Full Length Research Paper
ABSTRACT
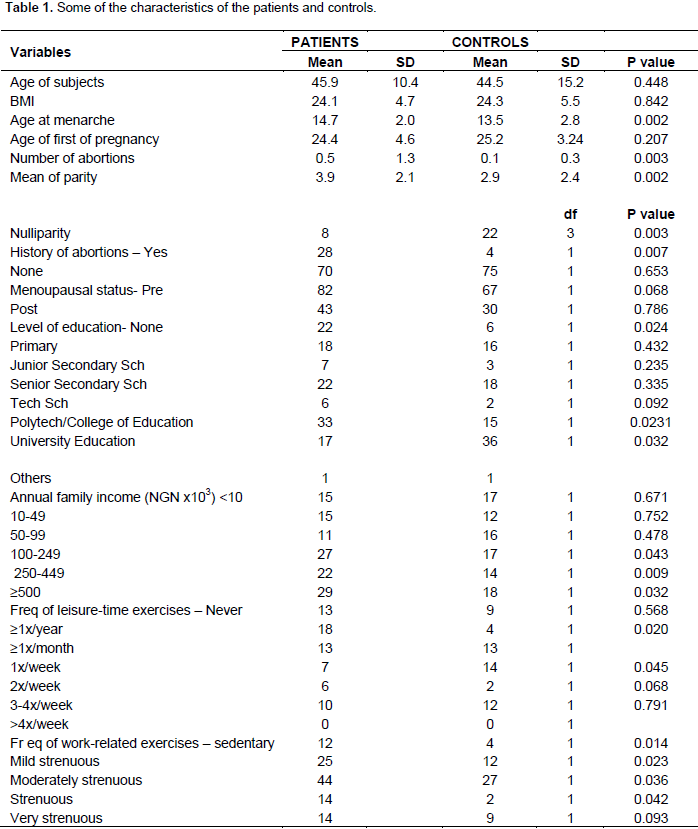
The aetiopathogenesis of cancer has been linked to life behaviour in a significant percentage of cases. Overweight, sedentary lifestyle, smoking and the excessive use of alcohol have been shown to play important roles. This study is aimed at determining the effect of life behavioural patterns and diets in the incidence of breast cancer in Nigerians population. A prospective case-controlled study of 125 breast cancer patients and 89 normal were recruited in Obafemi Awolowo University Teaching Hospital Complex, (OAUTHC), Ile-Ife, Nigeria. Questionnaire was administered to determine life behavioural patterns and nutritional habits. The variables on nutrition items were pooled to form 23 aggregate variables renamed “total variables” and exposure to endogenous estrogens was calculated. The means age in the patient and control groups were 45.9±10.4 and 44.5±15.2 years, respectively. A significantly higher number of patients in the breast cancer group had at least one previous abortion compared to the control group. The two groups have similar contraceptive use history and mean body mass index (BMI). 14 derived variables on univariate analysis were found to be significant, but only four (menarche [p = 0.002], “total beans” [p = 0.003], “total oils” [p = 0.021] and alcohol intake [p = 0.034]) reached statistical significance when subjected to multivariate regression analysis. Most were premenopausal but onsets of menarche were significantly higher among breast cancer patients. The onset of menarche, intake of beans, oils and alcohol may play a role in the incidence of breast cancer.
Key words: Life behaviour, diet, physical activities, breast cancer among women, Nigeria.
INTRODUCTION
MATERIALS AND METHODS
RESULTS




DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
ACKNOWLEDGEMENTS
REFERENCES
|
Adesunkanmi ARK, Lawal OO, Adelusola KA, Durosimi MA (2006). The severity, outcome and challenges of breast cancer in Nigeria. The Breast 15(3):399-409. |
|
|
Anand P, Kunnumakara AB, Sundaram C, Harikumar KB, Tharakan ST, Lai OS, Sung B, Aggarwal BB (2008). Cancer is a Preventable Disease that Requires Major Lifestyle Changes. Pharm. Res. 25(9):2097-2116. |
|
|
Anderson C, Harrigan C, George SM, Ferrucci LM, Sanft T, Irwin ML, Cartmel B (2016). Changes in diet quality in a randomized weight loss trial in breast cancer survivors: The lifestyle, exercise, and nutrition (LEAN) study. Nature Partner J. (npj) Breast Cancer 2:16026 |
|
|
Boyd NF, Greenberg C, Lockwood G, Little L, Martin L, Tritchler D, Byng J, Yaffe M (1997). Effects at two years of a low-fat, high-carbohydrate diet on radiologic features of the breast: results from a randomized trial. Canadian Diet and Breast Cancer Prevention Study Group. J. Natl. Cancer Inst. 89:488-496. |
|
|
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003). Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N. Engl. J. Med. 348:1625-1638. |
|
|
Cassidy A, Bingham S, Carlson J, Setchell KDR (1993). Biological effects of plant oestrogens in premenopausal women. FASEB J. 7:A866. |
|
|
Catsburg C, Kim RS, Kirsh VA, Soskolne CL, Kreiger N, Rohan TE (2015). Dietary patterns and breast cancer risk: A study in 2 cohorts. Am. J. Clin. Nutr. 101(4):817-823. |
|
|
Cerhan JR, Chiu BC, Wallace RB, Lemke JH, Lynch CF, Tomer JC, Rubenstein LM (1998). Physical activity, physical function, and the risk of breast cancer in a prospective study among elderly women. J. Gerontol. A Biol. Sci. Med. Sci. 53(4):M251-M256. |
|
|
Chang YJ, Hou YC, Chen LJ, Wu JH, Wu CC, Chang YJ, Chung KP (2017). Is vegetarian diet associated with a lower risk of breast cancer in Taiwanese women?. BMC public health, 17(1):800. |
|
|
Cohen LA (2000). Re: Meta-analysis: dietary fat intake, serum estrogen levels, and the risk of breast cancer. J. Natl. Cancer Inst. 92(1):78-78. |
|
|
Collaborative Gropu on Hormonal Factors in Breast Cancer (2002). Alcohol, tobacco and breast cancer- collaborative reanalysis of individual data from 53 epidemio- logical studies, including 58,515 women with breast cancer and 95,067 women without the disease. Br. J. Cancer. 87:1234-45. |
|
|
Demark-Wahnefried W, Peterson BL, Winer EP, Marks L, Aziz N, Marcom PK, Blackwell K, Rimer BK (2001). Changes in weight, body composition, and factors influencing energy balance among premenopausal breast cancer patients receiving adjuvant chemotherapy. J. Clin. Oncol. 19(9):2381-2389. |
|
|
Dirx MJ, Voorrips LE, Goldbohm RA et al (2001). Baseline recreational physical activity, history of sports participation, and postmenopausal breast carcinoma risk in the Netherlands Cohort Study. Cancer 92(6):1638-1649. |
|
|
Dorgan JF, Sowell A, Swanson CA, Potischman N, Miller R, Schussler N, Stephenson H (1998). Relationships of serum carotenoids, retinol, alpha-tocopherol, and selenium with breast cancer risk: results from a prospective study in Columbia, Missouri (United States). Cancer Causes Control 9:89-97. |
|
|
Egnell M, Fassier P, Lécuyer L, Zelek L, Vasson MP, Hercberg S, Latino-Martel P, Galan P, Deschasaux M, Touvier M (2017). B-Vitamin Intake from Diet and Supplements and Breast Cancer Risk in Middle-Aged Women: Results from the Prospective NutriNet-Santé Cohort. Nutrients 9(5):488. |
|
|
Ferrini K, Ghelfi F, Mannucci R, Titta L (2015). Lifestyle, nutrition and breast cancer: facts and presumptions for consideration. Ecancermedicalscience. 9:557. |
|
|
Friedenreich CM (2001). Review of anthropometric factors and breast cancer risk. Eur. J. Cancer Prev.10:15-32. |
|
|
Greenwald P (2002). Cancer prevention clinical trials. J. Clin. Oncol. 20(suppl 18):14S-22S. |
|
|
Herman C, Adlercreutz T, Goldin BR, Gorbach SL, Höckerstedt KA, Watanabe S, Hämäläinen EK, Markkanen MH, Mäkelä TH, Wähälä KT, Hase TA (1995). Soybean phytoestrogen intake and cancer risk. J. Nutr. 125(suppl 3):757S-770S. |
|
|
Holmberg L, Norden T, Lindgren A, Wide L, Degerman M, Adami HO (2001). Pre-operative oestradiol levels-relation to survival in breast cancer. Eur. J. Surg. Oncol. 27:152. |
|
|
Holmes MD, Chen WY, Feskanich D, Kroenke CH, Colditz, GA (2005). Physical Activity and Survival After Breast Cancer Diagnosis. JAMA. 293(20):2479-2486. |
|
|
Hu FB (2002). Dietary pattern Analysis: A new direction in nutritional epidemiology. Curr. Opin. lipidol. 13(1):3-9. |
|
|
Hulka BS (1996). Epidemiology of susceptibility to breast cancer. Prog. Clin. Biol. Res. 395:159-174. |
|
|
Hultén K, Van Kappel AL, Winkvist A, Kaaks R, Hallmans G, Lenner P, Riboli E (2001). Carotenoids, alpha-tocopherols, and retinol in plasma and breast cancer risk in northern Sweden. Cancer Causes Control 12(6):529-537. |
|
|
Hunter DJ, Manson JE, Coldzt GA, Stamper ME, Rosner B, Hennekens CH, Speiser FE, Willet WC (1993). A prospective study of intake of vitamin C, E and A and the risk of breast cancer. New Engl. J. Med. 329:234-40. |
|
|
IARC Working Group on the Evaluation of Cancer-Preventive Agents (2002). Weight Control and Physical Activity, IARC Handbooks of Cancer Prevention, Volume 6. Lyon, France: IARC. |
|
|
Jones JL, Daley BJ, Enderson BL, Jin-Rong Z (2002). Genistein inhibits tamoxifen effects on cell proliferation and cell cycle arrect in T47D breast cancer cells/Discussion. Am. Surg. 68(6):575-577. |
|
|
Ju YH, Doerge DR, Allred KF, Allred CD, Helferich WG (2002). Dietary genistein negates the inhibitory effect of tamoxifen on growth of estrogen-dependent human breast cancer (MCF-7) cells implanted in athymic mice. Cancer Res. 62(9):2474-2477. |
|
|
Key T, Appleby P, Barnes I, Reeves G (2002). Endogenous sex hormones and breast cancer in postmenopausal women: reanalysis of nine prospective studies. J. Natl. Cancer Inst. 94:606-616. |
|
|
Kumle M, Weiderpass E, Braaten T, Persson I, Adami HO, Lund E (2002). Use of oral contraceptives and breast cancer risk. Cancer Epidemiol. Prev. Biomarkers 11(11): 1375-1381. |
|
|
Lelièvre SA, Weaver CM (2013). Global Nutrition Research: Nutrition and Breast Cancer Prevention as a Model. Nutr. Rev. 71(11): 742-752. |
|
|
Longnecker MP, Newcomb PA, Mittendorf R, Greenberg ER (1988). Risk of breast cancer in relation to lifetime alcohol consumption. Int. J. Epidemiol. 17:298-306 |
|
|
Lonning PE, Helle SI, Johannessen DC, Ekse D, Adlercreutz H (1996). Influence of plasma estrogen levels on the length of the disease-free interval in postmenopausal women with breast cancer. Breast Cancer Res. Treat. 39(3):335-341. |
|
|
Marshall JR, Yinsheng Q, Junshi C, Parpia B, Campbell TC (1992). Additional ecological evidence: lipids and breast cancer mortality among women aged 55 and over in China. Eur. J. Cancer 28(10):1720-1727. |
|
|
McTiernan A (2000). Associations between energy balance and body mass index and risk of breast carcinoma in women from diverse racial and ethnic backgrounds in the U.S. Cancer 88(S5):1248-1255. |
|
|
McTiernan A, Rajan KB, Tworoger SS, Irwin M, Berstein L, Baumgarthe R, Gilliland F, Stanczyk FZ, Yasui Y, Ballar-Barbash R (2003). Adiposity and sex hormones in postmenopausal breast cancer survivors. J. Clin. Oncol. 21:1961-1966. |
|
|
McTiernan A, Tworoger SS, Ulrich CM, Yasui Y, Irwin ML, Rajan KB, Sorensen B, Rudolph RE, Bowen D, Stanczyk FZ, Potter JD (2004). Effect of exercise on serum estrogens in postmenopausal women: A 12-month randomized clinical trial. Cancer Res. 64(8):2923-2928. |
|
|
Morimoto LM, White E, Chen Z, Chlebowski RT, Hays J, Kuller L, Lopez AM, Manson J, Margolis KL, Muti PC, Stefanick ML (2002). Obesity, body size, and risk of postmenopausal breast cancer: the Women's Health Initiative (United States). Cancer Causes Control 13:741-751. |
|
|
Mourouti N, Kontogianni MD, Papavagelis C, Panagiotakos DB (2015). Diet and breast cancer: a systematic review. Int. J. Food Sci. Nutr. 66(1):1-42. |
|
|
Peeters K, Van Leemputte F, Fischer B, Bonini BM, Quezada H, Tsytlonok M, Haesen D, Vanthienen W, Bernardes N, Gonzalez-Blas CB, Janssens V, Tompa P, Versées W, Thevelei JM (2017). Fructose-1,6-bisphosphate couples glycolyticflux to activation of Ras. Nature Communications 8(1):922. |
|
|
Prentice RL, Kakar F, Hursting S, Sheppard L, Klein R, Kushi LH (1988). Aspects of the rationale for the Women's Health Trial. J. Natl. Cancer Inst. 80(11):802-814. |
|
|
Rossi RE, Pericleous M, Mandair D, Whyand T, Caplin ME (2014). The Role of Dietary Factors in Prevention and Progression of Breast Cancer. Anticancer Research 34(12):6861-6875 |
|
|
Sato R, Helzlsouer KJ, Alberg AJ, Hoffman SC, Norkus E P, Comstock GW (2002). Prospective study of carotenoids, tocopherols, and retinoid concentrations and the risk of breast cancer. Cancer Epidemiol. Biomarkers Prev. 11:451-457. |
|
|
Sellers TA, Vierkant RA, Cerhan JR, Gapstur SM, Vachon CM, Olson JE, Pankratz VS, Kushi LH, Folsom AR (2002). Interaction of dietary folate intake, alcohol, and risk of hormone receptor-defined breast cancer in a prospective study of postmenopausal women. Cancer Epidemiol. Biomarkers Prev.11:1104-1107. |
|
|
Shin MH, Holmes MD, Hankinson SE, Wu K, Colditz GA, Willett WC (2002). Intake of dairy products, calcium, and vitamin d and risk of breast cancer. J. Natl. Cancer Inst. 94(17):1301-1311. |
|
|
Thune I, Brenn T, Lund E, Gaard M (1997). Physical activity and the risk of breast cancer. New Engl. Med. J. 336(18):1269-1275. |
|
|
Thune I, Furberg AS (2001). Physical activity and cancer risk: Dose-response and cancer, all sites and site-specific. Med. Sci. Sports Exerc. 33(6):S530-S550. |
|
|
Welsch CW (1992). Relationship between dietary fat and experimental mammary tumorigenesis: a review and critique. Cancer Res. 52 (suppl 7):2040s-2048s. |
|
|
World Cancer Research Fund Panel (Potter JD Chair) (1997). Food, Nutrition and the Prevention of Cancer: a Global Perspective. Washington, DC: American Institute for Cancer Research. |
|
|
Wu AH, Ziegler RG, Nomura AM, West DW, Kolonel LN, Horn-Ross PL, Hoover RN, Pike MC (1998). Soy intake and risk of breast cancer in Asians and Asian Americans. Am. J. Clin. Nutr. 68(suppl 6):1437S-1443S. |
|
|
Zhang S, Hunter DJ, Hankinson SE, Giovannucci EL, Rosner BA, Colditz GA, Speizer FE, Willett WC (1999). A prospective study of folate intake and the risk of breast cancer. JAMA 281(17):1632-1637. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


