Full Length Research Paper
ABSTRACT
Alternative techniques for detecting cancer of the cervix uteri alongside its early precancerous lesions still remain necessary for low income environments since morbidity and mortality due to cervical cancer continues to be on the rise. We recruited one thousand and seventy-seven women aged 15-55 years from selected study hospitals in Eastern Uganda and examined them using Papanicolaou (Pap) smear, direct visual inspection with 5% acetic acid solution (VIA), and human papillomavirus (HPV) DNA testing. Study participants detected with high-grade lesions (HSIL) or cancer cells on Pap smear test, positive VIA test (acetowhite lesions, cervical ulcer or growth), and positive high-risk HPV DNA (relative light units (RLU) were immediately scheduled for colposcopy and cervical biopsy. Of the forty percent of the women confirmed with pap smear positive, 43 of the 63 women had invasive carcinoma (68.3%), while 89 out of 137 women with confirmed biopsy were diagnosed with high grade CIN (CIN2,3) (65%). DVI identified 46 of 63 carcinomas (73%) as well as 47 of 74 high grades CIN (CIN 2, 3) (64%). There was a variation in HPV DNA results due to the cutoff value considered in defining the final result. HPV DNA of high-risk HPV types was detected 39 (61.9%) out the 63 women diagnosed invasive cervical cancer, while 66 (73.3%) or 46 (51%) was detected in the biopsy of women diagnosed with high grade CIN (CIN 2,3). Similarity in identification of high-grade cervical abnormalities was registered by the testing methods. Both VIA and HPV genetic testing methods diagnosed similar numbers of high grade CIN 2,3 and invasive cancer cases as Pap smears. Nevertheless, individual test methods categorized study participants with no cervical disease as being positive.
Key words: Visual inspection with acetic acid (VIA), cervical intraepithelial neoplasia (CIN), human papillomavirus (HPV).
INTRODUCTION
Globally, high mortality rates due to cancer of the cervix uteri is still registered among middle aged women in low income environments in which 230, 000 women are reported to die annually (Ferlay et al., 2015; Bruni et al., 2017). Sub-Saharan Africa still registers the highest rates of incidence and mortality due to invasive cervical cancer in the world with the age standardized rate of 56 and 41 per 100000 women (Arbyn et al., 2011). Reports by GLOBOCAN (Ferlay et al., 2015; Bruni et al., 2017), revealed that Uganda ranked highest with the age-standardized incidence rate in the world of 44.4/100,000, while East Africa (ASR) of 42.7/100,000, and the World (ASR) of 14.0/100,000.
The control and decline in cervical cancer in developed countries is now well registered since the introduction of cytology-based screening strategies, but this has not yet been achieved in the developing countries in sub-Saharan Africa (Parkin et al., 2003). Reproducing and adopting these approaches to suite less developed nations like Uganda is still unachievable because of inadequate trained medical work force, and delayed specimen collection period to result dissemination (Blumenthal et al., 2007). Efforts by the Uganda government to introduce human papilloma virus (HPV) vaccine were a key cofactor and the key advance in the management of cancer of the cervix uteri in Uganda. Nevertheless, there is still a challenge in implementing large scale HPV vaccination in effective manner, large scale implementation of HPV vaccination is still challenging, and even when effective, the need for cervical cancer screening will still remain inadequate (Katz and Wrigh, 2006; Banura et al., 2008). Therefore, new considerations are now focused towards new testing methods which are affordable and reliable among the Ugandan women. Different approaches to conventional cytology have now been put in place, such as visual inspection with lugols iodine (VILI), visual inspection of the cervix with 5% acetic acid (VIA), and HPV DNA testing. These inventive approaches are cost effective and reliable in the management of invasive cancer of the cervix uteri since they can be used in a combination at all stages of the disease onset in low income setting (Goldie et al., 2001, 2005; Mandelblatt et al., 2002). Nevertheless, questions and alarms concerning the reliability and effectiveness of the newly developed test and treat approaches in less developed nations have arisen (Fokom-Domgue et al., 2014; Nakisige et al., 2017). Also, the newly developed approaches in cervical cancer testing are not globally acknowledged.
Back in the last century, World Health Organization and partner organizations approved various approaches for the management of cervical cancer in the developing nations. Furthermost, these schemes were intended to assess the viability and efficiency of different procedures for cervical cancer diagnosis in Sub-Saharan Africa (Adefuye et al., 2013). Main reports for the results of these study approaches differed; some findings stated that VIA was not suitable for cervical cancer screening in less developed countries in Africa (Cronje et al., 2003; Ajenifuja et al., 2013). Furthermore, large scale studies have assessed the precision of different screening procedures for cancer of the cervix uteri in other low-income countries, but no attention was granted to those in sub-Saharan Africa (Ajenifuja et al., 2013; Bradford and Goodman, 2013). In order to assess the performance of different testing procedures for low income environments, a study was conducted among previously unscreened women aged 15±55 years by performing Papanicolaou (Pap) smear test, visual inspection with 5% acetic acid (VIA), and HPV DNA testing. Results of VIA Test were given instantly to study participants upon examination, and were requested to coming back to the screening unit in 2±6 days upon reception their test results.
MATERIALS AND METHODS
Study area
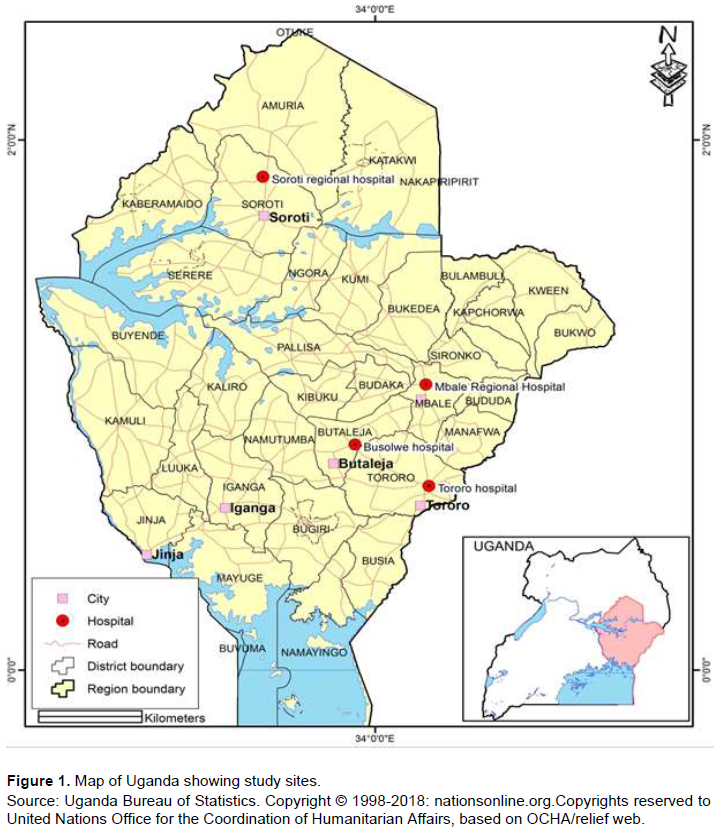
This research was performed in specified regional health facilities in Eastern Uganda, which include Tororo, Mbale, Butalejja, Kumi and Soroti referral hospitals. Accessibility to established screening facilities, professional oncologists and technologist for both inpatients and outpatients within these hospitals transformed them into testing and treatment facilities for the surrounding towns that lack them. Districts such as Moroto, Katakwi, Amuria, Kaberamaido, Ngora, Serere, Namalu, and Nakapiripirit with ineffective cancer treatment services entirely relied on these designated health facilities for their services (Figure 1).
Study design
This was a prospective study, with follow-up prior to the actual identification of high-grade intraepithelial neoplasia (CIN). A maximum of 1,077 women aged 15 to 55 years and accessing healthcare services were encouraged to take part in the screening program upon their eligibility to the participation criteria at the health facilities of Mbale, Tororo, and Butalejja and Soroti referral hospitals in Eastern Uganda. Women with recurrent vaginal discharge, external genital lesions, cervitis, irregular menstrual bleeding, post-coital hemorrhaging, or those identified to have an unhealthy cervix on review were requested to enroll in the cervical cancer test. The research omitted females who were < 15 and ≥55 years old as well as all females in their menstrual period. That's because the bleeding leakage during the menstruation could interfere with the visual activity of the cervix and give false positive results. The written informed consent of the participants was obtained, educating them of the purpose to the research, the drawbacks and the anticipated benefits. Ethical certification was acquired from Kampala International University (KIU), Mbarara University of Science and Technology (MUST) Institutional Ethical Committee (Approval No. 06/01-17) and the Uganda National council of Science and Technology (Approval No. HS2246). The research procedures have been carried out in compliance with the ethical guidelines of the Human Testing Committees set out in the Helsinki Declaration of 1964 updated in 2000.
Clinical examinations
Following a consultation with the study participants, informed written consent was received and short oral questionnaires were distributed. Two nurses who have been specialized in cervix VIA and Pap smear test conducted a gynecological review immediately. Nursing officers were taught to recommend all patients with acetowhite lesions along with all patients with endocervical lesions or genital wats. Hardly any attempt was allowed by the nurse to categorize the intensity of the abnormalities. Medical evaluations were done in three stages. In the first stage, a Pap test was obtained using an Accellon sampler (MedScand, Hollywood, FL); the very first specimen were extracted by a 360° rotation of the transition zone; the sample retrieved was then spread on the slide for rapid histologic assessment. In the second stage, the HPV DNA test specimen was collected using a standard accellon sampler by cutting the head of the Accellon into specimen collection tube (Digene Company, Silver Spring, MD); the end of the Spatula was broken up into a 15 ml holding tube containing 5 ml of PBS (pH 7.2) and then deposited for potential virological analysis. Specimens were briefly stored at 4°C for an average of 6 h and then placed in a freezer at 20°C for further tests. In the third stage, the cervical VIA was done by applying 5% acetic acid (Edmund Science, Barrington, NJ). Visual examination with acetic acid (VIA) was conducted by inserting a sterilized vaginal speculum into the vagina and followed by application of 5% acetic acid (vinegar) to the cervix. Unhealthy tissue looks slightly white/acetowhite when subjected to vinegar (WHO, 2017). The findings of the VIA test were promptly issued to patients, and all patients were requested to report to the health centre after the initial assessment.
Laboratory examinations
HPV Genetic material was analyzed every week with the first-generation Hybrid Capture II technique (Digene Corporation) at Mbale Regional Hospital in Eastern Uganda. The HPV DNA evaluation was conducted as directed by the manufacturer using probes for high oncogenic risk HPV types (types 16, 18, 31, 33, 35, 45, 51, 52 and 56). HPV assessments was interpreted as the proportion of the relative light units (RLU) of HPV DNA in the analysis to the positive control ratio of 10 pg / mL of HPV DNA (corresponding to approximately 100,000 HPV genome copies per test). Since the test was analytical, two separate HPV DNA levels were utilized to evaluate a positive outcome. The first cutoff threshold categorizes only specimens with substantially higher risk HPV DNA (RLU.>10×positive control or approximately > 100 pg / mL HPV DNA) as positive. This cutoff point was used to recommend patients to colposcopy. Furthermore, a second cutoff point was used in the study, which categorized specimens with low value of HPV DNA (RLU > 1×positive control) as positive. The lower cut-off threshold is indeed the normal level used mostly for clinical trials in Uganda.
Women with high-risk HPV DNA (RLU>10×positive control) or positive VIA findings undertook on-site colposcopy once they came back for their test outcome 2±5 days after their initial test. Colposcopic abnormalities were classified by Reid Colposcopic Index (Reid, 1990). Abnormalities categorized as less severe (Reid Score < 3) were surgically removed, whereas lesions graded as severe (Reid Score ≥ 3) were electro-excised utilizing loop electrodes. Endocervical curettage was done when no defects were evident. Any excised tissue and cytological samples were analyzed by a laboratory pathologist at the Mbale Regional Hospital. Histological findings were presented using two-tiered SIL nomenclature with low-grade SIL equal to (CIN 1) and high-grade SIL equal to (CIN 2, 3) respectively (Nayar and Wilbur, 2015; Singhal et al., 2018). Pap results were analyzed at the Mbale Regional Hospital cytopathology laboratory using the Bethesda methodology, and findings were readily accessible to patients within 20-22 weeks of Pap smear testing. Women with low-grade SIL, high-grade SIL, or carcinoma that had not yet undertaken colposcopy due to positive VIA or HPV tests were monitored when Pap findings were readily accessible and recommended for colposcopy. Patients with atypical squamous cells of undetermined significance (ASCUS) did not perform colposcopy because results from other alternate methods were negative.
Statistical analysis
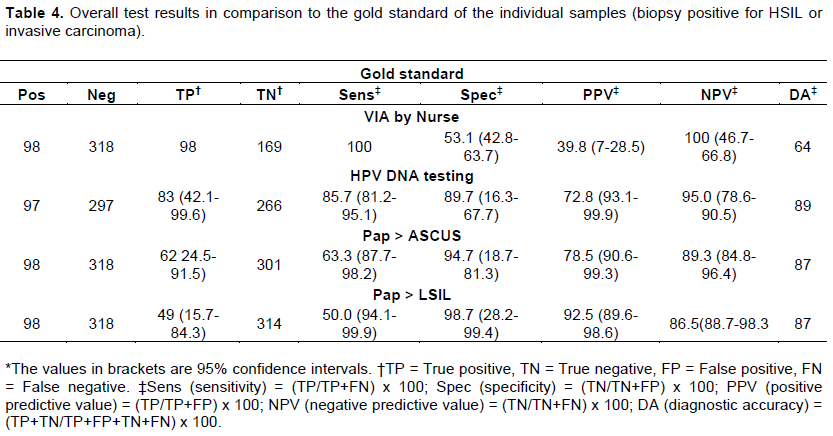
To assess the efficiency of the test methods, the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the individual analytic approaches were evaluated. Histopathology reports or colposcopy findings were used as the benchmark tool for determining the actual infection tissue excision had not been conducted in the event of a malignancy, thereby correcting for verification bias. The appearance of every lesion > CIN1 was the determining disease threshold. The criterion for consideration as positive for the three test procedures were as follows: for Pap, LSIL and above; for HPV, positive RLU > 1.0; for VIA, a well-defined aceto-white lesions stemming from the transformation zone.
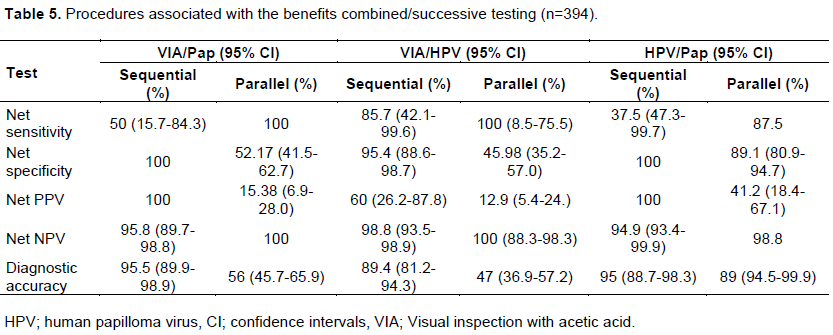
In order to assess the advantages of integrated testing procedures, the net sensitivity and accuracy of the alternate diagnostic approaches was added to the original results. For this method, two experiments were carried out. One was conducted on all study participants and, those detected as positive, the outcome was taken as positive and the next study was conducted on only those women who were positive in the first diagnosis. Although the previous method decreases the false negative probability, the latter lowers the false positive rate. Net sensitivity and specificity scores are the combined likelihood of a disease / non-disease getting identified using more than one approach.
RESULTS
Socio-demographic characteristics of studied participants
The research enrolled one thousand and seventy-seven women aged 15-55 years. The research participants who underwent the Pap test were categorized in regard to the form of hospital, age, educational level and marital status. In accordance with Hospital types, Mbale hospital recruited 302 (28.0%) study participants in which 137 (45.4%) were Pap smear positive and 165 (54.6%) Pap smear negative; while 154(51.0%) were VIA positive, and 148 (49.0%) VIA negative. Butalejja Hospital recruited 227 (21.1%) in which 108 (47.6%) were Pap smear positive and 119 (52.4%) Pap smear negative, while 122 (53.7%) were VIA positive and 105 (46.3%) negative. Tororo Hospital recruited 422 (39.2%) study participants in which 113 (26.8) were Pap smear positive and 309 (73.2%) negative, while 128 (30.3%) VIA positive and 294 (69.7%) VIA negative. Tororo hospital recruited 126 (11.7%) study participants in which 58 (46.0%) were Pap smear positive and 68 (54.0%) Pap smear negative, while 67(53.2%) were VIA positive and 59 (46.8%) VIA negative. In relation to age, the participants aged 35-44 years were frequently diagnosed positive with Pap smear test and VIA test respectively as compared to participants aged 15-24years. In the resent study 139 (42.5%) women aged 35-44 years were Pap smear positive and 202 (61.8%) were VIA positive, while 88 (35.8%), women aged 15-24 years were Pap smear positive and 68 (27.6%) were VIA positive (Table 1). Generally, the percentage (%) positivity of the rapid test kit was very high among the singles than married. This may be due to STIs since they might have more than one sexual partner compared to the married with one sexual partner.

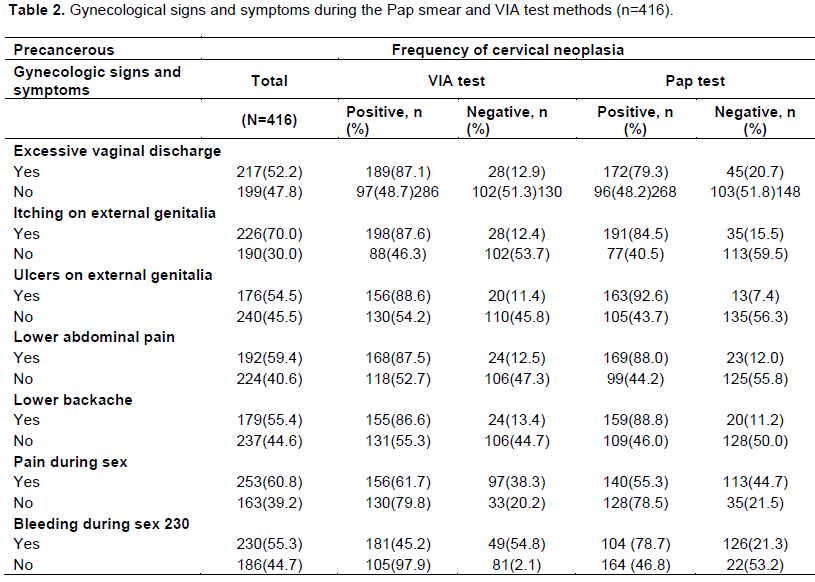
Gynecological signs and symptoms of the women during the screening test
The main concern was that 217 women had abnormal vaginal discharge, itching on external genitalia in 226 women, ulcers on external genitalia in 176 women, lower abdominal pain in 192 women, lower backache in 179 women, pain during sex in 253, and bleeding during sex in 230 women (Table 2).
Comparative analysis of the overall results of the three test methods
There were 63 incidents of histopathological identified intrusive cervical cancer, 90 incidents of high-grade CIN 2 or 3, and 95 incidents of low-grade CIN1. Of the 63 patients with invasive cancer and 90 with reported high-grade (CIN 2,3) biopsy confirmed within the research, VIA correctly detected 46 of 63 adenocarcinoma (73%) and 47 of 74 high-grade SIL (CIN 2,3) (64%). The burden of tumour-confirmed high-grade and low-grade SIL did not significantly vary among various ages: three incidents of HSIL and one of LSIL were reported in the age category < 40 years including in the age range ≥40 years. All patients with cancer of the cervix uteri were over 45 years of age. Nevertheless, the majority (23/63) of HPV-positive participants were < 40 years of age.
Of the 1077 Pap tests taken, 1047 (97.2%) were graded as "satisfactory for assessment." The average irregular occurrence, namely ASCUS, SIL, and carcinoma in situ, was 17%. Diagnosis of ≥LSIL / carcinoma was conducted on 40% of all Pap tests. This was the threshold standard used to refer patients for colposcopy in this report. In 43 of the 63 women with invasive carcinoma (68.3%), Pap results was graded as SIL or invasive carcinoma, and in 89 of the 137 women with biopsy, high grade SIL (CIN2, 3) was detected in (65%). This cutoff standard in this analysis was used for referring women for colposcopy (Table 3).
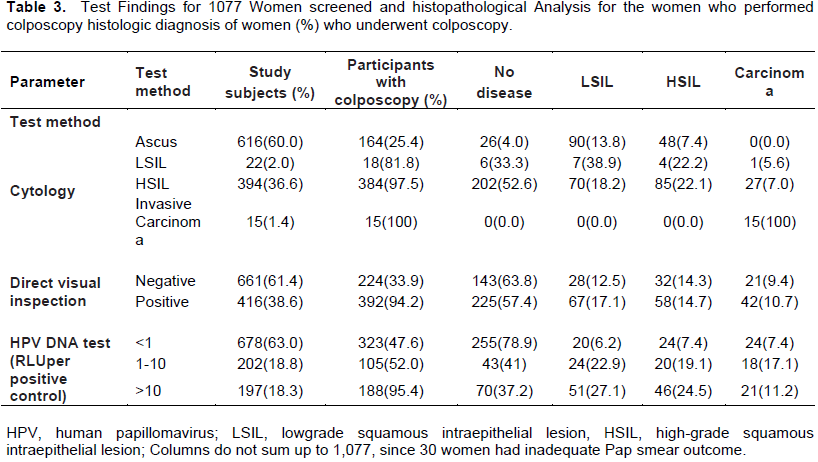
The majority of women (38.6%) were graded by the nurses as having an abnormal condition upon VIA examination with 5% acetic acid, while ninety-eight women with high-grade lesions were registered as positive for VIA. Endocervical diagnosis of precancer and cervical carcinoma, depending on the Reid index, associated well with histological evaluation. Just in 5 cases of invasive cancer, the Reid grade was < 2, also VIA was positive in this instance. The Reid index was roughly 3 in the remaining 46 cases of biopsy-proven lesions-HSIL. VIA skipped one event of LSIL (CIN 1) with a Reid score of 1. Of the 32 women with false-positive VIA outcomes, 16 had RCI ≥3, 8 had RCI 0-2, and 8 had no colposcopic proof of malignancy. By using Hybrid Capture II HPV DNA test, 399 (37%) of all females tested were confirmed to have been high-risk HPV DNA positive. Of these, 197 had a viral load of HPV DNA that was moderately high (RLU > 10 the positive control). High-risk HPV DNA was detected in 39 (61.9%) of 63 women with intrusive cervical cancer and 66 (73.3%) or 46 (51%) of women with high-grade SIL (CIN Grade 2, 3) reported biopsy at normal cutoff (RLU > 1×positive control) and high cutoff (RLU > 10×positive cont) amounts. The efficacy of the three screening tests was performed by determining the individual tests' sensitivity, specificity, PPV and NPV, as illustrated in Tables 4 and 5.
DISCUSSION
This recent research was designed to evaluate the efficiency of possible alternatives to cytological diagnosis for cancer of the cervix uteri in low income environment. This was the first large-scale clinical study of hospital-based Cancer of the cervix in patients aged 15 to 55 years in Eastern Uganda by using Pap test procedure, VIA and HPV DNA technique.
In this current research, VIA and HPV DNA analysis with Hybrid Capture II test (Digene Corporation) using typical cutoff point reported fairly similar percentages of high grade SIL (CIN 2, and CIN 3) and Intrusive incidents of cervical cancer, like was for traditional cytological testing in the hospitals surveyed. However, both approaches categorized many patients with no symptoms of cervical cancer as positive as cytology. This research was consistent with population-based studies (Sauvaget et al., 2011; Sankaranarayanan et al., 2012; Ajenifuja et al., 2013) that further revealed that visual diagnostic tests are better options to cytological testing in low income environments. Visual approaches are cheap, affordable and cost effective than cytological methods which involve complex setup and high technologists. It offers an instant outcome which is advantageous especially where accessibility to women with irregular test outcomes to treatment centers is impossible.
This research correlated well with other reports (Cronje et al., 2003; Sauvaget et al., 2011; Ajenifuja et al., 2013) that consistently found that the sensitivity of VIA to detect high grade SIL or invasive cervical carcinoma was equal to that of cytology. In a recent Indian study, for example, 3000 women were screened using VIA and cytology (Sauvaget et al., 2011). Ninety percent of patients of high grade SIL or invasive cancer of the cervix uteri was detected by VIA. VIA had a 77% sensitivity for CIN2, CIN3 and invasive cancer versus 44% for Pap smear result in an alternate experiment of similar model performed among palliative patients in Zimbabwe (Cronje et al., 2003). In fact, these results were in accordance with this research in which VIA had a sensitivity of 100% towards detection of cervical cancer compared to 50% of clinical cytological result in this research. Overall, based on the findings of these analyses, it suggests that perhaps the efficiency and sensitivity of VIA is adequate to permit its use in low income environments as an alternate cancer screening tool.
In addition, the recent observation showed that HPV DNA approach for detecting high-risk HPV types can detect an equal amount of high-grade SIL (CIN 2, 3) and invasive cancer of the cervix uteri as cytology supports the usefulness of HPV DNA testing as a tool for detecting patients with cervical cancer. Interestingly, limited studies have been conducted about application of HPV DNA analysis to be alternate diagnostic tool. In a sample of 350 Manipur women in India screened for high-risk HPV DNA using both Pap smear test and polymerase chain reaction, (Desai et al., 2019) recorded that sensitivity of HPV DNA testing for high-grade SIL or invasive cervical uterine cancer was 87.71% higher than that of cytology. Comparably, Sherman et al. (1998) recorded that in a survey of almost 10,000 Costa Rican women, 78% of patients with cancer of the cervix uteri diagnosed using cytology were HPVNA-positive at high risk using the Hybrid Capture II (Digene Corporation) (Sankaranarayanan and Wesley, 2003). Traditional testing procedures in general use in Uganda lead women who test positive for colposcopic analysis. Colposcopy, nonetheless, is a reasonably costly operation, and its facilities are mostly in shortage in low income areas. Consequently, the number of patients without severe cervical cancer identified as positives is significant as the actual cases of high-grade SIL (CIN 2, 3) and cervical cancer detected by laboratory analysis.
In the present research, both VIA and HPV DNA tests have showed that a significant number of women without high-grade disease were screened positive. High-risk HPV DNA was detected in 39 (61.9%) of 63 patients with intrusive cervical cancer and 66 (73.3%) or 46 (51%) of patients with high-grade SIL (CIN 2, 3) reported biopsy at normal cutoff levels (RLU > 1×positive control) and high cutoff levels (RLU > 10×positive control) accordingly. Close findings were observed for VIA (Bradford and Goodman, 2013). If either VIA or HPV genetic testing were also used to monitor cancer of the cervix uteri in Eastern Uganda, the existing colposcopic facilities would have been quickly overrun. The most probable source for poor accuracy of both VIA and HPV DNA tests of the present experiment are indeed the presumed higher incidence of venereal diseases among the study participants. Even though data on venereal diseases were not procured in the present studied population, very high prevalence of sexually transmitted diseases amongst females was noticed with a seroprevalence frequency of roughly 19% of human immunodeficiency virus (HIV), Trichomonas vaginalis in 25%, and 10% Neisseria gonorrhea, in concurrent surveys. Significant cervicovaginal complications render VIA even more complicated, and it is understood from the study that several incidents involving false-positive VIA exams are due to infection-related to cervical lesions and irritation.
CONCLUSION
Numerous approaches have been suggested to resolve the question of poor precision in VIA and HPV Genetic analysis. One that was currently designed, using observations from the hospitals assessed in Eastern Uganda, utilizes 2 consecutive diagnostic tests, and the second test is only done when the first result is positive. VIA accompanied by HPV tests will be the most appropriate screening method for the detection of females looking for extra treatment. Related observations were taken from research of Blumenthal et al. (2001). Smear test and HPV specimens at the same time had a clinical efficacy of 89%. The strength of this mixed approach rests in its high negative predictive potential, which can minimize the necessary follow-up amplitude and proximity. Females who are Pap and HPV negative are at exceptionally low risk of contracting illness, but those who are positive require more regular, colposcopy-assisted assessments. The precision of the diagnostic procedure is significantly improved by this two-stage diagnostic approach, but still the increase in precision is followed by a decrease in sensitivity. Another strategy is to disregard the poor specificity of test results for DVI and HPV DNA and merely treat all patients who really are positive for the diagnostic test (Sanghvi, 1998). This approach points out that cytological and colposcopic resources are highly doubtful to be accessible in several resource-poor environments in the coming future and also that invasive cervical cancer remains a significant medical issue for people who need to be treated urgently. While there are apparent benefits of integrating VIA or HPV DNA in disease intervention among women diagnosed as cancer positive, large-scale protection and effectiveness of clinical trials are required to closely examine the clinical and analytic complications of over treating substantial percentage of patients without cancer of the cervix uteri in the total lack of colposcopic guidance in low income environments. The application of VIA accompanied by HPV monitoring might more reliably classify non-disease incidents, at the cost of a small decline in sensitivity and identification frequency. This strategy would decrease the rate of referrals and care, and even the amount of appointments needed for diagnosis of diseases. The results of this study are promising and suggest that broader multicenter trials will help direct Uganda's government policy.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
ACKNOWLEDGMENTS
The authors appreciate the medical personnel of Mbale Regional Referral Hospital, Butalejja-Busolwe Hospital, Tororo Hospital and Soroti Regional Hospital for the logistical support during evaluation stage. As a result, they would like to thank all the respondents who gave their approval to this research project. They also appreciate the administration of Kampala International University Western campus for the support they offered during the study time.
REFERENCES
|
Adefuye P, Broutet N, de Sanjose S, Denny L (2013). Trials and projects on cervical cancer and human papillomavirus prevention in sub-Saharan Africa. Vaccine 31(5):F53-9. |
|
|
Ajenifuja K, Gage J, Adepiti A (2013). A population-based study of visual inspection with acetic acid (VIA) for cervical screening in rural Nigeria. International Journal of Gynecologic Cancer 23:507-12. |
|
|
Arbyn M, Castellsagué X., de Sanjosé, S, Bruni L, Saraiya M, Bray F, Ferlay J (2011). Worldwide burden of cervical cancer in 2008. Annals of Oncology 22(12):2675-2686. |
|
|
Banura C, Franceschi S, van Doorn LJ, Arslan A, Kleter B, Wabwire?Mangen F, Mbidde EK, Quint W, Weiderpass E (2008). Prevalence, incidence and clearance of human papillomavirus infection among young primiparous pregnant women in Kampala, Uganda. International Journal of Cancer 123(9):2180-7. |
|
|
Blumenthal P, Gaffikin L, Deganus S, Lewis R, Emerson M, Adadevoh S (2007). Cervical cancer prevention: safety, acceptability, and feasibility of a single-visit approach in Accra, Ghana. American Journal of Obstetrics and Gynecology 196(4):407-e1 |
|
|
Blumenthal PD, Gaffi kin L, Chirenje ZM, McGrath J, Womack S, Shah K (2001). Adjunctive testing for cervical cancer in low resource set-tings with visual inspection, HPV and the Pap smear. International Journal of Gynecology and Obstetrics 72(1):47-53. |
|
|
Bradford L, Goodman A (2013). Cervical cancer screening and prevention in low-resource settings. Clinical Obstetrics and Gynecology 56:76-87. |
|
|
Bruni L, Barrionuevo-Rosas L, Albero G, Serrano B, Mena M, Gómez D, Muñoz J, Bosch FX, de Sanjosé S (2017). ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in Uganda. Summary Report 27 July. |
|
|
Cronje H, Parham G, Cooreman B, de Beer A, Divall P, Bam R (2003). A comparison of four screening methods for cervical neoplasia in a developing country. American Journal of Obstetrics and Gynecology 188(2):395-400. |
|
|
Desai F, Singh LS, Majachunglu G, Kamei H (2019). Diagnostic Accuracy of Conventional Cell Blocks Along with p16INK4 and Ki67 Biomarkers as Triage Tests in Resource-poor Organized Cervical Cancer Screening Programs. Asian Pacific Journal of Cancer Prevention 20(3):917. |
|
|
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2015). Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International Journal of Cancer 136(5):E359-86. |
|
|
Fokom-Domgue J, Vassilakos P, Petignat P (2014). Is screen-and-treatapproach suited for screening and management of precancerous cervical lesions in Sub-Saharan Africa? Preventive Medicine 65:138-40. |
|
|
Goldie S, Denny L, Pollack A, Wright T (2001). Policy analysis of cervical cancer screening strategies in low-resource settings: clinical benefits and cost-effectiveness. JAMA 285(24):3107-3115 |
|
|
Goldie S, Gaffikin L, Goldhaber-Fiebert J, (2005). Cost-effectiveness of cervical-cancer screening in five developing countries. New England Journal of Medicine 353(20):2158-2168. |
|
|
Katz I, Wright A (2006). Preventing cervical cancer in the developing world. New England Journal of Medicine 354(11):1110-1110. |
|
|
Mandelblatt J, Lawrence W, Gaffikin L (2002). Costs and benefits of different strategies to screen for cervical cancer in less-developed countries. Journal of the National Cancer Institute 94(19):1469-1483. |
|
|
Nakisige C, Schwartz M, Ndira AO (2017). Cervical cancer screening and treatment in Uganda. Gynecologic Oncology Reports.20:37-40. |
|
|
Nayar R, Wilbur DC Eds. (2015). The Bethesda system for reporting cervical cytology: definitions, criteria, and explanatory notes. Springer. |
|
|
Parkin, DM, Ferlay J, Hamdi-Cherif M, Sitas F, Thomas JO, Wabinga H, Whelan SL (2003). Cancer in Africa. Epidemiology and prevention, 4, 268-276. |
|
|
Reid R (1990). Colposcopy of cervical preinvasive neoplasia. In:Singer A, editor. Premalignant Lesions of the Lower Genital Tract 2:87-116. |
|
|
Sankaranarayanan R, Nessa A, Esmy P, Dangou J (2012). Visual inspection methods for cervical cancer prevention. Best practice and research Clinical Obstetrics and Gynaecology 26(2):221-232. |
|
|
Sankaranarayanan R, Wesley R (2003). A practical manual on visual screening for cervical neoplasia. International Agency for Research on Cancer. World Health Organization, pp.1-4. |
|
|
Sanghvi H (1998). Treatment experiences in low resource settings.In: Abwao S, Greene P, Sanghvi H, Tsu V, Winkler JL, editors. Prevention and control of cervical cancer in the east and southern Africa region. |
|
|
Sauvaget C, Fayette J, Muwonge R, Wesley R, Sankaranarayanan R (2011).Accuracy of visual inspection with acetic acid for cervical cancer screening. International Journal of Gynecology and Obstetrics 113(1):14-24. |
|
|
Sherman ME, Mendoza M, Lee KR, Ashfaq R, Birdsong GG,Corkill ME, (1998). Performance of liquid-based, thin-layercervical cytology: correlation with reference diagnoses andhuman papillomavirus testing. Modern pathology: an official journal of the United States and Canadian Academy of Pathology, Inc, 11(9):837-843. |
|
|
Singhal U, Lamba S, Kumar, U, Nanda A (2018). Pattern of Epithelial Cell Abnormalities on Cervical Papanicolaou Smears In Hospital Of North India: A Retrospective Study. Annals of Pathology and Laboratory Medicine 5(3):A250-255. |
|
|
Uganda Bureau of Statistics (UBOS, 2018). Health planning in Uganda: Carey, R.B., Bhattacharyya, S., Kehl, S. C., Matukas, L. M., Pentella, M. A., Salfinger, M., & Schuetz, Implementing a quality management system in the medical microbiology laboratory. Clinical Microbiology Reviews 31(3):e00062-17. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


