Full Length Research Paper
ABSTRACT
Diabetes mellitus (DM) is a common endocrine metabolic disorder and a leading cause of death worldwide. Dyslipidemia is a well-recognized manifestation of uncontrolled DM, because insulin has important regulatory effects on lipid metabolism. This study was conducted to determine the frequency and pattern of dyslipidaemia in diabetic patients. Cross-sectional study was conducted on a total of two hundred ninety five diabetic patients attending diabetic follow-up clinic of Hawassa University Referral Hospital from March to November, 2014. For each selected subject, structured questionnaire about socio-demographic characteristics and diabetic related information was filled; overnight fasting blood samples were analyzed for fasting blood sugar (FBS) and lipid profiles, namely, total cholesterol (TC), triglyceride (TG), high density lipoprotein (HDL) and low density lipoprotein (LDL). Dyslipidemia was assessed according to the United State National Cholesterol Education Program Adult Treatment Panel III (NCEP-ATP-III) model guideline. SPSS version 20 was used as tool for data analysis. P-value of <0.05 was used as statistical significance. The mean (± standard deviation, SD) values of TC, TG, HDL, LDL were 186.03 (± 37.40), 194.33 (± 93.38), 49.66 (± 10.34), 119.15 (± 42.33) mg/dl, respectively. Among all of the diabetic patients, 34.9% had high serum LDL, 34.6% had hypercholesterolemia, 29.8% had hypertriglyceridemia and 12.2% had low HDL. Significantly higher mean serum levels of TC (p = 0.002) and LDL (p = 0.008) were noted in type 2 DM than type 1 DM. Females had significantly higher TC and LDL levels than males; whereas males had significantly lower HDL levels as compared to females (48.04 ± 9.13 versus 51.93 ± 11.49 mg/dl; p < 0.001). The mean (± SD) FBS level was 178.18(± 85.39) mg/dl and patients with type 1 DM had significantly higher FBS than those with type 2 DM (p < 0.001). Our study showed the presence of dyslipidaemia in Ethiopians with DM. The most common dyslipidemia in this study was high level of serum LDL followed by hypercholesterolemia and hypertriglyceridemia. The optimal care for diabetic patients should also include routine monitoring of serum lipid profile.
Key words: Diabetes, lipid profile, dyslipidemia.
Abbreviation: DM, Diabetes mellitus; HDL, high density lipoprotein; LDL, low density lipoprotein; TC, total cholesterol; TG, triglycerides; T1DM, type 1 diabetes mellitus; T2DM, type 2 Diabetes Mellitus; NCEP-ATP, National Cholesterol Education Program, Adult Treatment Panel.INTRODUCTION
Diabetes mellitus (DM) is a group of metabolic diseases characterized by hyperglycemia resulting from defects in insulin secretion, insulin action or both. Insulin deficiency in turn leads to chronic hyperglycaemia with disturbances of carbohydrate, fat and protein metabolism. Diabetes is associated with long term damage, dysfunction and failure of various organs, especially the eyes, kidneys, nerves, heart and blood vessels (Salim, 2005; Kumar and Clark, 2002; Expert, 1997). DM is related with greater risk of mortality from cardiovascular disease (CVD) which is well known as dyslipidaemia. Dyslipidaemia is defined by the presence of one or more than one abnormal serum lipid concentration according to United State National Cholesterol Education Program Adult Treatment Panel (NCEP-ATP) III guideline (NCEP, 2002). In type 2 diabetes mellitus (T2DM), the most common abnormal lipid pattern is a combination of elevated TG levels and decreased HDL cholesterol (Dunn, 1990); whereas the dyslipidemia seen in poorly controlled type 1 diabetes mellitus (T1DM) is mainly due to accumulation of chylomicrons and very low density lipoproteins in the plasma (Chase and Glasgow, 1976; Bagdade et al., 1967). Nevertheless, in both groups of DM, normalization of glycemic control is followed by improvement or normalization of the dyslipidemias (Weidman et al., 1982). Abnormal serum lipids are likely to contribute to the risk of coronary artery disease in diabetic patients (Miller, 1999) and the determination of the serum lipid levels in people with diabetes is now considered as a standard of the diabetes care (ADA, 1999).
Worldwide, there are more than 154 million diabetics and its prevalence is on the increase in the developing countries (Bennett, 2000; Sajjadi et al., 2005). The estimated number of people living with diabetes in Africa is currently 12.1 million, but a recent projection (IDF, 2009) showed that the number will reach 23.9 million by 2030. In Ethiopia, no population based prevalence study exists but from hospital based studies, it can be seen that the prevalence of diabetes admission has increased from 1.9% in 1970 to 9.5% in 1999 of all medical admissions (Feleke and Enquselassie, 2005; Seyoum et al., 1999; Lester and Tsega, 1976). World Health Organization estimated (WHO, 2013) the number of diabetics in Ethiopia to be about 800,000 cases by the year 2000, and the number is expected to increase to 1.8 million by 2030. In Ethiopia, glycemic control and management of co-morbid conditions on top of diabetes complications are alarmingly sub-optimal and perhaps one of the worst in the world. This problem was also evident by findings of only 4.9% diabetic patients, who had lipid test over the last five years of follow up (Feleke and Enquselassie, 2005; Gudina et al., 2011). There are limited studies on the prevalence of lipid abnormalities in patients with diabetes from Horn of Africa. Therefore, the present work was carried out to determine the frequency and pattern of dyslipidaemia among diabetic patients attending diabetic follow-up clinic of Hawassa University Referral Hospital, Southern Ethiopia.
METHODOLOGY
A cross sectional study was conducted on a total of two hundred ninety five diabetic patients attending diabetic follow-up clinic of Hawassa University Referral Hospital from March to November, 2014. The study subjects enrolled in this study were all diabetic patients attending diabetic clinic for follow up of their treatment during the study period. Among all study participants, 172 (58.3%) were male and 123 (41.7%) were female diabetic patients and all were randomly selected and examined for dyslipidemia. Patients with other alignment and metabolic disorders were excluded from the study. Ethical clearance was obtained from Institutional Review Board (IRB) of the College of Medicine and Health Sciences, Hawassa University. The aim of this study was explained to the subjects and those who gave informed consent were included in the study. Five milliliters of venous blood samples were collected from all patients after an overnight fasting into Serum Separator Tube (SST) Vacutainer System (BD Diagnostics, New Jersey, USA). The sample was allowed to clot and centrifuged at 1,500 rpm for 5 min. CHOD-PAP Enzymatic Colorimetric (HUMAN GmbH, Wiesbaden, Germany) and GOD-PAP Enzymatic Colorimetric (HUMAN GmbH, Wiesbaden, Germany) methods were used for determination of lipid profiles and blood glucose, respectively. All of these biochemical analyses were carried out using automated chemistry analyzer (Vegasys, AMS, Italy). For serum lipid reference level the NCEP-ATP III guideline (NCEP, 2002) was referred and in accordance with this guideline: hypercholesterolemia and hypertriglyceridemia were defined as TC ≥ 200 mg/dl and TG ≥ 150mg/dl, respectively; while high level of LDL was defined as LDL ≥ 130 mg/dl and low level of HDL was defined as HDL < 40 mg/dl. SPSS ver.20 (SPSS Inc. Chicago, IL, USA) was used as tool for data analysis. Descriptive statistics was given as means (± SD) for continuous variables and as frequency and percentage of study population for categorical variables. Chi-square (c2) test was used to explore the relationship among categorical variables. The level of significance was considered at probability level (p-value < 0.05).
RESULTS
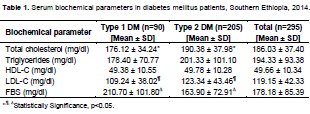
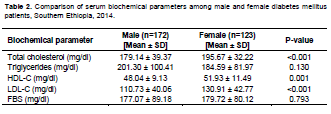
Of the total 295 subjects studied, 205 (69.5%) patients had T2DM and 90 (30.5%) had T1DM. The overall mean (± SD) age of study participants was 45.6 (± 16.6) years. The mean (± SD) age for patients with T1DM and T2DM were 28.56 ± 12.30 and 53.08 ± 12.21 years, respectively. Patients with type 2 diabetes were significantly (p < 0.001) older than those with type 1 diabetes. The mean (± SD) duration of diabetes was 8.6 ± 2.7 years and it was longer in patients with T2DM than in patients with T1DM (9.4 ± 1.7 versus 3.9 ± 0.8 years, p < 0.05). The biochemical parameters in all diabetic patients and with respect to types of DM (that is, types 1 and 2) patients are shown in Table 1, while comparison of patients’ serum biochemical parameters according to gender is shown in Table 2. The mean (± SD) serum LDL cholesterol level was 119.15 ± 42.33 mg/dl and 34.9% of the studied patients had serum LDL level higher than 130 mg/dl. There was significant difference between types 1 and 2 DM patients (109.24 ± 38.02 versus 123.34 ± 43.46 mg/dl; p = 0.008) as well as among males and females (110.73 ± 40.06 versus 130.91 ± 42.77 mg/dl; p < 0.001) with regard to serum LDL levels. The mean (± SD) serum total cholesterol level was 186.03 (± 37.40) mg/dl and 34.6% of the studied patients had serum total cholesterol level higher than 200 mg/dl. Serum total cholesterol levels were significantly higher in T2DM (190.38 ± 37.98) than T1DM (176.12 ± 34.24) (p = 0.002). There was also significant difference (p < 0.001) in mean serum cholesterol level between male (179.14 ± 39.37 mg/dl) and female (195.67 ± 32.22 mg/dl). The mean (± SD) serum triglyceride level was 194.33 (± 93.38) mg/dl and among all study participants, 29.8% had serum triglyceride levels higher than 150 mg/dl. There was no difference in mean serum triglycerides levels between types 1 and 2 DM patients (p = 0.762) or among males and females (p = 0.130). The mean (± SD) serum HDL cholesterol levels were 49.66 ± 10.34 mg/dl. Thirty six (12.2%) of DM patients had HDL values below 40 mg/dl. HDL levels were significantly higher (p=0.001) in females (51.93 ± 11.49 mg/dl) than males (48.04 ± 9.13 mg/dl), while there was no difference in HDL levels between types 1 and 2 DM patients. The mean (± SD) fasting blood sugar level was 178.18 (± 85.39) mg/dl and 216 (73.2%) of patients had mean FBS level above 120 mg/dl. Type 1 DM patients had significantly higher FBS than those with type 2 DM (210.70 ± 101.80 versus 163.90 ± 72.91 mg/dl; p < 0.001). There was no difference between males and females with respect to FBS levels. Table 3 shows comprehensive frequency of the biochemical variables in all diabetic patients, and among types of DM according to the NCEP-ATP III classification. The category immediately above the borderline high threshold levels for TC, TG and LDL, were ≥240, ≥200 and ≥160 mg/dl, respectively. Based on this categorization, among all of diabetic patients 16.9% had TG ≥200 mg/dl, 16.3% had LDL ≥160 mg/dl, and 7.8% had TC ≥240 mg/dl. Serum LDL level above 160 mg/dl was found in 37 (18%) of type 2DM patients while 11 (12.2%) of T1DM patients had this LDL value.
DISCUSSION
In diabetic patients, several researches have evidently established that complications are mainly due to chronic hyperglycemia that exerts its adverse to health effects through numerous mechanisms: dyslipidemia, platelet activation, and altered endothelial metabolism (Ozder, 2014; Brownlee, 2001; Taskinen, 2003). Lipid profile and diabetes together have been revealed to be the important predictors for metabolic disturbances including dyslipidaemia, hypertension, and cardiovascular diseases. Lipids play a significant role in the pathogenesis of DM. Dyslipidemia as a metabolic abnormality is commonly associated with DM. Abnormalities in lipid metabolism have been reported in patients with DM accompanied by the risk of cardiovascular arteriosclerosis (Goldberg, 2001; Krauss, 2004). Similar to observations in other population, our study demonstrated that patients with diabetes had higher LDL, TC, and TG levels as well as lower HDL levels. There is obvious proof in the study that in patients with diabetes and dyslipidemia, both conditions are independent cardiovascular risk factor (Dunn, 1990). The Multiple Risk Factor Intervention Trial (MRFIT) reported that patients with DM had more than 3-fold greater risk of cardiovascular problems than non diabetic patients (Stamler et al., 1984). In the current study, significantly higher mean serum levels of LDL cholesterol, total cholesterol, and triglycerides were noted in patients with diabetes, which are well known risk factors for cardiovascular diseases among diabetic patients. Higher level of LDL (34.9%) and hypercholesterolemia (34.6%) were the most frequent and found almost in similar proportion in all diabetic patients. The third prevalent dyslipidemia was hypertriglyceridemia affecting 29.8% of studied subjects. The elevated level of LDL observed from this study, was also seen in a study done in the US (Saaddine et al., 2002) and Jordan (Abdel-Aal et al., 2008); their data showed that the most common form dyslipidemia was higher LDL. The findings of hypercholesterolemia and hypertriglyceridemia are almost half way between two studies from Ethiopia (Seyoum et al., 2003; Siraj et al., 2006), in which hypercholesterolemia was found the most prevalent with 18.5 to 47.5% of all studied diabetic patients; while hypertriglyceridemia was the second prevalent with 14.2 to 41.8% of all study participants. In addition, our result has some similarity with study from Botswana (Addisu, 2006) but by far lower than study finding from the UK (Lawrence et al., 2001) and Jordan (Abdel-Aal et al., 2008). The pattern of dyslipidemia in our study varied from the ‘typical’ diabetic dyslipidemia as reported by several studies (Dunn, 1990; Chase and Glasgow, 1976; Bagdade et al., 1967). In our patients, this ‘typical’ diabetic dyslipidemia was observed, but its presence was not as such significant. Our finding indicated that elevated LDL and TC level was the most prevalent form of dyslipidemia. The difference in the pattern of dyslipidemia cited by different studies may be affected by factors arising from difference in cut points, variation of study populations and different observation method across these studies. Aside from genetic diversities, cultural factors, exercise and dietary pattern and treatment schemes may affect the pattern of dyslipidemia in patients with DM.
In this study, serum TC and LDL levels were found significantly higher in female (p < 0.001) as compared with males. This gender difference is similar to the TC in Jordan (Abdel-Aal et al., 2008) and UK (Prospective Diabetes Study, 1997) study; and for LDL in study from Botswana (Addisu, 2006). Furthermore, the Jordanian study (Abdel-Aal et al., 2008) stated that gender was considered as a major factor for determining the TC and LDL levels. Our finding is also supported by other study (Firdous and Khan, 2007); their finding stated that adverse effects of DM on dyslipidemias are more marked in women than men. Contrary, females in our study had higher HDL level that is consistent with other study (Summerson et al., 1992), whereas this observation is not in congruent with studies from Malaysia (Ismail et al., 2001) and Kuwait (Al-Adsani et al., 2004). Our study also demonstrated that significantly elevated TC level (p=0.002) and LDL level (p=0.008) in T2DM than T1DM, this finding is similar with other study (Seyoum et al., 2003); while this finding varied from other report (Siraj et al., 2006; Addisu, 2006). The mean FBS of 178.18 (± 85.39) mg/dl is comparable to report by Gudina et al. (2011), while it is better than the 190 ± 89.6 mg/dl in Addis Ababa (Feleke and Enquselassie, 2005); however, it is far higher than the recommendations in the developed world (ADA, 1999; Brownlee, 2001). 216 (73.2%) patients had FBS above 120 mg/dl, almost similar to other studies (Feleke and Enquselassie, 2005; Gudina et al., 2011). Feleke and Enquselassie (2005) found 79% having >120 mg/dl and Gudina et al. (2011) found 73.1% having > 130 mg/dl; indicating that glycaemic control in Ethiopia is very poor and not properly addressed. Another finding with regard to FBS was with higher level of FBS in T1DM patients as compared with T2DM, which was also reported from previous studies.
CONCLUSION
The current study demonstrated the presence of dyslipidemia in diabetic patients of Southern Ethiopia. The increase in LDL and TC were more pronounced than the other lipid abnormalities. This finding of dyslipidemia, which might be playing a major role in increasing the relative risk for the development of cardiovascular diseases, deserved appropriate attention from health care providers. It also echoed the need of incorporating serum lipid profile as regular laboratory investigation for monitoring of diabetic patients, in order to minimize the possible complications resulted from terminal dyslipidemia.
ABBREVIATIONS
DM, Diabetes mellitus; HDL, high density lipoprotein; LDL, low density lipoprotein; TC, total cholesterol; TG, triglycerides; T1DM, type 1 diabetes mellitus; T2DM, type 2 Diabetes Mellitus; NCEP-ATP, National Cholesterol Education Program, Adult Treatment Panel.
ACKNOWLEDGEMENTS
The authors want to thank all the patients, who have generously given their time to be involved in this study. They also would like to thank Ms. Yeshiareg Behailu and all staff working in the Diabetic Follow Up Clinic, Hawassa University, Referral Hospital, and acknowledge the Hawassa University for financial and logistic support.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
|
Abdel-Aal NM, Ahmad AT, Froelicher ES, Batieha AMS, Hamza MM, Ajlouni KM (2008). Prevalence of dyslipidemia in patients with type 2 diabetes in Jordan. Saudi Med. J. 29(10):1423-1428. Pubmed |
||||
| Addisu YM (2006). Lipid profile among diabetes patients in Gaborone, Botswana. S. Afr. Med. J. 96(2):147-148. | ||||
|
Al-Adsani A, Memon A, Suresh A (2004). Pattern and determinants of dysliipidemia in type 2 diabetes mellitus patients in Kuwait. Acta Diabetol. 41:129-135. Crossref |
||||
| American Diabetes Association (ADA) (1999). The management of dyslipidemia in adults with diabetes. Diabetes Care 22(Suppl. I):S56-S59. | ||||
|
Bagdade JD, Parte Jr D, Bierman E (1967). Diabetic lipemia. A form of acquired fat induced lipemia. N. Engl. J. Med. 276:427-433. Crossref |
||||
| Bennett PH (2000). Epidemiology of type 2 diabetes mellitus In: Lekoith D, Taylor SI, Olefsky JM (eds.), Diabetes Mellitus. New York: Wolter pp. 544-557. | ||||
|
Brownlee M (2001). Biochemistry and molecular cell biology of diabetic complications. Nature 414(6865):813-820. Crossref |
||||
|
Chase HP, Glasgow AM (1976). Juvenile diabetes mellitus and serum lipids and lipoprotein levels. Am. J. Dis. Child 130(10):1113-1117. Crossref |
||||
|
Dunn FL (1990). Hyperlipidemia in diabetes mellitus. Diabetes Metab. Rev. 6:47-61. Crossref |
||||
|
Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (1997). Report of the expert committee on the diagnosis and classification of Diabetes Mellitus. Diabetes Care 20:1183-1197. Crossref |
||||
| Feleke Y, Enquselassie F (2005). An assessment of the health care system for diabetes in Addis Ababa, Ethiopia. Ethiop. J. Health Dev. 19(3):203-210 | ||||
| Firdous S, Khan MZ (2007). Comparison of patterns of lipid profile in type-2 diabetics and non-diabetics. Ann. King Edward. Med. Coll. 3(1):84-7. | ||||
|
Goldberg IJ (2001). Diabetic dyslipidemia: causes and consequences. J. Clin. Endocrinol. Metab. 8 (3):965-971. Crossref |
||||
|
Gudina EK, Amade ST, Tesfamichale FA, Ram R (2011). Assessment of quality of care given to diabetic patients at Jimma University Specialized Hospital diabetes follow-up clinic, Jimma, Ethiopia. BMC Endocr. Disord. 11:19 Crossref |
||||
| IDF (2009). Diabetes Atlas. 4th edn. International Diabetes Federa¬tion. Available at: http://www.diabetesatlas.org/downloads | ||||
|
Ismail IS, Nazaimoon W, Mohamed W, Letchuman R, Singaraveloo M, Hew Fl, Shuguna C, Khalid BA (2001). Ethnicity and glycemic control are major determinants of diabetic dyslipidemia in Malaysia. Diabet. Med. 18:501-508. Crossref |
||||
|
Krauss RM (2004). Lipids and lipoproteins in patients with type 2 diabetes. Diabetes Care 27(6):1496-1504. Crossref |
||||
| Kumar PJ, Clark M (2002). Textbook of Clinical Medicine. 6th ed. London: Saunders Ltd. | ||||
|
Lawrence JM, Bennett P, Young A, Robinson AM (2001). Primary care screening for diabetes in general practice: cross sectional population study. BMJ 323:548-551. Crossref |
||||
|
Lester FT, Tsega E (1976). The pattern of adult medical admissions in Addis Ababa, Ethiopia. East Afr. Med. J. 53:620-634. Pubmed |
||||
|
Miller M (1999). The epidemiology of triglycerides as a coronary artery disease risk factor. Clin. Cardiol. 22(Suppl. II):111-116. Crossref |
||||
|
National Cholesterol Education Program (NCEP) (2002). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 106:3143-3421. Pubmed |
||||
|
Ozder A (2014). Lipid profile abnormalities seen in T2DM patients in primary healthcare in Turkey: a cross-sectional study. Lipids Health Dis. 13:183 Crossref |
||||
|
Saaddine JB, Engelgau MM, Beckles GL, Gregg EW, Thompson TJ, Narayan KM (2002). A diabetes report card for the United States: quality of care in the 1990s. Ann. Intern. Med. 136:565 Crossref |
||||
| Sajjadi F, Mohammadifard N, Ghaderian N, Alikhasi H, Maghroon M (2005). Clustering of cardiovascular risk factors in diabetic and IGT cases in Isfahan province. 2000 - 2001: Isfan healthy heart program. ARYA J. 1(2):94-100. | ||||
| Salim B (2005). Review Diabetes mellitus and its treatment. Int. J. Diabet. Metab. 13:111-13. | ||||
|
Seyoum B, Abdulkadir J, Berhanu P, Feleke Y, Mengistu Z, Worku Y, Ayana G (2003). Analysis of serum lipids and lipoproteins in Ethiopian diabetic patients. Ethiop. Med. J. 41(1):1-8. Pubmed |
||||
| Seyoum B, Abdulkadir J, Gebregziabher F, Alemayehu BB (1999). Analysis of diabetic patients admitted to Tikur Anbessa Hospital over eight years period. Ethiop. J. Health Dev. 13(1):9-13. | ||||
|
Siraj ES, Seyoum B, Saenz C, Abdulkadir J (2006). Lipid and lipoprotein profiles in Ethiopian patients with diabetes mellitus. Metabolism 55(6):706-710. Crossref |
||||
| Stamler J, Wentworth D, Neaton J, Schoenberger JA, for the MRFIT Research Group (1984). Diabetes and risk of coronary, cardiovascular and all cause mortality: findings for 356,222 men screened by the Multiple Risk Factor Intervention Trial (MRFIT). Circulation 70(Suppl II):161 | ||||
|
Summerson JH, Konen JC, Dignan MB (1992). Racial differences in lipid and lipoprotein levels in diabetes. Metabolism 41(8):851-855. Crossref |
||||
|
Taskinen MR (2003). Diabetic dyslipidaemia: from basic research to clinical practice. Diabetologia 46(6):733-749. Crossref |
||||
|
U.K. Prospective Diabetes Study Group (1997). U.K. Prospective Diabetes Study 27: Plasma lipids and lipoproteins at diagnosis of NIDDM by age and sex. Diabetes Care 20(11):1683-1687. Crossref |
||||
|
Weidman SW, Ragland JB, Fisher JN, Kitabchi AE, Sabesin SM (1982). Effects of insulin on plasma lipoproteins in diabetic ketoacidosis: evidence for a change in high density lipoprotein composition during treatment. J. Lipid Res. 23(1):171-182. Pubmed |
||||
| World Health Organization (WHO) (2013). Diabetes estimates and Projections. Available at: http://www.who.int/diabetes/facts/en/ | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


