Full Length Research Paper

ABSTRACT
The aim of this study was to determine the prevalence of early childhood caries (ECC) and factors leading to it among 71 months of age children or younger in Karachi, Pakistan. ECC is a preventable chronic disease affecting infants and children worldwide. The early detection of ECC can reduce pain and life threatening conditions and help growth and development of infant and children. A cross-sectional study was conducted in Karachi, Pakistan. About 650 mothers of children (71 months of age or younger) were randomly selected and interviewed using a pretested semi-structured questionnaire. The dental examination was performed by the dentist, who was calibrated against a standard examiner using World Health Organization (WHO) criteria. The data was entered and analysed using statistical package for social sciences (SPSS) version 16 software. ECC was found in 23.5% of children with mean decayed missing and filled teeth (dmft) of 0.67. The factors identified were age of the child, mother educational and occupational status, sweetened drink consumption at night and not utilizing routine dental health care services. This study concluded that high proportion of ECC was found among children (71 months of age children or younger) and factors identified were all preventable and needs attention to promote dental health education and routine dental visits.
Key words: Early childhood caries (ECC), mothers, risk factors, children 6 to 71 months of age.
INTRODUCTION
Early childhood caries (
The etiology of ECC is multi-factorial, and the exact interplay of risk factors in different communities found was controversial. There are many risk factors which were found significantly associated with ECC. The most important is consumption of sugary snacks, sweetened drinks, and consumption of sweetened feeding bottles at night (Liu et al., 2007). Breastfeeding or bottle feeding at night is a major risk factor for development of dental caries (Van Palenstein et al., 2006). A study conducted in Japan showed that nocturnal breastfeeding and snacking habits are associated with early childhood caries (Nakayama and Mori, 2015). According to American Academy of Pediatric Dentistry (AAPD), prolonged and repetitive breastfeeding and bottle feeding without proper oral hygiene were reported to be a devastating risk factor for ECC. Therefore, parents are encouraged to feed infants through drinking cups from first year of life and stop bottle feeding between 12 and 14 months (American Academy of Pediatrics, 2008, 2009). The other reported risk factors for ECC were poverty, racial minorities, single mother, parent’s level of education, mothers’ illiteracy, enamel hypoplasia due to prenatal and perinatal malnutrition or undernourishment, poor oral hygiene, fluoride insufficiency and greater preference for sugary foods (Chu, 2006).
The most effective approach for the control of early childhood caries is early detection and prevention. The restorative treatment can be avoided by preventive strategies. It is necessary to provide expectant mothers dental health education and counseling regarding prevention of ECC. The routine dental examination of children should be emphasized during counseling of mothers as late utilization of dental health care facility is the biggest problem faced by dentist for the control and prevention of early childhood caries. It is reported that few parents take their children to the dentist at the age of three years which usually prevents early detection of ECC (Drury et al., 1999). This study was designed to determine prevalence of ECC and factors leading to it among 71 months age group of children or younger in Karachi, Pakistan. There is scarcity of data on this important problem and this would help in designing preventive dental health education strategies for ECC.
METHODOLOGY
A cross-sectional study was conducted in Gulberg Town of Karachi, Pakistan from October 2009 to 2010. It has a total population of 453,490 according to the consensus conducted in 1998. A sample size of 650 was calculated by taking the proportion of ECC to be 19.2% (Tyagi, 2008), confidence interval of 95%, margin of error to be 3%, design effect to be 1.0% and power of test to be 80%. The sampling was performed in two stages; in the first phase, four union councils out of a total of eight were selected randomly through lottery method. In the second phase, list of households in each selected union council was obtained from town administration and random number table was generated and required sample size was achieved by taking equal proportion of participants from each selected union council. The selected households were visited and the child (71 months of age or younger) age was examined for the presence of ECC and the mother interviewed through administering a questionnaire.
The dental examination was performed by the dentist, who was calibrated against a standard examiner. Inter-examiner reliability was 92% agreement giving kappa = 0.85. The intra-examiner reliability was 97% in agreement with kappa = 1.0. Consent was obtained at the time of interview and clinical examination of the child. Clinical examination of the child was performed by dental surgeon under natural light at knee-to-knee position with an autoclavable mouth mirror using disposable gloves and mask and a gauze to dry the tooth. The WHO diagnostic criterion was used for diagnosis of dental caries (World Health Organization [WHO], 2003). ECC was diagnosed according to the WHO criteria; presence of caries on the labial or lingual surfaces of at least two maxillary incisors with the absence of caries in mandibular incisors (Azevedo et al., 2005; Dini et al., 2000). The data was entered and analysed using the Statistical Package for Social Science (SPSS) version 16 software. Descriptive statistics was used to describe socio-demographic characteristics and study variables (risk factors) were computed. The association between dependent variable, that is, early childhood caries with independent variables (risk factors) were determined through multi binary logistic regression analysis using the logistic model and 95% confidence intervals. The P-value of less than 0.05 has been considered significant.
Ethical consideration
Ethical approval for the study was obtained from the Institutional Review Board of Dow University of Health Sciences. Furthermore, a written consent for participation in the study was obtained from the caregivers of children.
RESULTS
Descriptive statistics
Out of 650 guardians, 97.5% were mother and 2.5% were father of the child examined. The mean age of the mothers was 29 years (SD ± 5.4). Among 650 children, 46.5% were boys and 53.5% were girls. The mean age of the child was 45 months (SD ± 16.8). About 31% guardians were having four or more than four children. Regarding educational status, 40.9% mothers and 25.8% fathers were found illiterate. About 21.6% women were working on daily wages, while 62% were earning less than 10,000 Pakistani rupees (Table 1). The prevalence of ECC was found to be 23.5% with mean dmft of 0.67. About 46% children had dmft positive in their whole arch (Table 2).
Univariate analysis
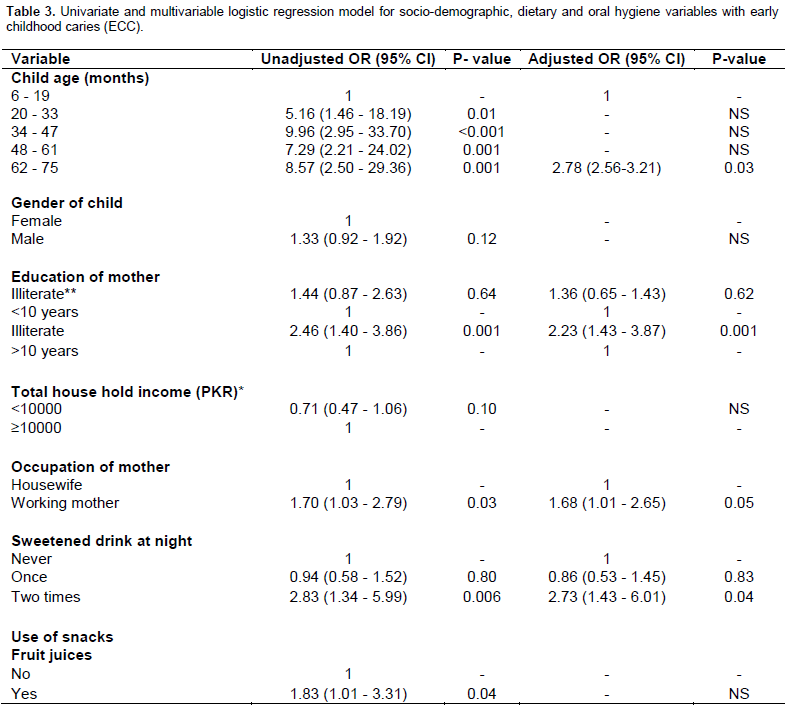
The univariate analysis showed that increase in age of the child showed statistically significant association with ECC. Gender did not show any significant association with ECC. The odds of having early childhood caries in children of illiterate mothers were two times (OR = 2.46, CI = 1.40 to 3.86) more as compared to mothers who had <10 years of education. The odds of having early childhood caries in children of working mothers were more as compared to non-working mothers (OR = 1.70, CI = 1.03 to 2.79). The dietary factors related to ECC showed that odds of having early childhood caries among children who were having sweetened drink at night were 2 times (OR = 2.83, CI = 1.34 to 5.99) more as compared to children who never consumed sweetened drink at night. The odds of having ECC in children of mothers who had stopped breastfeeding after 6 months (OR = 2.45, CI = 1.76 to 3.92) and after 18 months (OR = 3.12, CI = 2.38 to 4.19) were significantly associated with ECC. The other dietary factors which showed significant association in univariate analysis were consumption of fruit juices (OR = 1.83, CI = 1.01 to 3.31), biscuits (OR = 2.21, CI = 1.43 to 3.76), and nursing bottle (OR = 1.56, CI = 1.02 to 2.52). The frequency of brushing did not show significant association with ECC. The routine dental visits showed significant association; children who did not visit dentist regularly were having ECC two times more (OR = 2.87, CI = 1.06 to 7.85) as compared to those who visit dentist regularly (Table 3).
Multivariate analysis
After adjusting socio-demographic variables, the odds of having early childhood caries in children of illiterate mothers were two times (AOR = 2.19, CI = 1.38 to 3.87) more as compared to mothers who had >10 years of education. The odds of having early childhood caries in children of working mothers were more (AOR = 1.70, CI =1.03 to 2.79) as compared to housewives. The odds of having early childhood caries among children who consumed sweetened drink at night showed significant association (AOR = 2.83, CI = 1.34 to 5.99) as compared to children who did not consume sweetened drink at night. The children of mothers who breast fed for 18 to 24 months had ECC three times more (AOR = 3.12, CI = 2.38 to 4.19) as compared to those who never breast fed. The mothers who did not visit dentist regularly, their children had ECC two times more (AOR = 2.87, CI = 1.06 to 7.85) as compared to children who had visited dentist regularly (Table 3).
DISCUSSION
High prevalence of ECC is reported worldwide. It has become a great public health challenge to control and prevent due to its complex etiology and involvement of multiple risk factors. This study reported prevalence of ECC (23.5%) which is consistent with the findings of research studies conducted in Iran and India (Askarizadeh and Siyonat, 2004; Mahjabeen et al., 2006). The dmft scores did not show any difference in gender and similar results are reported from studies conducted in Mexico and China (Segovia-Villanueva et al., 2006; Du et al., 2007). The children from low socio economic group consumed more sugary foods and did not possess healthy dental practices, for example use of toothbrush, toothpaste and attending routine dental health clinics. The low socio economic status and income is considered to be one of the most important risk factor for ECC. A study conducted in Australia showed that guardian income is strongly associated with children oral health (Wyne and Khan, 1998). Our study did not prove any statistical association of income and ECC, and this is consistent with the findings of a study conducted in Riyadh, Saudi Arabia (Al Ghanim et al., 1998).
Several studies from various part of the world reported that consumption of beverages and sweetened milk is a profound predictor of caries (Al Ghanim et al., 1998; Warren et al., 2008). These findings are consistent with the findings of our study. But contrary to these findings, another study reported that it may not be the sole reason and there are other factors involved such as time of milk consumption and its content; sweetened or non-sweetened (Johansson et al., 2010). An interesting and favourable finding of this study is that most of the children consumed milk or other liquids in glass rather than in bottle at bed time. This reduces the chances of dental caries and helps the parents to brush their child’s teeth prior going to bed. It is found helpful in breaking the habit of using a feeding bottle which is usually advocated for children up to 12 months of age (Marshall et al., 2007). Most of the mothers preferred to continue breastfeeding from twelve to twenty four months of child age while only few mothers stopped breastfeeding after six months. A study conducted in Japan showed that nocturnal breastfeeding and snacking habits are associated with ECC (Nakayama and Mori, 2015). Another study conducted in Brazil reported that children who did not breastfeed for more than 24 months of age are at risk of ECC (Dini et al., 2000).
This study showed that caries status is significantly associated with children who did not breastfeed for six months or more than eighteen months of age. This is consistent with the findings of a Hispanic study that children who did not breastfeed are found more at risk of oral diseases and other systemic diseases like gastro intestinal (GI) infections, asthma, atopic disease and diabetes mellitus (Rosenblatt and Zarzar, 2004). In our study, consumption of fruit juices and biscuits are found significantly associated with ECC. Majority of the children reported consumption of different types of snacks during the day and choice depends on the availability and affordability of the snacks. Most preferred type of snacks reported are chips, flavoured milk, juices, chocolates, biscuits, instant noodles and potato fries. These findings are consistent with the findings of studies conducted in US and Australia (Johansson et al., 2010; Hallett and O’Rourke, 2006). Another research conducted on pre-school children reported similar findings regarding consumption of beverages, biscuits and chocolates (Tsai et al., 2006).
.png)
Proper brushing technique plays an important role in prevention of ECC. In this study, only few children reported brushing teeth once or twice a day. Majority reported that they never brushed their teeth. Only few children reported some alternatives for example miswak or a chewing stick (dandasa) for cleaning teeth. Similar findings are reported by a study conducted in Taiwan (Pacey et al., 2007, 2008). The parent’s education and counselling is very important for maintenance of oral hygiene of their children. If early protective and preventive methods are not taken, then it leads to plaque and multiple cavities formation and there is increased risk of other dental problems. Similarly, routine dental health care utilization is an important strategy which is neglected by most of the parents. The results of this study showed that majority of parents did not take their children to dentist for routine check-up. The parents usually take their children to dentist when the child complaint of pain or some other dental problem. The reasons reported are access to dental health care service, unaffordability; and in parents opinion routine visits are not important.
.png)
In this study, majority of participants were less educated and belong to low income group. Several studies reported similar findings related to routine dental health care utilization (Iida et al., 2007; Nunn et al., 2009; Adair and Popkin, 2005). A reporting bias might be probable regarding caregivers response to the use of glass for child’s beverage or milk consumption as well as recognition of ill effects of leaving nipple in child’s mouth and avoidance of such practices. Hence, there is a liable chance that such ratios could have been more than revealed. There are few limitations of this study, for example there is likelihood of recall bias among mothers, especially of older child and his or her breastfeeding practices at the time when the child was young. Oral hygiene and plaque levels of toddlers were not calibrated for the study purpose. The ECC examination was entirely visual and lacked radiographic proof to second the visual findings because of shortage of capital resources. This might have led to underestimation of true ECC experience in the defined population.
CONCLUSION
This study concluded that high proportion of ECC was found among children (71 months of age or younger) and factors identified were child age, mother’s level of education, mother’s occupation and time of cessation of breastfeeding, and consumables like fruit juices and biscuits are all preventable.
RECOMMENDATION
This study recommended that oral health awareness programmes should be planned for the guardians especially for mothers and there is need to pay attention for promoting dental health education and routine dental visits so that ECC can be early detected. The program should be focused on preventive interventions to reduce the burden of ECC.
ACKNOWLEDGEMENTS
The authors are thankful for the guidance and tremendous support of Professor Haleem of Community Dentistry. They also pay gratitude to the children who cooperated graciously and their parents for their involvement in this research.
CONFLICTS OF INTEREST
The authors declare that they have no competing interest.
REFERENCES
|
Adair LS, Popkin BM (2005). Are child eating patterns being transformed globally? Obes. Res. 13:1281–1299. Crossref |
||||
|
Al Ghanim NA, Adenubi JO, Wyne AA, Khan NB (1998). Caries prediction model in pre-school children in Riyadh, Saudi Arabia. Int. Crossref |
||||
|
Albert RJ, Cantin RY, Cross HG, Castaldi CR (1988). Nursing caries in the Inuit children of the Keewatin. J. Can. Dent. Assoc. 54:751-758. Pubmed |
||||
|
American Academy of Pediatric Dentistry; American Academy of Pediatrics (2008, 2009). Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. Pediatr. Dent. 30(7 Suppl):40-43. Pubmed |
||||
|
Askarizadeh N, Siyonat P (2004). The prevalence and pattern of nursing caries in preschool children of Tehran. J. Indian Soc. Pedod. Prev. Dent. 22(3):92-95. Pubmed |
||||
|
Azevedo TD, Bezerra AC, de Toledo OA (2005). Feeding habits and severe early childhood caries in Brazilian preschool children. Pediatr. Dent. 27:28-33. Pubmed |
||||
| Burt BA, Eklund SA (1999). Dentistry, dental practice, and the community. 5th ed. Philadelphia: Saunders. | ||||
|
Carino KM, Shinada K, Kawaguchi Y (2003). Early childhood caries in northern Philippines. Community Dent. Oral Epidemiol. 31:81-89. Crossref |
||||
|
Chu S (2006). Early childhood caries: Risk and prevention in underserved populations. J. Young Investig. 14(5):1-2. Crossref |
||||
|
Davies GM, Blinkhorn FA, Duxbury JT (2001). Caries among 3-year-olds in greater Manchester. Br. Dent. J. 190:381-384. Crossref |
||||
|
Dini EL, Holt RD, Bedi R (2000). Caries and its association with infant feeding and oral health-related behaviours in 3–4-year-old Brazilian children. Community Dent. Oral Epidemiol. 28:241-248. Crossref |
||||
|
Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG, Selwitz RH (1999). Diagnosing and reporting early childhood caries for research purposes. A report of a workshop sponsored by the National Institute of Dental and Craniofacial Research, the Health Resources and Services Administration, and the Health Care Financing Administration. J. Public Health Dent. 59(3):192-197. Crossref |
||||
|
Du M, Luo Y, Zeng X, Alkhatib N, Bedi R (2007). Caries in preschool children and its risk factors in 2 provinces in China. Quintessence Int. 38:143-151. Pubmed |
||||
|
Hallett KB, O'Rourke PK (2006). Caries experience in preschool children referred for specialist dental care in hospital. Aust. Dent. J. 51:124-129. Crossref |
||||
| Harrison R, White L (1997). A community-based approach to infant and child oral health promotion in a British Columbia First Nations community. Can. J. Community Dent. 12:7–14. | ||||
|
Harrison R, Wong T, Ewan C, Contreras B, Phung Y (1997). Feeding practices and dental caries in an urban Canadian population of Vietnamese preschool children. ASDC J. Dent. Child. 64:112-117. PMid:9189000 |
||||
|
Iida H, Auinger P, Billings RJ, Weitzman M (2007). Association between Infant Breastfeeding and Early Childhood Caries in the United States. Pediatrics 120:e944-e952. Crossref |
||||
|
Ismail AI, Sohn W (1999). A systematic review of clinical diagnostic criteria of early childhood caries. J. Public Health Dent. 59:171-191. Crossref |
||||
|
Jin BH, Ma DS, Moon HS, Paik DI, Hahn SH, Horowitz AM (2003). Early childhood caries: Prevalence and risk factors in Seoul, Korea. J. Public Health Dent. 63:183–188. Crossref |
||||
|
Johansson I, Holgerson PL, Kressin NR, Nunn ME, Tanner AC (2010). Snacking Habits and Caries in Young Children. Caries Res. 44:421-430. Crossref |
||||
|
Jose B, King NM (2003). Early childhood caries lesions in preschool children in Kerala, India. Pediatr. Dent. 25:594-600. Pubmed |
||||
|
Liu Y, Zou J, Shang R, Zhou XD (2007). Genotypic diversity of Streptococcus mutans in 3- to 4-year-old Chinese nursery children suggests horizontal transmission Arch. Oral Biol. 52(9):876-881. Crossref |
||||
| Mahjabeen R, Sudha P, Kulkarni SS, Anegundi R (2006). Dental Caries Prevalence among preschool children in Hubli: Dharwad city. J. Indian Soc. Pedod. Prev. Dent. 2006:19-22. | ||||
|
Marshall T, Gilmore J, Larson M, Warren J, Levy S (2007). Comparison of intakes of sugars by young children with and without dental caries experience. J. Am. Dent. Assoc. 138:39-46. Crossref |
||||
|
Milnes AR (1996). Description and epidemiology of nursing caries. J. Public Health Dent. 56:38-50. Crossref |
||||
|
Nakayama Y, Mori M (2015). Association Between Nocturnal Breastfeeding and Snacking Habits and the Risk of Early Childhood Caries in 18- to 23-Month-Old Japanese Children. J. Epidemiol. 25(2):142-147. Crossref |
||||
|
Nunn ME, Braunstein NS, Krall Kaye EA, Dietrich T, Garcia RI, Henshaw MM (2009). Healthy Eating Index Is a Predictor of Early Childhood Caries. J. Dent. Res. 88(4):361–366. Crossref |
||||
| Pacey A, Nancarrow T, Egeland GM (2007, 2008). Prevalence and risk factors for parental-reported oral health of Inuit preschoolers: Nunavut Inuit Child Health Survey, 2007-2008. Rural Remote Health 10(2):1368. | ||||
|
Rosenblatt A, Zarzar P (2004). Breastfeeding and early childhood caries: an assessment among Brazilian infants. Int. J. Paediatr. Dent. 14:439-445. Crossref |
||||
|
Santos AP, Soviero VM (2002). Caries prevalence and risk factors among children aged 0 to 36 months. Pesqui. Odontol. Bras. 16(3):203-208. Crossref |
||||
|
Segovia-Villanueva A, Estrella-Rodriguez R, Medina-Solis CE, Maupome G (2006). Dental caries experience and factors among preschoolers in southeastern Mexico: a brief communication. J. Public Health Dent. 66:88-91. Crossref |
||||
|
Szatko F, Wierzbicka M, Dybizbanska E, Struzycka I, Iwanicka-Frankowska E (2004). Oral health of Polish three-year-olds and mothers' oral health-related knowledge. Community Dent. Health. 21:175-180. Pubmed |
||||
|
Tsai AI, Chen CY, Li LA, Hsiang CL, Hsu KH (2006). Risk indicators for early childhood caries in Taiwan. Community Dent. Oral Epidemiol. 34:437–445. Crossref |
||||
|
Tyagi R (2008). The prevalence of nursing caries in Davangere preschool children and its relationship with feeding practices and socioeconomic status of the family. J. Indian Soc. Pedod. Prevent Dent. 2008:153-157. Crossref |
||||
|
Van Palenstein Helderman WH, Soe W, van 't Hof MA (2006). Risk factors of early childhood caries in a Southeast Asian population. J. Dent. Res. 85(1):85-88. Crossref |
||||
|
Warren JJ, Weber-Gasparoni K, Marshall TA, Drake DR, Dehkordi-Vakil F, Kolker JL, Dawson DV (2008). Factors associated with dental caries experience in 1-year-old children. J. Public Health Dent. 68(2):70-75. Crossref |
||||
| World Health Organization (WHO) (2003). Global strategy for infant and young child feeding. Geneva: WHO; 2003. Available at: http://www.who.int/nutrition/publications/infantfeeding/9241562218/e/ | ||||
| Wyne A, Khan N (1998). Caries Prevalence In 2 And 3 Year Old Children Of Adelaide, Australia. Odonto-Stomatologie Trop. 8:115-122. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


