Full Length Research Paper
ABSTRACT
Obesity is associated with diverse morbidities, and elevated blood pressure has been suggested to be associated with increased body weight. This study therefore aimed to determine the relationship between obesity and elevated blood pressure among adolescent. This is a cross-sectional study. Consenting adolescents aged 10 to 18 years completed a pretested semi-structured questionnaire. Anthropometric parameters and blood pressure were measured using standard methods. Data were analysed using descriptive and inferential statistics. A total of 1000 adolescents were recruited with male to female ratio of 1:1. The mean age was 14.05±1.98 years. Early adolescence was predominant (43.3%). The prevalence of obesity was 1.3% while overweight was 4.1%. There was female preponderance for both overweight (53.7%) and obesity (53.8%). Sixty–nine (6.9%) had systolic hypertension while 50 (5.0%) had diastolic hypertension. Three (23.1%) obese and four (9.8%) overweight adolescents had statistically significant elevated systolic blood pressure in the hypertensive range (χ2 = 11.306, p = 0.015). One (7.7%) obese and four (9.8%) overweight subjects had statistically significant elevated diastolic blood pressure (χ2 = 9.803, p = 0.029). Routine screening for elevated blood pressure in schools is highly recommended among school-aged adolescents especially the obese and overweight.
Key words: Adolescents, blood pressure, Nigeria, obesity, overweight.
INTRODUCTION
Overweight and obesity have become a global epidemic contributing to the increasing burden of cardiovascular diseases, strokes, and premature deaths worldwide (Qorbani et al., 2013). Unfortunately, overweight and obesity are erroneously taken as a sign of good living in developing countries (Qorbani et al., 2013). It has been opined that obesity will almost always put the victims at health risks (de Onis et al., 2010). Obesity is caused by interaction of environmental factors, genetic predisposition and human behavior; and is associated with an increased risk of numerous chronic diseases, ranging from cardiovascular diseases, diabetes and other systemic diseases (Yang and Kelly, 2007).
Adolescents are older children with peculiar characteristics and a unique transitional stage marked by physical and psychological developments that span from puberty to legal adulthood (Ogden et al., 2012). Adolescence stage is characterized by lifestyle and behavioral changes and adoption of poor nutritional lifestyle at this stage could lead to malnutrition especially overweight and obesity which tends to track into adulthood (de Onis et al., 2010; Nguyen et al., 2010). Overweight and obesity are associated with diverse morbidities (de Onis et al., 2010), hence the need to forestall the rising trend. Complications of obesity in adolescents can occur both in the short term and in the long term. Some of these complications earlier thought to be long-term issues, which will only occur in adults, have now been shown to occur in children (Lackland, 2014).
The elevation of blood pressure with age is adduced to increasing peripheral resistance in arterial vessels and cardiac output (Gahagan, 2011). Cardiac output, stroke volume and blood volume all increase with increased body weight (Gahagan, 2011). Excessive body fat and hypertension are some of the major risk factors for coronary heart disease (Lackland, 2014). There is a linear trend in blood pressure with age and there is a positive correlation between body mass index and blood pressure (Lackland, 2014; Gahagan, 2011; Saunders et al., 2013).
Many studies have been done both in developed and some developing countries in order to explore the association between overweight/obesity and blood pressure (Nwaiwu and Ibe, 2014; Oduwole et al., 2012). Some of these studies established a strong relationship between elevated blood pressure and obesity (Qorbani et al., 2013; de Onis et al., 2010). However, the association between elevated blood pressure and obesity has not been thoroughly studied among adolescents in Nigeria. This study, therefore, attempted to document the burden of overweight and obesity as well as determine the relationship between overweight/obesity and blood pressure among school-aged adolescents in Owo Local Government Area, Nigeria.
MATERIALS AND METHODS
The study was conducted among secondary school students in Owo Local Government, Ondo State, Nigeria. Owo is located in South-western Nigeria, at the southern edge of the Yoruba Hills and at the intersection of roads from Akure, Kabba, Benin City and Siluko. Owo Local Government lies on longitude 5° 35’ E and latitude 7° 11’ N with a population of 218,886 and it has eleven wards which cut across Owo and surrounding towns (Aralepo, 2013).
This is a cross-sectional school-based study conducted between 5th of April, 2017 and 30th of June, 2017. Ethical approval with registration number FMC/OWO/380/VOL.XLVI/139 was obtained from the Federal Medical Centre, Owo, Ondo-State. Permission was obtained from the principals/proprietress of selected schools. Written informed consent was obtained from the parents/guardians of each eligible child and assent was also obtained from each recruited child. The respondents were assured of the confidentiality of the information given and the data collected were entered and kept in a password protected computer.
One thousand school-aged adolescents aged 10–18 years were recruited for the study using a multistage sampling method. The number allocated to each group of students was determined using the formula n/N × 1,000, where n is the number in each group and N is the total number of students (Suresh and Chandrashekara, 2012). There were 33 secondary schools in Owo LGA, comprising 18 public and 15 private secondary schools. Consenting adolescents filled a pretested semi-structured questionnaire which was distributed consecutively during the break period and was filled at their convenience. World Health Organization classification of adolescents was used in classifying the adolescents into early (10 – 13 years), middle (14 – 16 years) and late (17–18 years) adolescence (Christie and Viner, 2005).
Height (in centimeters) was measured with Leicester® stadiometer. The subjects stood erect, barefooted, feet together, chest out and looking horizontally straight ahead with the heel, buttock, and occiput touching the vertical plane of the instrument (Frankfort plane) (McIntosh and Campbell, 2003). The measurement was taken to the nearest 0.1 cm.
Weight (in kilograms) was measured using the analog weighing scale by SECA®, Great Britain with the participants wearing only school uniform and no shoes. The scale was standardized before each measurement by ensuring the indicator returned to the zero mark. Also, commercially sold metals with known weights were used at weekly intervals for standardization and readings were measured to the nearest 0.1 kg.
Body Mass Index (BMI) was estimated by dividing the measured weight in kilograms by the square of the height in meters (kg/ m²). The BMI was grouped into underweight, BMI below 5th percentiles; normal weight, BMI from 5th to 84th percentiles; overweight, BMI of 85th and less than 95th percentiles and obesity, BMI of equal to or greater than 95th percentile using Centers for Disease Control and Prevention (CDC) BMI-for-age chart (Magarey et al., 2003).
Resting blood pressure (mmHg) was taken for all the subjects using the right arm after a ten- minute resting period having allowed the subjects to sit with legs uncrossed and feet standing on a firm surface (National Institute of Health, 2005). An Accoson® mercury sphygmomanometer with an appropriate bladder cuff was applied evenly and firmly about 2.5 cm above the antecubital fossa. The cuff bladder width was 40% of the arm circumference measured at a point midway between the acromion and the olecranon and the bladder length covering 80 to 100 percent of the arm circumference. The cuff was inflated rapidly and deflated slowly. A Littman’s classic II Pediatric stethoscope bell was used for auscultating the Korotkoff sounds during deflation.
Systolic and diastolic blood pressure values were taken at the 1st and 5th Korotkoff sounds respectively. All subjects had two readings taken 5 min apart after the initial blood pressure trial run which was to secure subjects’ confidence. The average reading was then taken to the nearest 2 mmHg. Blood pressure percentile was deduced and was then classified according to the recommendations of the National Blood Pressure Education Program into normal (<90th percentile); pre-hypertension (≥ 90th to < 95th percentile); hypertension (≥ 95th percentile) (National Institute of Health, 2005).
Data were analyzed using the statistical package for social sciences (SPSS) software version 20 (SPSS Chicago Inc., IL, USA, Released 2011). Body Mass Index and BMI percentiles were generated using the Nutstat component of the Epi Info software (Jebb et al., 2004). The software uses 2000 CDC growth charts for boys and girls. Values and the results were expressed as means, standard deviation for continuous variables and as proportions and percentages for categorical variables. Data were compared among the non-overweight, overweight and obese using bar chart, tables and figures. Inferential statistics was done using Chi-square and Student’s t-test for categorical and continuous variables respectively. Correlation of blood pressure with overweight and obesity was also done to know the strength of association. Logistic regression was used to examine the association between overweight and obesity and the blood pressure that were significantly associated with it. Analyses with probability value p less than 0.05 were taken as statistically significant.
RESULTS
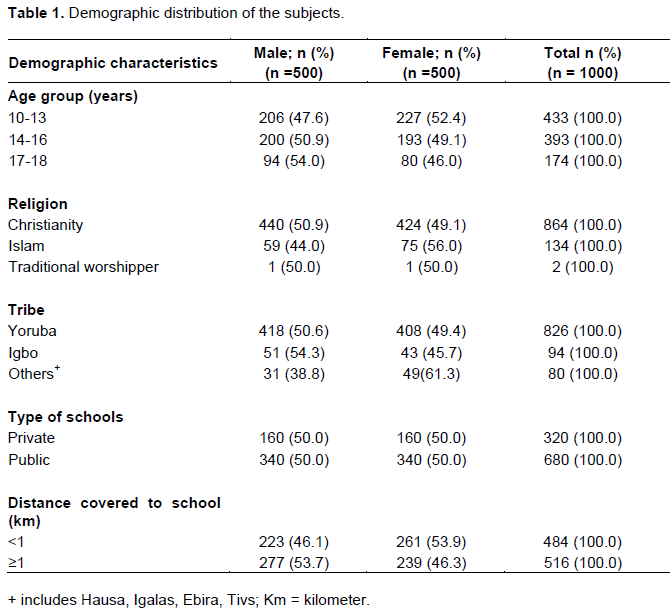
A total of 1000 school-aged adolescents were recruited during the study period comprising 500 each of males and females giving a male to female ratio of 1:1. Table 1 shows the demographic characteristics of the adolescent. All the subjects recruited were aged between 10 and 18 years with a mean ± standard deviation (SD) of 14.05±1.98 years while the modal age was 17 years. Four hundred and thirty–three (43.3%) of the subjects were aged 10 – 13 years, of whom 206 (47.6%) were males and 227 (52.4%) were females. Six hundred and eighty (68.0%) of the subjects attended public schools while the remaining were from private schools.
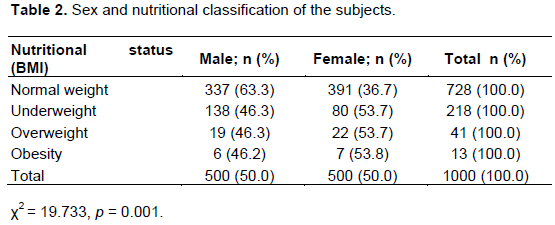
Nutritional classification of the subjects showed that the prevalence of overweight was 4.1% while that of obesity was 1.3%. Twenty-two (53.7%) of the 41 overweight subjects were females while seven (53.8%) of the 13 obese subjects were females. This gender-related difference in the prevalence of overweight and obesity was statistically significant (χ2 = 19.733, p = 0.001), as seen in Table 2.
The mean systolic blood pressure (SBP) for the 1000 subjects was 107.20±13.04 mmHg with the range of 52 - 165mmHg and mean diastolic blood pressure (DBP) was 68.33± 10.46 mmHg with the range of 40 – 100mmHg. The mean SBP was significantly higher among females (108.48±12.94 mmHg) with the range of 52-165mmHg compared to males (105.93±13.02 mmHg) with the range of 62-160mmHg (p = 0.002, 95% CI:12.31-13.84). The mean DBP was higher among females (68.92±10.44 mmHg) with the range of 41-100mmHg compared to males (67.73±10.47 mmHg) with the range of 40-100 mmHg; however this was not statistically significant (p = 0.072; 95% CI: 10.05-10.91).
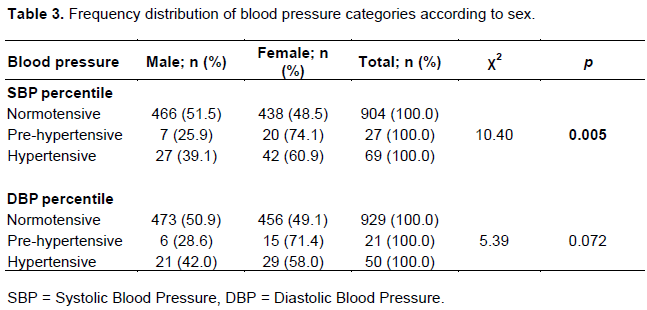
Sixty-nine (6.9%) of the subjects had systolic hypertension while 50 (5.0%) had diastolic hypertension. As seen in Table 3, for the frequency distribution of blood pressure categories of the study subjects according to sex, a significantly higher percentage of females had SBP values in the range of pre hypertension and hypertension than males (χ2 = 10.40, p = 0.005). However, the higher proportion of females with DBP values in the range of prehypertension and hypertension compared to males was not statistically significant (χ2 = 5.39, p = 0.072).
The mean SBP and DBP was significantly higher among male subjects who were pre-hypertensive (p = 0.006 and p = 0.025 respectively), as shown in Table 4.
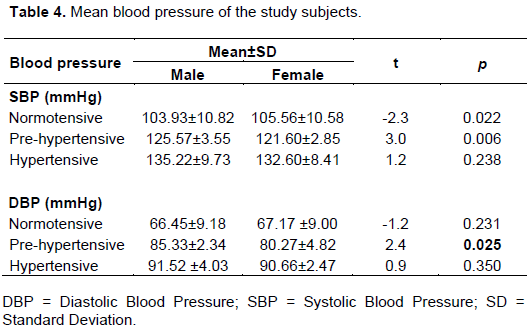
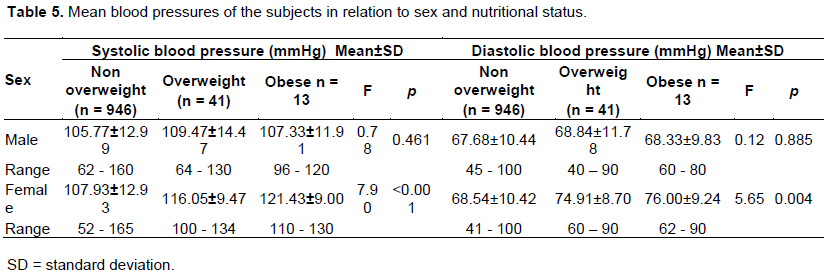
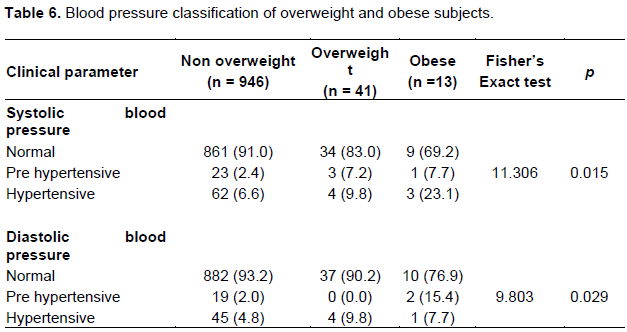
Table 5 shows the mean blood pressure of the study subjects in relation to sex and nutritional status. The mean systolic and diastolic blood pressure values of overweight and obese females were significantly higher than their non-overweight counterparts (p <0.001 and p = 0.004 respectively). The blood pressure classification of overweight and obese subjects is seen in Table 6. Sixty-nine (6.9%) of the subjects had elevated systolic blood pressure (in hypertensive range). Three (23.1%) of obese subjects and 4 (9.8%) of overweight subjects had statistically significant elevated systolic blood pressure in the hypertensive range (χ2 = 11.306, p = 0.015). Among the 21 participants with pre-hypertensive diastolic blood pressure, 9.5% were obese and none was overweight. One (7.7%) of 13 obese subjects and 4 (9.8%) of 41 overweight subjects had hypertensive diastolic blood pressure (χ2 = 9.803, p = 0.029).
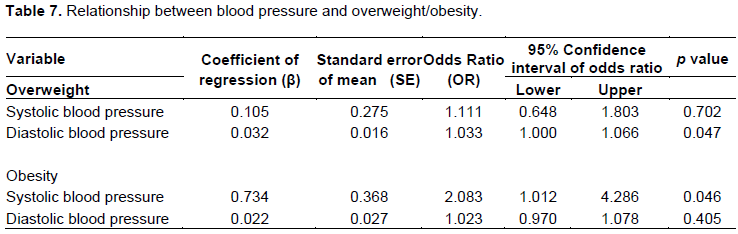
The diastolic blood pressure had a statistically significant association with overweight from bivariate analysis (OR=1.0; CI: 1.00-1.06; p = 0.047). Obese adolescents were twice likely to have hypertensive systolic blood pressure when compared with non-overweight counterparts (OR = 2.08; 95% CI: 1.01 – 4.29; p= 0.046) (Table 7).
DISCUSSION
The prevalence of overweight in this study was 4.1% while that of obesity was 1.3%. The prevalence was higher than what was documented in Ile-Ife with a prevalence of 2.8% and 0.3% for overweight and obesity respectively (Adegoke et al., 2009). The higher prevalence in the present study could be due to the inclusion of only adolescents in this present study unlike the Ile-Ife where children of all age groups were included. Overweight/obesity are more common among adolescents (Lifshitz, 2008), therefore, inclusion of children outside the adolescent age group is likely to have a lowering effect on the prevalence of obesity that will be obtained. Similarly, the study in Ile-Ife was done over a decade ago therefore, the rising trend of overweight and obesity in the country and globally could also explain the higher prevalence in the current study.
The prevalence of obesity in this study was markedly overweight/obesity in our study could be related to the rapid growth that occurs during puberty which is earlier and more pronounced in females (Soliman et al., 2014). In addition, it has been suggested that the female hormone estrogen inhibits thyroid hormone thereby reducing basal metabolism and encourage fat storage (Grantham and Henneberg, 2014). Estrogen also modulates the hypothalamic hormones through the activity of leptin thus stimulating appetite and resulting in positive energy balance (Grantham and Henneberg, 2014).
In this study, the mean systolic and diastolic blood pressure values were significantly higher among overweight and obese subjects. Also worthy of note is that among the female subjects, the mean blood pressure values were higher in those overweight and obese. This is similar to the observations from previous study (Oduwole et al., 2012). Higher blood pressure values are not unexpected in overweight and obese adolescents because in individuals with excess body fats there is deposition of fats on the blood vessel wall resulting in thickening of the wall thereby increasing the total peripheral resistance thus increasing the blood pressure. Also, leptin and other adipokines produced by the adipocytes cause the activation of sympathetic nervous system leading to elevated blood pressure (Gahagan, 2011).
The prevalence of systolic hypertension was highest among obese subjects in this study. This was similar to previous study where more obese subjects were found to have hypertensive systolic blood pressure (Oduwole et al., 2012). In this study, obese participants were twice more likely to have hypertensive systolic blood pressure when compared to their non-overweight participants. This finding was similar to the study where elevated blood pressure is three-times higher in obese children compared with their non-obese peers (Sorof and Daniels, 2002). The implication of this finding is that routine blood pressure measurement should be encouraged among adolescents especially in those who are obese.
Elevated blood pressure has been reported as independent factors associated with overweight and obesity (Barriuso et al., 2015). Some of these associations were seen in the present study with elevated systolic blood pressure being independent associated factors with obesity while elevated diastolic blood pressure was independently associated with overweight. Therefore, clinicians should screen for elevated blood pressure among overweight and obese adolescents. The limitation of this study was the blood pressure values obtained were point measurements, so persistence of elevated blood pressure could not be ascertained.
In conclusion, the prevalence of obesity and overweight in this study demonstrated its presence among the school-aged adolescents in Owo, Ondo-state despite being a low-middle-income State. The systolic and diastolic blood pressure was elevated among the overweight/obese adolescents which calls for attention and urgent intervention so as to alleviate the long-term damage this might cause. Similarly, the association between hypertension and overweight/obesity is alarming and calls for policy making for the reduction of obesity and overweight among the adolescent. There is also the need for routine blood pressure evaluation among the overweight/obese children for early detection and management of hypertension.
CONFLICT OF INTERESTS
The authors declare that there are no conflicts of interest, financial or otherwise in the publication of this paper.
ACKNOWLEDGEMENT
The authors appreciate the effort of Dr. J.A.O Okeniyi, of the Department of Paediatrics and Child Health, Obafemi Awolowo University, Ile-Ife, Osun-State for proofreading of the paper.
REFERENCES
|
Adegoke SA, Elusiyan JBE, Olowu WA, Adeodu OO (2009). Relationship between body mass index and blood pressure among Nigerian children aged 6-18 years. Niger Endocrine Practice 3:35-41. |
|
|
Aralepo AJ (2013). A synopsis of Owo history. (Eds.), Lagos: Iadmo press, pp. 1-5. |
|
|
Barriuso L, Miqueleiz E, Albaladejo R, Villanueva R, Santos JM, Regidor E (2015). Socioeconomic position and childhood adolescent weight status in rich countries: A systematic review, 1990-2013. BMC Pediatrics 15(1):129-132. |
|
|
Christie D, Viner R (2005). Adolescent development. British Medical Journal 350:301-304. |
|
|
de Onis M, Blossner M, Borghi E (2010). Global prevalence and trends of overweight and obesity among preschool children. The American Journal of Clinical Nutrition 92(5):1257-64. |
|
|
Gahagan S (2011). Overweight and obesity. In. Behrman RE, Kliegman RM, Stanton BF, St Geme III JW, Schor NF (Eds.), Nelson Textbook Paediatrics. Philadelphia: W.B. Saunders, pp. 179-188. |
|
|
Grantham JP, Henneberg M (2014). The estrogen hypothesis of obesity. PLoS One 9(6):99776-83. |
|
|
Hamaideh SH, Al-Khateeb RY, Al-Rawashdeh AB (2010). Overweight and obesity and their correlates among Jordanian adolescents. Journal of Nursing Scholarship 42(4):387-394. |
|
|
Jebb SA, Rennie KL, Cole TJ (2004). Prevalence of overweight and obesity among young people in Great Britain. Public Health Nutriton 7(3):461-465. |
|
|
Kimani-Murage EW, Pettifor JM, Tollman SM, Klipstein-Grobusch K, Norris SA, Kahn K (2011). Predictors of adolescent weight status and central obesity in rural South Africa. Public Health Nutrition 14(6):1114-1122. |
|
|
Lackland D (2014). Racial differences in blood hypertension: Implication for high blood pressure management levels of adolescents. American journal of the medical sciences 348(2):135-138. |
|
|
Lifshitz F (2008). Obesity in children. Journal of Clinical Research in Pediatric Endocrinology 1(2):53-60. |
|
|
Magarey AM, Daniels LA, Boulton TJ, Cockington RA (2003). Predicting obesity in early adulthood from childhood and parental obesity. International Journal of Obesity 27(4):505-513. |
|
|
McIntosh N, Campbell AGM (2003). Adolescent medicine. In. Forfar A (Eds.), Textbook of Pediatrics. Edinburgh: Churchill Livingstone, pp. 1757-1768. |
|
|
National Institute of Health (2005). The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. National Institutes of Health 5267:1-60. |
|
|
Nguyen DM, El-Serag HB, Cammarota G, Haley AP, Styriak I, Gaspar L (2010). The Epidemiology of Obesity. Gastroenterology Clinics of North America 39(1):1-7. |
|
|
Nwaiwu O, Ibe BC (2014). Body mass index of children aged 2-15 years in Enugu Nigeria. Nigerian Journal of Paediatrics 41(3):194-198. |
|
|
Oduwole AO, Ladapo TA, Fajolu IB, Ekure EN, Adeniyi OF (2012). Obesity and elevated blood pressure among adolescents in Lagos, Nigeria: a cross-sectional study. BMC Public Health 12(1):616. |
|
|
Ogden CL, Carroll MD, Kit BK, Flegal KM (2012). Prevalence of obesity in the United States, 2009-2010. National Centre for Health Statistics Data Brief 82:1-8. |
|
|
Qorbani M, Kelishadi R, Farrokhi-khajeh-Pasha Y, Motlagh M, Aminaee T, Ardalan G, Asayesh H, Shafiee G, Taslimi M, Poursafa P, Heshmat R, Larijani B (2013). Association of Anthropometric measures with cardiovascular risk factors and metabolic syndrome in normal weight children and adolescents. Obesity Facts 6:483-492. |
|
|
Saunders TJ, Tremblay MS, Després JP, Bouchard C, Tremblay A, Chaput JP (2013). Sedentary Behavior, Visceral Fat Accumulation and Cardiometabolic Risk in Adults: A 6-Year Longitudinal Study from the Quebec Family Study. PLoS One 8(1):132-6. |
|
|
Soliman A, Sanctis V, Elalaily R, Bedair S (2014). Advances in pubertal growth and factors influencing it: Can we increase pubertal growth? Indian Journal of Endocrinology and Metabolism 18(7):53-55. |
|
|
Sorof J, Daniels S (2002). Obesity and hypertension in children: A problem of epidemic proportions. Hypertension 40:441-447. |
|
|
Suresh KP, Chandrashekara S (2012). Sample size estimation and power analysis for clinical research studies. Journal of Human Reproductive Sciences 5:7-13. |
|
|
Yang W, Kelly T (2007). Genetic epidemiology of obesity. Epidemiologic Review 29:49-61. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


