Full Length Research Paper
ABSTRACT
This research was designed to investigate antihyperglycaemic impact of aqueous extract of Moringa oleifera leaf on alloxan-induced diabetic male wistar rats. Diabetes is a metabolic disease linked to weakened sugar metabolism. Managing diabetes devoid of any adverse effect remains an issue to health system. Therefore, there is an increase in the search for better anti-diabetic medicine. M. oleifera leaves were air-dried, grinded, sieved and the aqueous extract was prepared. Twenty male wistar rats were used and these rats were grouped into four groups, five rats in each group. Group 1 and group 2 rats were diabetes induced groups treated with 100 and 400 mg/kg of aqueous extract of M. oleifera leaf respectively, group 3-diabetic untreated group, group 4-control group. Fasting blood glucose level, uric acid level and C-reactive protein level were measured by oxidase method, Uricase-PAP method and turbilatex method respectively. Results of this research work showed a significant increase in the fasting blood glucose level, uric acid level and C-reactive protein level in rats that were diabetic when compared with the control rats. However, treatment with 100 and 400 mg/kg of aqueous extract of M. oleifera leaf for a period of four weeks brought the fasting blood glucose level, uric acid level and C-reactive protein level toward the basal level significantly (P<0.05). The study showed that the aqueous extract of M. oleifera leaf has the potential to lower the elevated fasting blood glucose, uric acid and C-reactive protein levels toward the basal level in alloxan-induced diabetic male Wistar rats.
Key words: Hyperglycaemia, Moringa oleifera leaf, fasting blood glucose, uric acid, C-reactive protein, health system, metabolic disease.
INTRODUCTION
Diabetes mellitus (DM) is a multifactorial disease which is characterized by hyperglycaemia, lipoprotein abnor- malities (Scoppola et al., 2001) and altered intermediary metabolism of major food substances (Unwin et al.,2001).
Three major types of diabetes mellitus (DM) exist. Type 1 diabetes mellitus results from the inability of the body to generate insulin and is required of the individual to inject insulin or wear an insulin pump (Amed and Oram, 2016). This form was formerly known as insulin- dependent diabetes mellitus. Type 2 diabetes mellitus results from insulin resistance, a situation where the cells of the body cannot utilize insulin well, occasionally joined with total deficiency of insulin. This was formerly called non- insulin dependent diabetes mellitus. The third major type of diabetes mellitus is gestational diabetes; it happens when pregnant women who have no past history of diabetes start developing high level of blood sugar. Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secretion, cystic fibrosis- related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes. Diabetes can be managed by exercise, diet and pharmaceutical drugs which are either too expensive or have undesirable side effects or contraindications (Seuring, 2015). Types 1 and 2 are critical incurable conditions. Pancreas transplantation has been attempted with narrow accomplishment in type 1 diabetes mellitus, and gastric bypass surgery has been successful in many with morbid obesity and type 2 diabetes mellitus. Gestational diabetes usually resolves after delivery. Diabetes without proper management can cause many complications. Acute complications include hypo-glycaemia, diabetic ketoacidosis, or nonketotic hyperosmolar coma. Serious long- term complications include cardiovascular disease, chronic renal failure and diabetic retinopathy. Adequate management of diabetes is thus important as well as blood pressure control and lifestyle factors such as smoking and maintaining a healthy body weight (Lambert and Bingley, 2002).
The pathogenesis of diabetes mellitus and the possibility of its management by existing therapeutic agents without any side effects have stimulated great interest in recent years (Bailey, 1999). Management of diabetes without any side effects is still a challenge for the health care system. Therefore, there is an increased search for improved anti- diabetic drugs.
Few plant extracts used in traditional medicine for treating diabetes have received scientific scrutiny and the World Health Organization has recommended greater attention to the use of plant extracts (WHO, 1980). The present study was carried out to evaluate the anti- diabetic effect of aqueous extract of Moringa oleifera leaf in alloxan- induced diabetic male Wistar rats. M. oleifera is the most widely cultivated species of the genus Moringa, which is the only genus in the family Moringaceae. Its English common names include moringa, benzolive tree and West Indian ben (Makkar et al., 2007). The tree itself is rather slender, with drooping branches that grow to approximately 10 m in height. In cultivation, it is often cut back annually to 1- 2 m and allowed to re-grow so the pods and leaves remain within arm’s reach.
MATERIALS AND METHODS
Plant material
M. oleifera leaves were collected from the University Farm of Ladoke Akintola University of Technology, Ogbomoso of Oyo State. Identification was done at the Department of Biology (Botany option) of the Ladoke Akintola University of Technology, Ogbomoso. The leaves were dried at room temperature until they were free from moisture. The dried leaves were thoroughly grinded into powdery form using mortar and pestle and sieved. And the aqueous extract of M. oleifera leaf was prepared by dissolving ten grams of the powder in 40 ml of distilled water as crude extract.
Animals
Wistar rats weighing 100-120 g were used in this research work. The animals were maintained under laboratory conditions of humidity, temperature (23-25°C) and light 12 h light-dark cycle in the Animal House of College of Health Sciences, University of Ilorin, and allowed free accesses to grower mash and water ad libitum. The animals were acclimatized for two weeks. The principles of laboratory animal care guideline procedures were followed in the study (NIH publication revised, 1985).
Induction of diabetes
After fasting the animals for 12 h, the animals were given a single dose of intraperitoneal injection of freshly prepared alloxan solution using saline (0.9% (w/v) NaCl) as vehicle at a dose of 12 mg alloxan/100 g body weight (Bahnak and Gold, 1982). The rats were maintained on 5% glucose solution for next 24 h to prevent hypoglycaemia. The diabetic state was ascertained by high fasting blood glucose level above the normal. Symptoms of diabetes were observed within a week of alloxan injection.
Experimental design
Twenty male Wistar rats were used for this study. The rats were divided into four groups, each group consisting of five rats: Group 1, Diabetes induced group treated with 100 mg/kg of aqueous extract of M. oleifera leaf; Group 2, Diabetes induced group treated with 400 mg/kg of aqueous extract of M. oleifera leaf; Group 3, Diabetes induced untreated group and Group 4, Control group
Determination of fasting blood glucose level
Blood glucose levels were determined using a glucometer (Accu Chek Active) and test strips using glucose oxidase method (Sera Pak, USA).
Determination of uric acid level (Uricase PAP method)
Uricase transforms uric acid in the sample into Allantoin, Carbon dioxide (CO2) and Hydrogen peroxide (H2O2). By the action of Peroxidase (POD) and in the presence of phenol-derivative, DHBS (3,5-Dichloro-2- hidroxy-benzenesulfonic acid) and 4-aminoantipyrine, hydrogen peroxide give a coloured indicator reaction which can be measured at 520 nm. The increase in absorbance is proportional to the uric acid concentration of the sample (Fossati et al., 1980).
Uricase- PAP methodology: Linear up to 25 mg/dl, reconstituted reagent stable up to 30 days at 2-8°C.
Enzymatic determination of uric acid according to the following reactions;
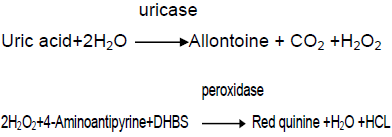
DHBS=3.5-Dichloro-2-Hydroxybenzenesulfonic acid.
Uric acid concentration (mg/dl) =Absorbance of sample/Absorbance of standard×6
Determination of C-reactive protein level
The reagent CRP-Turbilatex agglutination assay is a quantitative turbidimetric assay for measuring CRP in serum/plasma. Latex particles coated with specific anti-CRP are agglutinated when mixed with sample containing CRP. The agglutination causes an absorbance change, depending on the CRP contents of the sample that can be quantified by comparison from a calibrator of known CRP concentration (Sindhu et al., 2011). Turbilatex method with high sensitivity and specificity was used. The linear measurement was up to 150 mg/l.
CRP Concentration in mg/l= (A2-A1) sample/ (A2-A1) calibrator × calibrator concentration
Duration of treatment
Treatment started on the day the diabetic state was ascertained. Fasting blood glucose level was determined weekly for 4 weeks throughout the period of the experiment. The animals were then sacrificed using anaesthesia (chloroform) and blood samples were collected from the heart for biochemical analysis.
Analyses
Blood samples collected through cardiac puncture were used to analyze for Uric acid and C-reactive protein concentrations.
Statistical analysis
All values were expressed as  The differences were compared using one-way Analysis of Variance (ANOVA) followed by student t-test. P values with <0.05 were considered as statistically significant.
The differences were compared using one-way Analysis of Variance (ANOVA) followed by student t-test. P values with <0.05 were considered as statistically significant.
RESULTS
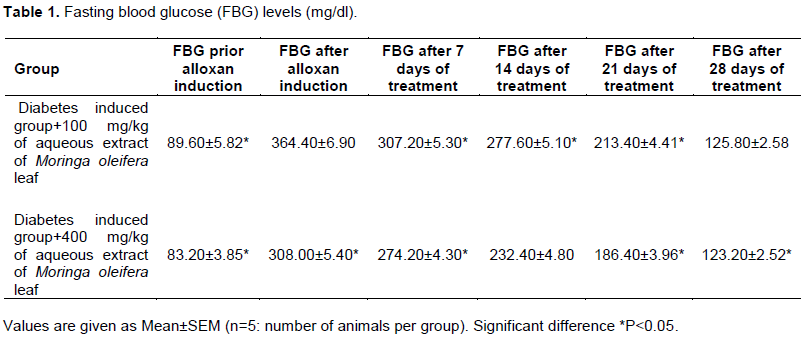
Fasting blood glucose levels increased significantly (P<0.05) 48 h after the induction of diabetes. But the fasting blood glucose levels were reduced toward the basal level by the aqueous extract of M. oleifera leaf significantly (P<0.05) (Table 1).
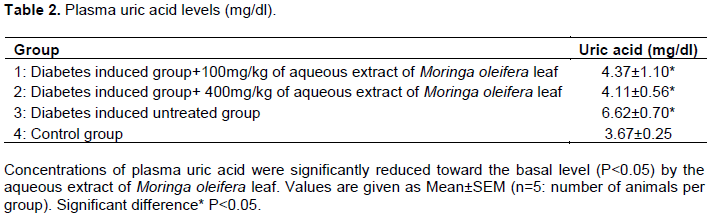
Concentrations of plasma uric acid were significantly reduced toward the basal level (P<0.05) by the aqueous extract of M. oleifera leaf (Table 2).
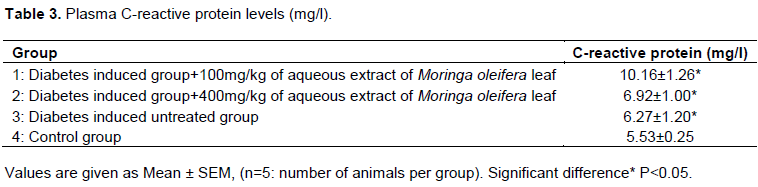
The aqueous extract of M. oleifera leaf reduced the concentration of C-reactive protein significantly toward the basal level (P<0.05) (Table 3).
DISCUSSION
Diabetes mellitus is a metabolic ailment linked to weakened glucose metabolism (Talloroth et al., 1990). Diabetes mellitus can be diagnosed by demonstrating any of the following; fasting plasma glucose level at or above 126 mg/dl (7.0 mmol/l), plasma glucose level at or above 200 mg/dl (11.1 mmol/l) 2 h after a 75 g oral glucose load as in a glucose tolerance test, random plasma glucose at or above 200 mg/dl (Sacks et al., 2011). According to the current definition, two fasting glucose measurements above 126 mg/dl (7.0 mmol/l) are considered diagnostic for diabetes mellitus. Alloxan induces diabetes by damaging the insulin secreting cells of the pancreas leading to hyperglycaemia (Szudelski, 2001). Alloxan, a β-cytotoxin destroys the β-cells of the islets of Langerhans of pancreas (Tyrberg and Anderson, 2001). This leads to a decrease in the endogenous insulin secretion and creates the ways for the decreased utilization of glucose by the tissue. This now results in elevation of blood glucose level above the normal physiological range.
In the present study, the anti-diabetic activity of the aqueous extract of M. oleifera leaf was evaluated in alloxan-induced diabetic male Wistar rats, using fasting blood glucose test. Expression of elevated fasting blood glucose level above the normal physiological range confirmed induction of diabetes in alloxan-induced experimental rats. Blood samples collected from the tail of the Wistar rats were used to determine the fasting blood glucose levels weekly throughout the period of the experiment. The glucose levels of the diabetic wistar rats treated with 100 mg/kg of the aqueous extract of M. oleifera leaf were lowered toward the basal levels significantly (P<0.05). Also, there was a significant decrease in the fasting blood glucose levels of the diabetic wistar rats treated with 400 mg/kg of the same extract (P<0.05). This agrees with the local uses of the leaves of the plant for the treatment of diabetes by traditional medicine practitioners. Therefore, this suggests the effectiveness of the aqueous extract of M. oleifera leaf in lowering the elevated fasting blood glucose levels in alloxan-induced diabetic rats as shown in Table 1.
The experiment lasted for four weeks after which the rats were sacrificed using chloroform, an anaesthesia and the blood samples were collected from the heart. Uric acid level was measured using Uricase- PAP method which is known to be sensitive and specific. Uric acid is the end product of purine metabolism and its normal physiological range is 3.6-8.3 mg/dl (Doring et al., 2008). Uric acid concentrations in blood plasma above and below the normal range are known as hyperuricemia and hypouricemia respectively and uric acid is being excreted by the kidneys. Increased levels of uric acid are found in gout, arthritis, impaired renal functions and starvation but decreased levels are found in yellow atrophy of the liver. High level of uric acid has been observed to be a risk factor for diabetes (Nakagawa et al., 2006). Hyperuricemia is associated with components of metabolic syndrome. A study has even suggested that fructose-induced hyperuricemia may play a pathogenic role in the metabolic syndrome (Nakagawa et al., 2006). In this study the uric acid level in diabetic rats treated with 100 mg/kg of the aqueous extract of M. oleifera leaf was reduced toward the basal level significantly (P<0.05). The same reduction toward the basal level was observed in diabetic rats treated with 400 mg/kg of the same extract.
C-reactive protein level was also estimated using turbilatex method with high sensitivity and specificity and this method can measure up to 150 mg/l of plasma C-reactive protein level. C-reactive protein is an acute protein synthesized by the liver in response to tissue injuries, bacterial and viral infections, inflammation and neoplasia. It is a member of the pentraxin family of proteins (Pepys and Hirschfield, 2003). High level of C-reactive protein level above the normal physiological range has been observed to be an independent risk factor for diabetes, cardiovascular disease such as hypertension (Dehghan et al., 2007). In this study, C- reactive protein level of the diabetic rats treated with 100 mg/kg of the aqueous extract of M. oleifera leaf was significantly reduced toward the basal level (P<0.05). The same reduction toward the basal level was observed in diabetic rats treated with 400 mg/kg of the same extract.
Mode of action by which aqueous extract of M. oleifera leaf brings about its hypoglycaemic effect may be by potentiating the insulin effect by increasing the insulin secretion from the beta cells of the pancreas. This study showed that aqueous extract of M. oleifera leaf has anti-diabetic effect on alloxan-induced diabetic male Wistar rats.
Further work could be done to investigate the active compounds responsible for the observed effect.
CONCLUSION
In conclusion, this study showed that the aqueous extract of M. oleifera leaf has antidiabetic effect. Few plants with potential therapeutic constituents such as fibers, sterols, saponins, polyphenols, flavonoids etc have been investigated for their antihyperlipidemic, antioxidant and antiatheroscelorotic properties. Thus, the phytochemical screening showed the presence of some substances such as alkaloids, saponins, tannis etc in the M. oleifera leaf. Further research may be carried out to investigate the exact constituents responsible for the observed effect.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Amed S, Oram R (2016). Maturity Onset Diabetes of the youn(MODY): Making the right diagnosis to optimize treatment. Canada Journal of Diabetes 40:449-454. |
|
|
Bahnak BR, Gold AH (1982). Effects of alloxan diabetes on the turnover of rat liver glycogen synthase comparison with liver phosphorylase. Journal of Biological Chemistry 257:8775-8780. |
|
|
Bailey CJ (1999). New Pharmacological approaches to glycaemic control. Diabetes Reviews 7:94-113. |
|
|
Dehghan A, Kardys I, Mact D (2007). "Genetic variation of C-reactive protein levels and incidence of diabetes". Journal of Diabetes 56(3):872-878. |
|
|
Doring A, Giegei C, Mehta D (2008). "SLC2A9 influences uric acid concentration with pronounced sex-specific effects". Nature Genetics 40(4):430-436. |
|
|
Fossati P, Prencipe L, Berti G (1980). Use of 3,5-dichloro-2-hydroxybenzenesulfonic acid/4-aminophenazone chromogenic system in direct enzymatic assay of uric acid in serum and urine. Journal of Clinical Chemistry 26:227. |
|
|
Lambert P, Bingley PJ (2002). What is type 1 Diabetes"? Medicine 30:1-5. |
|
|
Makkar HP, Francis G, Becker K (2007). "Bioactivity of phytochemical in some lesser-known plants and their effects and potentials application in livestock and aquaculture production system". Animal 1(9):1371-1391. |
|
|
Nakagawa T, Hu H, Zharikov S, Tuttle KR (2006). "A causal role for uric acid in fructose induced metabolic syndrome". American Journal Physiology Renal Physiology 290(3):F625-631. |
|
|
Pepys MB, Hirschfield GM (2003). C-reactive protein: a critical update. Journal of Clinical Investigation 11(12):1805-1812. |
|
|
Sacks DB, Arnold M, Bakris GL (2011). Executive summary: Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Journal of Clinical Chemistry 57:793-798. |
|
|
Scoppola A, Montecci FR, Mezinger G, Lala A (2001). Urinary mevalonate excretion rate in type 2 diabetes: Role of metabolic control. Journal of Atherosclerosis 156:357-361. |
|
|
Seuring T (2015). How Much Does Type 2 Diabetes Cost? PharmacoEconomics and Outcomes News 725(1):11-14. |
|
|
Sindhu S, Singh HK, Salman MT, Fatima J, Verma VK (2011). "Effects of atorvastatin and rosuvastatin or high-sensitivity C- reactive protein and lipid profile in obese type 2 diabetes mellitus patients". Journal of Pharmacology and Pharmacotherapeutics 2(4):2615. |
|
|
Szudelski T (2001). The mechanism of alloxan and streptozotocin action in beta cells of rat pancreas. Journal of Physiological Research 50(6):537-546. |
|
|
Tallroth GM, Lindgren G, Sternberg I, Agadh CD (1990). Neurophysiological changes during insulin-induced hypoglycaemia and in the recovery period following glucose infusion in type 1 diabetes mellitus and normal men. Diabetologia 33:319-327. |
|
|
Tyrberg B, Anderson A (2001). "Species differences in susceptibility of transplanted and cultured pancreatic islets to the beta cell toxin alloxan". General and Comparative Endocrinology 122(3):238-51. |
|
|
Unwin NE, Sobugwi E, Albert KGMM (2001). Type 2 diabetes: The challenge of preventing a global epidemic. Diabetes Int. pp. 11-48. |
|
|
WHO Expert Committee on Diabetes Mellitus (1980). Technical Report Series 646. World Health Organization, Geneva 61 p. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


