (Tables 4 and 5). When the univariate significant predictor variables for cervical histological transformations were subjected to multivariable regression analysis, they had the following logistic regression values: age 15-24 (OR=0.479; 95% CI: 0.277-0.827; p < 0.05), age group 25-34 (OR=0.531; 95% CI: 0.323-0.875; p < 0.05) widowed (OR=2.083; 95% CI: 1.110-3.912; p < 0.05), use of contraceptives (OR=2.139; 95% CI: 1.532-2.986; p < 0.05), history of STI (OR=2.866; 95% CI: 2.047-4.012; p < 0.05) and HIV (OR=0.295; 95% CI:0.212-0.409; p < 0.05) were found to have statistically significant relationships (p < 0.05) with high grade cervical histological transformation (Table 6).
DISCUSSION
This study determined the histologic prevalence, factors associated with cervical intraepithelial development (CIN), and their strength among women attending health-care services from selected referral hospitals in Eastern Uganda. The general prevalence of cervical intraepithelial neoplasia in this study was 38.6%. Younger age, marital status, history of STIs, usage of oral contraceptives, and HIV status were all risk factors for cervical intraepithelial neoplasia development. Our results were slightly higher than findings from other resource limited settings in sub-Saharan Africa in which a 4.8-14% prevalence of pre-cancer lesions was reported in Nigeria (Ludwig and Weinstein, 2005). This could have been due to the difference in the screening method used. Our study used Pap smear test method while the later used VIA test method. However, our study compared well with Santesso et al. (2016) who reported cervical intraepithelial neoplasia prevalence of 34% in Uganda, and with the clinical studies conducted in Uganda between 2006-2007 at Mulago Referral Hospital by Katahoire et al. (2007) who reported increase in bed occupancy from 30-63.5% by cervical cancer patients, of whom 80% were diagnosed with late stage disease. Furthermore, this findings are consistent with the current study in Eastern Uganda, in which a high prevalence of cervical intraepithelial lesions was registered in the studied hospitals; Mbale Hospital registered-11/167(8.0%) women with CIN1, 67/137 (48.9%) with CIN2, and 59/137 (43.1%) with CIN3; Butalejja Hospital had 6/108(5.6%) women with CIN1, l5/108 (13.9%) women with CIN2, and 87/108(80.5%) with CIN3; Tororo Hospital registered -5/113-(4.4%) women with CIN1, 68/113 (60.2%) women with CIN2, and 40/113 (35.4%) with CIN3; Soroti Hospital registered 0/58(.0%) with CIN1,30/58 (51.7%) women with CIN2, and 28/58 (48.3%) with CIN3. Previous hospital based studies conducted at Mulago Hospital by Wabinga et al. (2000) and Mutyaba et al. (2006) also showed that cervical intra epithelial neoplasia was the most common malignancy among women in Uganda accounting for 40% of all genital tract cancers and for 8% of all malignancies. In other studies, Wabinga et al. (2014) reported a prevalence of 22% in Uganda, 25.8% in East Africa, and 15.1% in the world, and the age-standardized incidence rates were 44.4% in Uganda, 42.2% in East Africa, and 14% in the world. This ranked Uganda as the 14th country with the highest cervical cancer incidence in the world (Ndejjo et al., 2016). Our current study reported a general prevalence of 38.6% which is higher than 17.1% prevalence reported by Wabinga et al. (2014), and Forman et al. (2013) at Kyandondo County in Kampala in Uganda. The high prevalence was probably because of the difference in sample size and screening methods used in our study. Unfortunately, screening in Uganda is erratic, opportunistic, and in some places absent due to a lack of resources or lack financial commitment. This translates to a staggeringly low screening uptake of about 4.8% in rural Uganda (Ndejjo et al., 2016). However, our study compared well with the earlier reports from Harare (Chokunonga et al., 2013), which reported high age-standardized incidence rates of 55.0 per 100,000 and 45 per100, 000. Cervical intraepithelial neoplasia still accounts for 40% of all cancers in Uganda (Mitchell et al., 2017). However, the actual magnitude of cervical intraepithelial neoplasia and cervical cancer prevalence might be higher since most of the cases are never reported or registered.
In the current study, cytological and histological findings showed that, women who were diagnosed with HSIL were at an increased risk of developing CIN. Of the 416/1077(38.6%) women who were diagnosed with CIN, 22/1,077(2.0%) had mild CIN1, 180/1,077(16.7%) had moderate CIN2, and 214/1,077(19.9%) had severe CIN3. Older women aged 45-55years were frequently diagnosed with the advanced disease stage; as compared to sexually young adults aged 15-24 who were less commonly diagnosed with the late disease stage. Older women were less often diagnosed at early stage of cervical cancer compared to younger women. This may be due to lack of seeking obstetrics and gynecological medical care in post-menopausal period, particularly for women who live in rural areas where health care services are difficult to access. Another likely factor could be lack of awareness about their susceptibility to cervical cancer (Abotchie and Shokar, 2009; Kharbanda et al., 2015; Mitchell et al., 2017). In line with our study, are qualitative studies conducted in India, South Africa and Uganda which found out that older women who were of low socio economic status and unemployed, were less likely to participate in cervical cancer screening (Bradley et al., 2004; Kaku et al., 2008).
According to Muñoz et al. (2004), and Sankaranarayanan et al. (2004), long-term use of oral hormonal contraception has also been associated with an increased risk of cervical cancer and its precursors, but it has not been evident in all studies (Bertram, 2004; Bhatla et al., 2018). Our study demonstrated that there was an increased risk for cervical intraepithelial neoplasia in women who had used oral hormonal contraception method with ORs of 2.139 (p<0.001). The study indicated that usage of oral contraceptives increased the risk of developing cervical intraepithelial neoplasia.
Out of605/1077(56.2%) women who consented to having used oral hormonal contraceptives, 81/605(13.4) were diagnosed with CIN2, and 194/605(32.1) with CIN3 as opposed to 472/1077(43.8) who did not use oral contraceptive method in which 99/472(21.0 women were diagnosed with CIN2 and 20/472(4.2) with CIN3.This trend confirmed previous work in the region (Banura et al.,2008) which showed that prolonged usage of oral hormonal contraception method contributed to an increased risk of cervical intraepithelial neoplasia development with an adjusted OR of 3.15 [95%CI;1.62-6.13, p=0.001] among women in central Uganda.
In the current study, there was no significant risk for CIN in women who had circumcised sexual male partners with unadjusted ORs of 1.714(p<0.609). Out 164/1077(15.2) women who had circumcised male partners only 12/164(7.3) women were diagnosed withCIN2, and 13/164(7.9) with CIN3 in contrast to913/1077(84.8) women who had un-circumcised male partners in which 168/913(18.4) were diagnosed with CIN2 and 201/913(22.0) with CIN3 respectively. The study demonstrated that women who had circumcised partners were at a lower risk of developing cervical abnormalities than women with uncircumcised sexual partners. Indeed, our findings are in line with other studies (Cook et al., 1994) which showed that, male circumcision was associated with the prevention of common sexually transmitted diseases. Furthermore, data analysis from International Agency for Research on Cancer (IARC) established that circumcised men not only had substantial lower risk of penile HPV infections than uncircumcised men, but also that their partners had a lower risk of HPV infections and a lower risk of developing cervical cancer (Wideroff and Haderer, 1999).The protective effect was more pronounced among women whose male partners engaged in high-risk sexual behaviors. Further evidence of the protective effect comes from two resent randomized controlled trials. One trial showed that circumcision of adolescent boys and men in a rural Uganda population had reduced HPV prevalence by 35% (Tobian et al., 2009).
The present study also showed that, there was an increased risk for CIN development in women who had history of STI’S with ORs of 2.866 (p<0.001). Out of 635/1077 (60.0) women who had history of STI’S,103/635(16.2) were diagnosed with CIN2, and 196/635 (30.9) with CIN3 respectively. Our findings are in agreement with other studies by Mosciski et al. (2001)who showed that, cervical infections with STI’S such as chlamydia trachomatis and HIV may increase susceptibility to cervical cancer development by inflammation or micro abrasions of the epithelium resulting from sexual intercourse. This may allow direct access to basal epithelium cell. It is possible that STI’S could enhance the oncogenic effect of an already established HPV infection by influencing local response (Schmuz et al., 1989).
Last but not the least, cervical intraepithelial neoplasia has long been associated with HIV infection, and in fact, it was added as an AIDS-defining illness to early AIDS case definitions by the CDC. In the present study, women who were HIV positive had an increased risk of CIN development with ORs of 0.295(p<0.001). As women with HIV have a higher frequency of HPV coinfections, rates of pre-cancer and cancer are typically higher. Previous studies in sub-Saharan Africa have demonstrated a consistent association of cervical cancer and HIV in Senegal (Holmes et al., 2009); South Africa, Zimbabwe (Moodley, 2006); and also in other low-and middle income countries (Forhan et al., 2015).
CONCLUSION
This study showed that the prevalence of cervical intraepithelial neoplasia infections was high in the studied population of women in Eastern Uganda. Age at first intercourse, multiple sexual partners, Infection with HIV, long-term use of oral contraceptives, and cervical infections with STI had statistically significant associations with high grade of cervical intraepithelial neoplasia development. There is need for effective and affordable screening methods for early detection of precancerous lesions and treatment in poor resource setting
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abotchie PN, Shokar NK (2009). Cervical cancer screening among college students in Ghana.Knowledge and health beliefs. International Journal of Gynecologic Cancer 19:412-416, 128. |
|
|
Baldwin MK, Jensen JT (2013). Contraception during the perimenopause. Maturitas 76(3):235-242. |
|
|
Banura C, Franceschi S, van Doorn LJ (2008). Prevalence, incidence and clearance of human papillomavirus infection among young primiparous pregnant women in Kampala Uganda. International Journal of Cancer 123:2180-2187. |
|
|
Barut MU, Kale A, KuyumcuoÄŸlu U, Bozkurt M, AÄŸaçayak E, Özekinci S, Gul T (2015). Analysis of sensitivity, specificity, and positive and negative predictive values of smear and colposcopy in diagnosis of premalignant and malignant cervical lesions. Medical science monitor. International Medical Journal of Experimental and Clinical Research 21:3860. |
|
|
Bertram CC (2004). Evidence for practice: oral contraception and risk of cervical cancer. Journal of the American Academy of Nurse Practitioners 16(10):455-461. |
|
|
Bessesen MT, Adams JC, Radonovich L, Anderson J (2015). Disinfection of reusable elastomeric respirators by health care workers.A feasibility study and development of standard operating procedures. American Journal of Infection Control 43(6):629-634. |
|
|
Bhatla N, Aoki D, Sharma DN, Sankaranarayanan R (2018). Cancer of the cervix uteri. International Journal of Gynecology and Obstetrics 143:22-36. |
|
|
Bingham A, Bishop A, Coffey P, Winkler J, Bradley J, Dzuba I, Agurto I (2003). Factors affecting utilization of cervical cancer prevention services in low-resource settings. SaludPublicaMex 3:S408-416. |
|
|
Bradley CJ, Given CW, Roberts C (2004).Health care disparities and cervical cancer. American Journal of Public Health 94(12):2098-2103. |
|
|
Bruni L, Barrionuevo-Rosas L, Serrano B, Brotons M, Cosano R, Muñoz J, Bosch FX, de Sanjosé S, Castellsagué X (2014). Human papillomavirus and related diseases in Uganda.Summary report 2014.HPV Information Centre. |
|
|
Camargo M, Soto-De Leon DC, Sanchez R, Perez-Prados A, Patarroyo ME, Patarroyo MA (2011). Frequency of human papillomavirus infection, coinfection, and association with different risk factors in Colombia. Annals of Epidemiology 21:204-213. |
|
|
Canepa M, Patel NR, Garcia-Moliner ML (2019).Pathology and Molecular Diagnosis of Cervical Cancer and Precursor Lesions.Uterine Cervical Cancer. Clinical and Therapeutic Perspectives 61:87. |
|
|
Cheesbrough M. (2006). District laboratory practice in tropical countries. Cambridge University Press 60:64. |
|
|
Chokunonga E, Levy LM, Bassett MT (2013).Zimbabwe National cancer registry.2010 Annual Report. Harare. |
|
|
Collins SI (2010). An investigation of the natural history of early cervical human papillomavirus infection and its relationship to the acquisition of epithelial abnormalities of the cervix (Doctoral dissertation, University of Birmingham). |
|
|
Cook LS, Koutsky LA, Holmes KK (1994).Circumcision and sexually transmitted diseases. American Journal of Public Health 84(2):197-201. |
|
|
Deacon JM, Evans CD, Yule R, Desai M, Binns W, Taylor C, Peto J (2000).Sexual behaviour and smoking as determinants of cervical HPV infection and of CIN3 among those infected. British journal of Cancer 83(11): 1565-72. |
|
|
Denny LA, Franceschi S, de Sanjose S, Heard I, Moscicki AB, and Palefsky J (2012). Human papillomavirus, human immunodeficiency virus and Immunosuppression. Vaccine 5:168-74. |
|
|
de Oliveira CM, Fregnani JH, Carvalho JP, Longatto-Filho A, Levi JE (2013). Human papillomavirus genotypes distribution in 175 invasive cervical cancer cases from Brazil. BMC Cancer 13:357. |
|
|
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Bray F (2015). Cancer incidence and mortality worldwide. International Journal of Cancer 136(5):359-386. |
|
|
Forhan SE, Godfrey CC, Watts DH, Langley CL (2015). A Systematic Review of the Effects of Visual Inspection with Acetic Acid, Cryotherapy, and Loop Electrosurgical Excision Procedures for Cervical Dysplasia in HIV-Infected Women in Low- and Middle-Income Countries. Journal of Acquired Immune Deficiency Syndromes (1):350-356. |
|
|
Forman D, Bray F, Brewster DH, Gombe Mbalawa C, Kohler B, Piñeros M, Steliarova-Foucher E, Swaminathan R, and Ferlay J (2013). Cancer Incidence in Five Continents Volume X. IARC Scientific Publication No. 164. |
|
|
Holmes RS, Hawes SE, Touré P, Dem A, Feng Q, Weiss NS, Kiviat NB (2009). HIV Infection as a Risk Factor for Cervical Cancer and Cervical Intraepithelial Neoplasia in Senegal. Cancer Epidemiology, Biomarkers and Prevention 18(9):2442-2446. |
|
|
ICO Information Centre on HPV and Cancer (HPV Information Centre) (2016). Human Papillomavirus and Related Diseases Report: Uganda [Internet]. 2016. |
|
|
Kaku M, Mathew A, Rajan B (2008). Impact of socio-economic factors in delayed reporting and late-stage presentation among patients with cervix cancer in a major cancer hospital in South India. Asian Pacific Journal of Cancer Prevention 9(4):589-594. |
|
|
Katahoire AR, Jetta J, Arube-Wani J, Kivumb G, Murokora D, Siu G,Arinaitwe L, Lyazi I (2007). Formative research report, An assessment of thereadiness for introduction of a cervical cancer vaccine in Uganda. Kampala, Child Health and Development Centre, Makerere University, 2008PATH. |
|
|
Ludwig JA, Weinstein JN (2005). Biomarkers in cancer staging, prognosis and treatment selection. Nature Reviews Cancer5 (11):845. |
|
|
Mark J, Morrell K, Alfiero A, Frederick PJ (2018). Expert Review of Cervical Cytology. Journal of Lower Genital Tract Disease 22(2):120-122. |
|
|
Mitchell SM, Pedersen HN, Sekikubo M, Moses E, Mwesigwa D (2017). Self-collection based HPV testing for cervical cancer screening among women living with HIV in Uganda. A descriptive analysis of knowledge intentions to screen and factors associated with HPV positivity. BMC Womens Health 17(1):4. |
|
|
Moodley JR (2006). HIV and pre-neoplastic and neoplastic lesions of the cervix in South Africa: a case-control study. BMC Cancer 6:135. |
|
|
Mosciki A, Hill N, Powel K (2001). Risk for incident human papillomavirus infection and low-grade squamous intraepithelial lesions development in young females.JAMA 285:2995-3002. |
|
|
Mukama T, Ndejjo R, Musabyimana A, Halage AA,Musoke D (2017). Women's knowledge and attitudes towards cervical cancer prevention: a cross sectional study in Eastern Uganda. BMC Women's Health17(1):9. |
|
|
Muñoz N, Bosch FX, Castellsagué X (2004). Against which human papillomavirus types shall we vaccinate and screen? The international perspective. International Journal of Cancer 111:278-285. |
|
|
Mutyaba T, Faxelid E, Mirembe F, Weiderpass E (2007). Influences on uptake of reproductive health services in Nsangi community of Uganda and their implications for cervical cancer screening. Reproductive Health 4:4. |
|
|
Mutyaba T, Mmiro FA, Weiderpass E (2006). Knowledge, attitudes and practices on cervical cancer screening among the medical workers of Mulago Hospital, Uganda. BMC Medical Education 6(1):13. |
|
|
Nakisige C, Melissa S, Anthony ON (2017). Cervical cancer screening and treatment in Uganda. Gynecologic Oncology Reports 20:37-40. |
|
|
Nayar R, Wilbur DC (2015). The Bethesda system for reporting cervical cytology.definitions, criteria, and explanatory notes. Springer. |
|
|
Ndejjo R, Mukama T, Musabyimnana A, Musoke D (2016). Uptake of cervical cancer screening and associated factors among women in rural Uganda. PLoS ONE 11(2):0149696. |
|
|
Parkin DM, Ferlay J, Hamdi-Cherif M (2003). Cancer in Africa: epidemiology and prevention. Lyon: IARC Press. |
|
|
Parkin DM, Whelan SL, Ferlay J, Teppo L, Thomas DB (2002). Cancer Incidence in Five Continents, Vol. VIII. IARC Scientific Publications No. 155, Lyon, IARC. |
|
|
Sankaranarayanan R, Basu P, Wesley RS, Mahe C, Keita N, Mbalawa CG. Nayama M (2004). Accuracy of visual screening for cervical neoplasia: Results from an IARC multi-center study in India and Africa. International Journal of Cancer 110(6):907-913. |
|
|
Santesso N, Mustafa RA, Schünemann HJ, Arbyn M, Blumenthal PD, Cain J, Forhan SE (2016). World Health Organization Guidelines for treatment of cervical intraepithelial neoplasia 2-3 and screenâ€andâ€treat strategies to prevent cervical cancer. International Journal of Gynecology and Obstetrics 132(3):252-258. |
|
|
Sapkota B, Gupta GK, Mainali D (2014). Impact of intervention on healthcare waste management practices in a tertiary care governmental hospital of Nepal. BMC Public Health 14(1):1005. |
|
|
Schmuz R, Okong P, deVilliers EM (1989). Multiple infections in case of cervical cancer for high incidence area in tropical Africa. International Journal of Cáncer 43:805-9. |
|
|
Singhal U, Lamba S, Kumar U, Nanda A (2018). Pattern of Epithelial Cell Abnormalities On Cervical Papanicolaou Smears In Hospital Of North India. Annals of Pathology and Laboratory Medicine 5(3):A250-255. |
|
|
Stanley M (2010). Pathology and epidemiology of HPV infection in females. Gynecologic Oncology 117(2):5-10. |
|
|
Szaba R, Short RV (2000). How does circumcision protect against HIV infections? British Medical Journal10; 320(7249):1592-4 |
|
|
Tobian A, Serwadda D, Quin TC (2009). Male circumcision for prevention of HSV-2 and HPV infections and Syphilis. New England Journal of Medicine 360:1298-309. |
|
|
Uganda Bureau of Statistics (UBOS), Health planning in Uganda (2015).Carey RB, Bhattacharyya, S, Kehl SC, Matukas LM, Pentella MA, Salfinger M, Schuetz AN (2018).Implementing a quality management system in the medical microbiology laboratory. Clinical Microbiology Reviews 31(3):62-17. |
|
|
Wabinga HR, Nambooze S, Amulen PM, Okello C, Mbus L,Parkin DM (2014). Trends in the incidence of cancer in Kampala, Uganda 1991-2010. International Journal of Cancer 135(2):432-439. |
|
|
Wabinga HR, Parkin DM, Wabwire-Mangen F, Nambooze S (2000).Trends in cancer incidence in Kyadondo County, Uganda, 1960-1997. British Journal of Cancer 82(9):1585. |
|
|
Walker ARP, Michelow PM, Walker BF (2002).Cervix cancer in African women in Durban, South Africa. International Journal Gynecology and Obstetrics 79:45-46. |
|
|
World Health Organization (WHO) (2014). Cervical cancer, human papillomavirus (HPV), and HPV vaccines: key points for policy-makers and health professionals. Geneva: WHO 2007. [21 November 2014]. |
|
|
Wideroff SM, Haderer P (1999). Seroreactivity to human papillomavirus type, 16, 18, 31 and 45 virus-like particles in a case control study of cervical squamous intraepithelial lesions. Journal of Infectious Diseases 180:1424-28. |
|
|
Kharbanda P, Singh DK, Anand R, Singh A (2015). Study of awareness amongst women in rural and urban areas about early detection of cervical cancer by Pap smear. Indian Journal of Pathology ad Oncology 2(4):219-29. |
|
|
WMA (2000). World Medical Association Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects, (e52ndWMA General Assembly, Edinburgh, Scotland, 2000. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


