ABSTRACT
Proper tooth brushing technique along with tooth brush replacement at recommended intervals may help to protect the accumulation of plaque and reduce the prevalence of dental caries and gingivitis. We aimed to determine the frequency of tooth brush change and the variables associated with this practice in population living in Karachi. A cross sectional study was conducted among dental Orthodontics and Pediatric Dentistry (OPD) visitors of DIKIOHS in Karachi, from, March to May, 2015. A total of 232 participants were selected by using consecutive sampling technique. Data were collected by using a semi structured pretested questionnaire. Socio-demographic and behavioral factors related to tooth brush changing were identified by applying logistic regression model. Majority of participants (65%) were changing tooth brush at every 3 months. After adjusting socio-demographic and dental variables, the odds of changing tooth brush within 3 months among participants who brush more than twice a day, were 3 times more (AOR= 3.49, CI= 1.054 – 11.571) as compared to those who brush once a day. The other factors that showed significant association in multivariate analysis were people who had monthly income >50,000 Pakistan rupees, users of other mouth cleaning aids and people using tooth brush with soft bristles. This study concluded that majority of the participants were changing their tooth brush at recommended intervals and different variables (demographic, socioeconomic and dental) are associated with the frequency of tooth brush changing.
Key words: Tooth brush change, oral hygiene variables, Karachi.
Oral health is now widely accepted as equally important in relation to general health and is reflective of a person’s general health. A number of factors are linked with different oral conditions contributing towards basis of the common risk factor approach (WHO, 2000) in the prevention of oral diseases. Such factors include tobacco smoking, nutritional status, oral hygiene, stress, alcohol etc (Sheiham and Watt, 2000). Among these oral hygiene is an important factor which plays a significant part in the prevention of oral diseases. It is recommended by the American Dental Association to brush and floss at least once a day in order to avoid oral diseases (Bhat et al., 2010).
Available literature on tooth brushing majorly focused on plaque removal efficiency of either manual or electric toothbrushes, or with some kind of modification (Taschner et al., 2012; Rosema et al., 2013). Other studies have described it as independent variable in various oral diseases (Molina-Frechero et al., 2012; Pita-Fernández et al., 2010). In terms of prevalence of tooth brushing behavior, study in China reports 44.4% (Zhu et al., 2003), and 31% in Jordan (Rajab et al., 2002). Other countries report higher prevalence, with figures between 51.6 and 99.4% (Herrera et al., 2009; Wierzbicka et al., 2002; Al-Omiri et al., 2006; Petersen et al., 2001; Kolawole et al., 2011). Data published for industrialized countries, including European countries, USA, and Canada; vary between 16 to 80% in boys and 26 to 89% in girls (Pita-Fernández et al., 2010; Maes et al., 2006), to 47% in socially disadvantaged groups in New Zealand ( Schluter et al., 2007).
In Mexican study on tooth brushing and associated socio-demographic indicators, the results suggest that different variables (socio-demographic, socioeconomic, and dental) may influence the frequency of tooth brushing. Furthermore, family size (a proxy for socioeconomic status) may indicate certain oral health inequities in this population, which can influence oral self-care behaviors in populations of Mexican origin (Casanova – Rosado et al., 2014).
In Pakistan, research data regarding oral hygiene habits specifically about practice of tooth brush replacement, at national level is scarce, though different studies have been carried out in different hospitals. Recent study from Peshawar regarding the use of tooth-brush for oral hygiene depicts majority of the participants were brushing their teeth regularly once a day and males were more particular about their oral health compared with females. Moreover, improved brushing habits were observed with better economic status (Shah et al., 2015).
Although toothbrush has a major impact on adequacy of oral hygiene, there are many other contributing factors. These factors have not been well demonstrated from an epidemiological perspective. There are many reasons that indicate need to investigate the socio-demographic and socioeconomic factors which could modify the adequacy of oral hygiene. Most importantly, it could provide the opportunity to identify target populations to plan preventive dental programs at the individual and community levels. Previous studies identified various variables which were either improved or worsen the oral hygiene (Martens et al., 2004; Mubeen and Nisar, 2015). Among these variables are gender, age, and frequency of tooth brushing, type of brushing and cleaning aids, daily consumption of sugared beverages, and the amount of toothpaste used. As expected, there is a great deal of variation in these patterns.
Along with tooth brushing, the knowledge of type of toothbrush and the frequency of changing tooth brush is also very important for the prevention of dental caries as well as periodontal problems. Related to these crucial oral hygiene variables and associated behavioral factors, there is scarcity of epidemiological studies in Pakistan.
Keeping in view the importance of social background and oral hygiene practices of individuals, the present study was carried out to determine the impact of the socio-demographic and hygiene factors on tooth brush replacement frequency among patients visiting dental Orthodontics and Pediatric Dentistry (OPD) at DIKIOHS, Karachi.
Study area, design and period
A cross sectional study was conducted among patients visiting out-patient department of Dr. Ishrat ul Ibaad Khan institute of oral sciences in Karachi, Pakistan from March to May’ 2015.
Sample size and sampling technique
A sample size of 232 was calculated through the proportion of mother’s knowledge regarding correct brushing technique (18.1%) with 95% confidence interval and a 5% margin of error (Mubeen and Nisar, 2015). The sample was recruited by convenient sampling technique. Incoming patients in all departments were included following inclusion criteria.
Instrument and data collection
Study participants aged above 18 years and gave written consent, were included in study and were interviewed using a structured and pre-validated questionnaire. Data were collected after taking written consent from the participants and they were informed about the purpose and benefits of the study.
The questionnaire collected data provide basic demographic data (age, gender, marital status, household income, etc.) questions about and dental services utilization patterns and oral hygiene self-practices, including change of tooth brush (dependent variable), frequency of brushing, brush type, toothpaste type, the tools used for cleaning the mouth, duration of tooth brushing, use of extra tools such as dental floss and mouthwash, and their concern about oral hygiene of family and peers. Average time allotted to fill the questionnaire was 10 to 15 min. Changes were made to the questionnaire before data collection in the light of responses collected during validation phase.
Ethical consideration
The ethical approval was obtained from institutional review board, Dow University of health sciences, Karachi. Verbal and written consent was obtained from the participants prior to data collection.
Data management and analysis
Data entry and analysis was performed via SPSS V.16 software (SPSS. Inc., Chicago, IL, USA). Baseline characteristics of the study subjects were calculated as frequencies and percentages for categorical variables, and as means ± standard deviations for numeric variables. A multivariate binary logistic regression model employed to estimate the strength of association between tooth brush changing frequency (dependent variable) and the independent variables, which is expressed as odds ratios with 95% confidence intervals (95% CI), as well as reporting the p values that were considered statistically significant (p-value <0.05) for multivariate analysis, the independent variables having p-value ≤0.25 were included. To control for confounding, the final model included those variables that had a p-value <0.25 in the bi-variate analysis.
A total of 232 participants visiting dental OPD gave consent and returned the completed questionnaire and hence, considered to include in data analysis. The overall response rate was 85%. Incompletely filled questionnaires were taken as non respondents.
Descriptive statistics
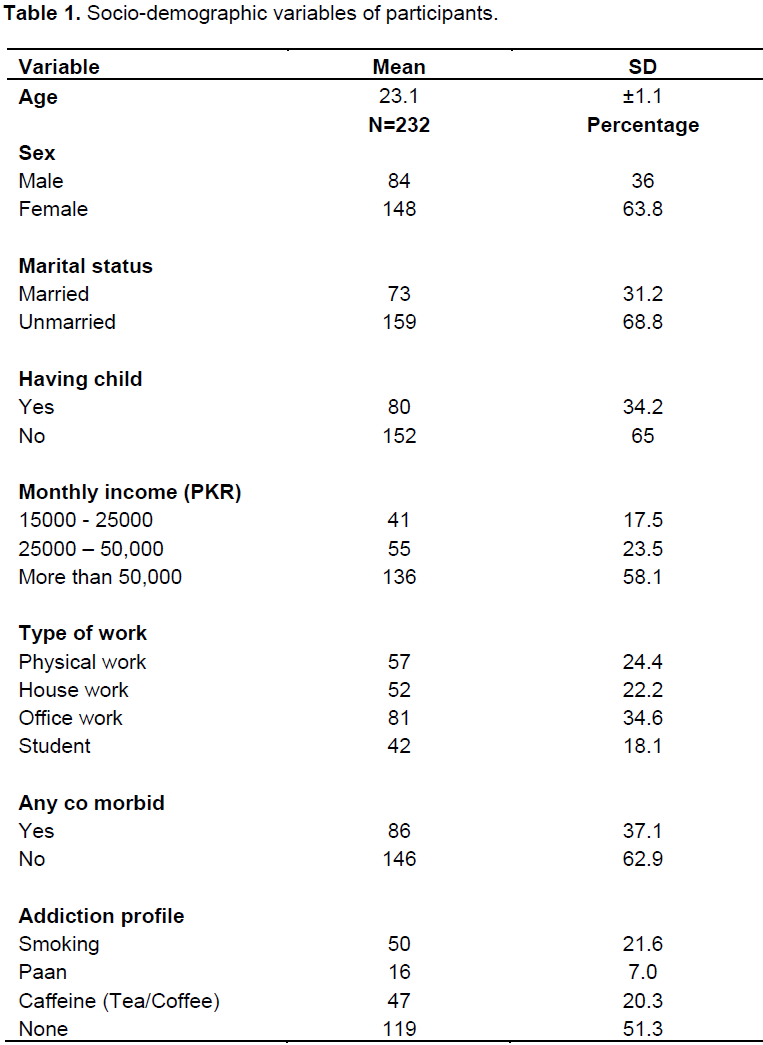
The mean age of participants was 23.1 (SD±1.1) and females are in higher proportion (63.8%) than males (36%). Most of participants were unmarried (68.8%) and belong to higher income group (58.1%). Majority reported no addiction (51%). Smoking and users of tea/coffee were almost in same numbers (21.6 and 20.3% respectively. Table 1 describes socio-demographic characteristics of study participants.
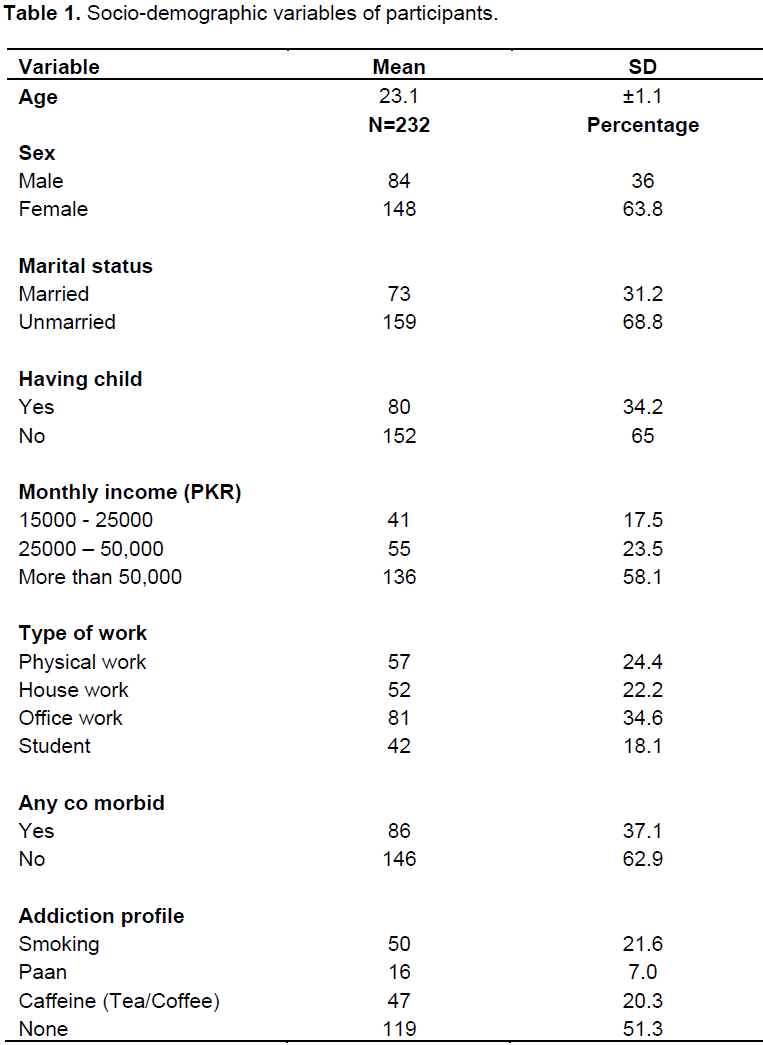
Participants reported their oral health and hygiene practices. About 72.8% of them had visited dentist for more than 6 months interval while 81% had some kind of dental treatment. Most of them were using tooth brush (90%) as cleaning aid and were using combined technique of tooth brushing (58.4%) followed by horizontal brushing technique users (24.1%). Regarding type of tooth paste and tooth brush use, frequency of sensitivity relief paste users were higher (38.4%) than whitening and cavity protection pastes while tooth brush having medium-textured bristles was used more frequently (47.4%) by participants. More than twice a day tooth brushing was observed by very small group of patients (11.2%) followed by once a day while majority brushed twice (51.3%). Regarding duration of tooth brushing, majority participants brush their teeth for 2 min (62.5%) and most of them changed their tooth brush at every 3 months interval (65.5%). Flossing and cleaning of tongue/palate were also in practice of majority participants.
Bi-variate analysis
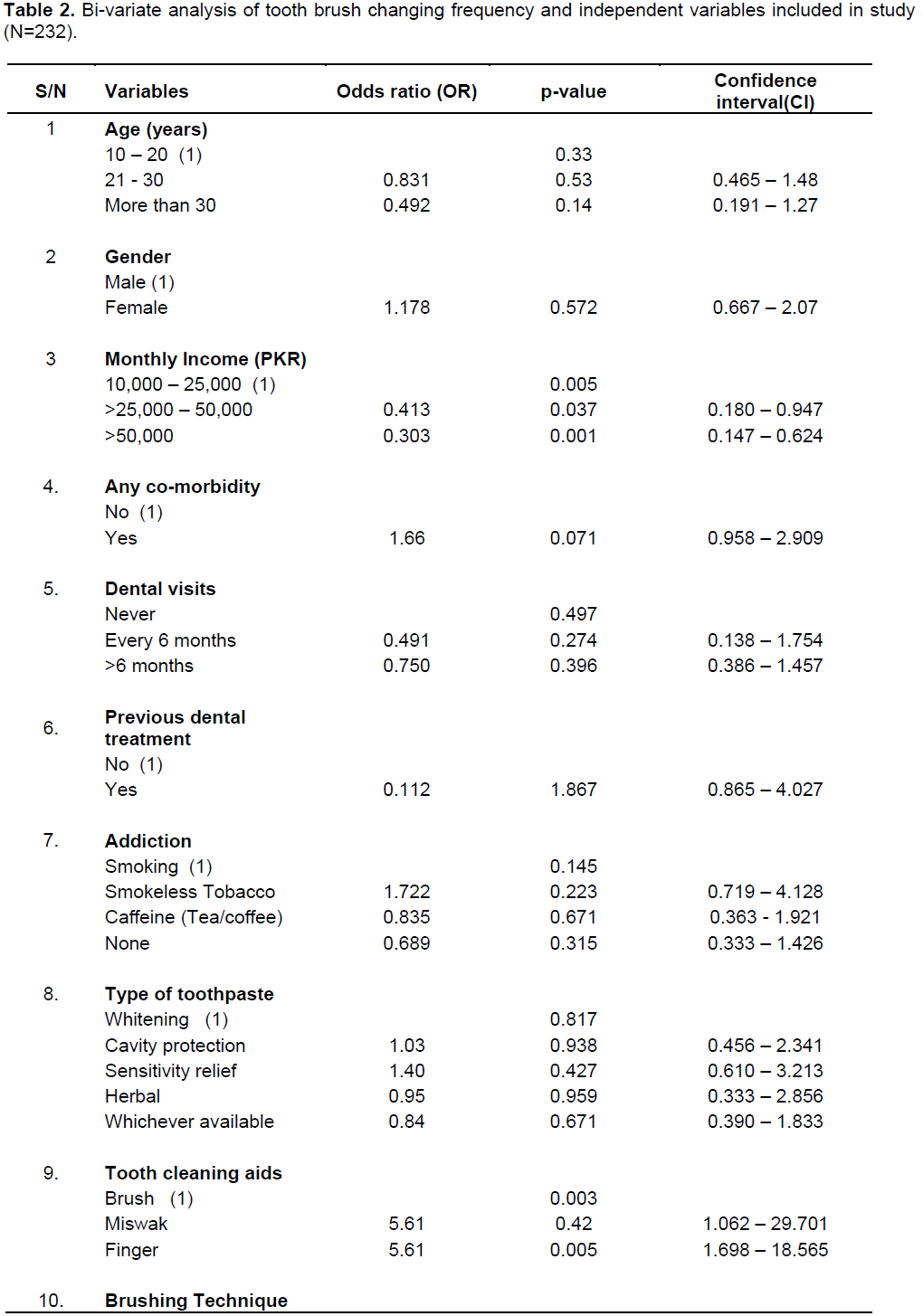
Table 2 shows results of the bi-variate analysis. The bi-variate analysis depicted that the odds of changing tooth brush among higher monthly income group (>50,000 PKR) were about one-third (OR= 0.30, CI= 0.147 – 0.624, p-value 0.001) as compared to lowest income group. The odds of changing tooth brush within 3 months among users of miswak and finger as tooth cleaning tools, were 5 times higher (OR= 5.6, CI= 1.062 – 29.701, p-value 0.42 and OR= 5.6, CI= 1.698 – 18.565, p-value 0.005 respectively) as compared to those using tooth brush only.
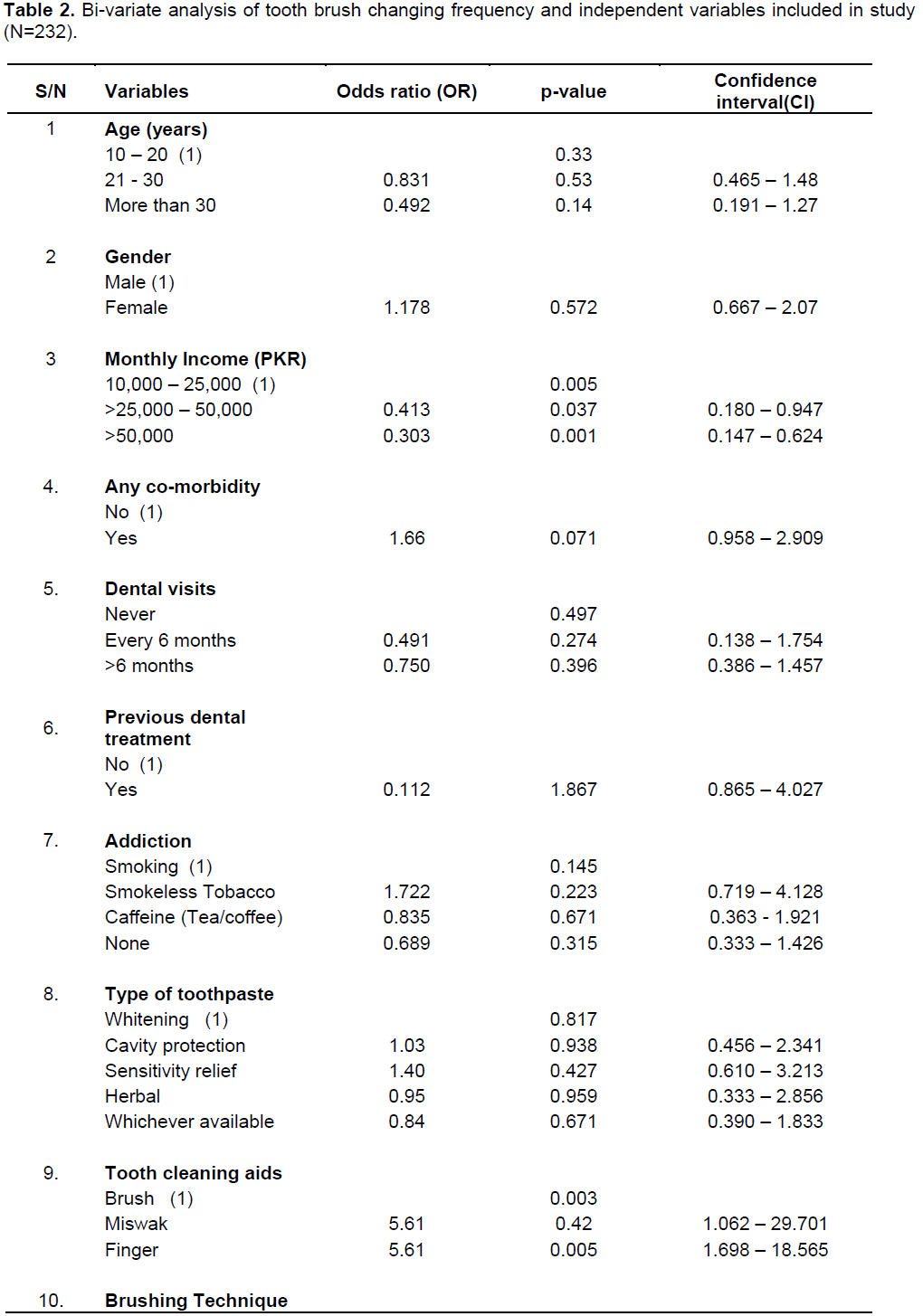
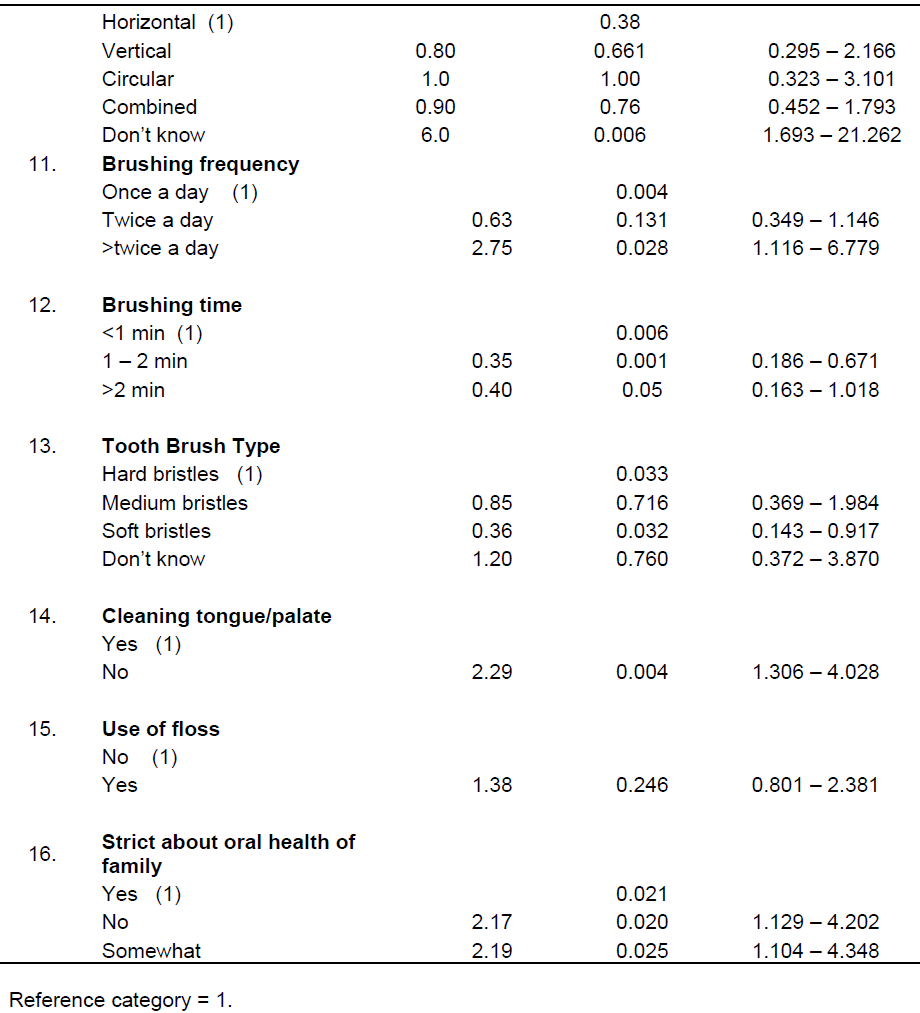
The odds of changing tooth brush within 3 months among those who were unknown about brushing technique were 6 times more (OR= 6.0, CI= 1.693 – 21.262, p-value 0.006) as compared to horizontal brushing method users. The odds of changing tooth brush within 3 months among those who brush more than twice a day were 2 times higher (OR= 2.5, CI= 1.116- 6.779, p-value 0.02) as compared to those who brush once a day. The odds of changing tooth brush within 3 months among soft bristles brush users were one-third (OR= 0.36, CI= 0.143- 0.917, p-value 0.03) as compared to hard bristles brush users. The odds of changing tooth brush within 3 months among participants who did not clean their tongue/palate with tooth brush, were 2 times higher (OR= 2.29, CI= 1.306- 4.028, p-value 0.004) as compared to those who clean their tongue/palate.
Multi-variate analysis
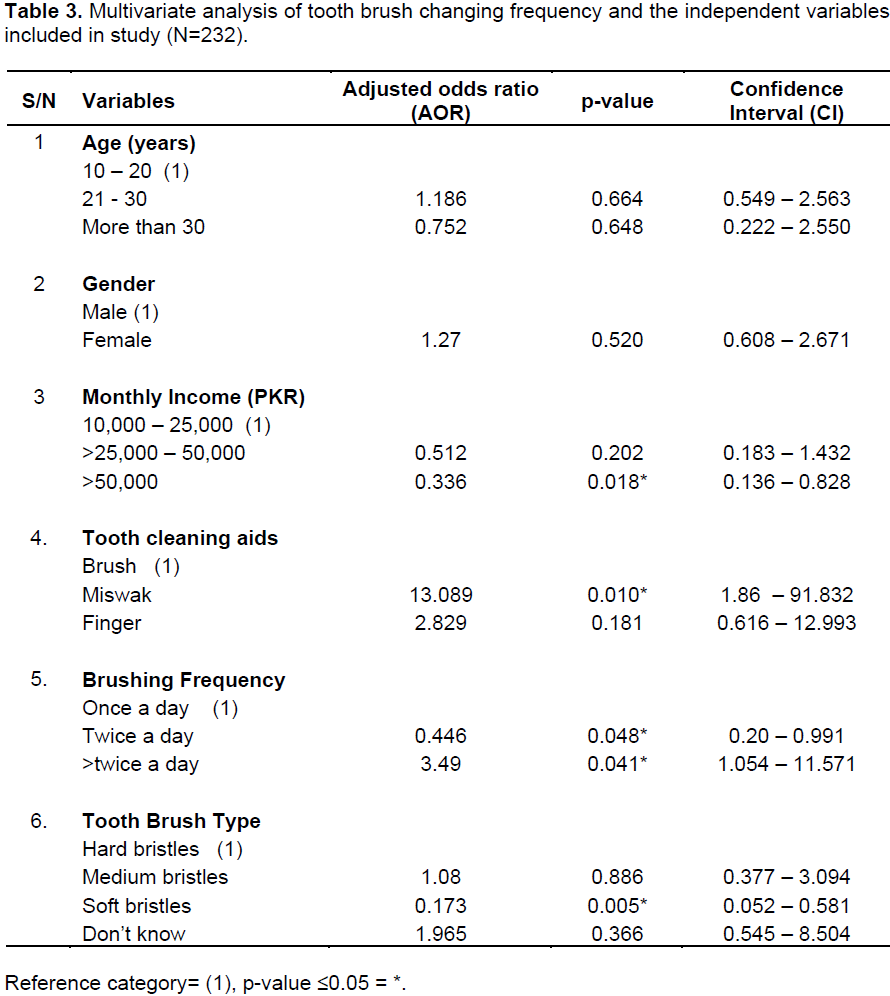
The logistic regression model is shown in Table 3. After adjusting for socio-demographics and oral-hygiene related variables, the odds of changing tooth brush within 3 months among participants who had monthly income >50,000 PKR were one-third (AOR= 0.336, CI= 0.136- 0.828) as compared to lowest monthly income group. The odds of changing tooth brush within 3 months among miswak users were 13 times higher (AOR= 13.08, CI= 1.86 - 91.83). The odds of changing tooth brush within 3 months among participants who brush more than twice a day, were 3 times more (AOR= 3.49, CI= 1.054-11.571) as compared to those who brush once a day. Finally, frequency of changing of tooth brush within 3 months among soft bristles brush users, were decreased (AOR= 0.17, CI= 0.052-0.581).
This cross-sectional was carried out among visitors at dental OPD of Dr. Ishrat ul Ibaad Khan institute of oral health sciences. This study characterized the frequency of changing tooth brush in a sample of general public of Karachi, together with socio-demographic and oral hygiene practices associated with it. The sampling technique used in this study was convenient sample which had its limitations.
There are certain methodological limitations in this study strategy that must be considered to place the value of the findings in an objective perspective. It is necessary to note that all self-reported data are susceptible to a socially desirable behavior bias, in which the subjects report what they believe to be socially acceptable. Another limitation is inherent to cross-sectional studies’ designs, which measure the cause and effect at the same time, thus the relationships described are not necessarily causal. Despite being unique in objective and first in reporting these findings locally, the study has limitation of small sample size and not truly representative of population of Karachi.
The literature lacks studies about frequency of changing tooth brush and the effect of demographic as well as oral hygiene variables on it among residents of Karachi. This study is of prime importance in this field as it is the first to explore this area among general public of Karachi. The overall frequency of changing brush within 3 months was 65.5% in our study sample. In our study, 62% females reported higher frequency of brush change within 3 months than males. This finding is similar to a study where females (53.4%) more frequently changing their toothbrush every 3 months in comparison to males (Oberoi et al., 2014). Other demographic variables which presented with higher number of participants changing tooth brush every 3 months are 21 to 30 years age group and higher monthly income group. Socio-economic status has impact on tooth brush replacement practice and people belong to higher income class in our study, tend to replace their tooth brush more often. Some author mentioned this link is due to people from the high socio-economic class brush their teeth more frequently (Herrera et al., 2009; Vallejos-Sánchez et al., 2006).
A study conducted at Mexico showed that people of lower socioeconomic status have fewer resources to meet oral health challenges: less free time, less money to buy toothpaste and toothbrushes (Casanova – Rosado et al., 2014). Similarly, our study participants from lower and middle class as per monthly income were found to be in practice of not changing tooth brush for every 3 months. This could be due to lack of oral health knowledge and more economic burden on lower class families in our society.
Daily brushing frequency has profound effect on practice of tooth brush changing in our study. About 66% of participants, who change their tooth brush every 3 months, had reported brushing frequency of twice a day and more. This effect is probably due to increased frequency contact of tooth brush with tooth surface and also depends on manual dexterity of brush user as greater brushing force cause bristles to worn out more rapidly. A local survey in Peshawer showed that the majority had frequency of brushing once a day and majority of their participants change tooth brush for every 2 to 6 months interval (Ataullah et al., 2010).
The majority of the patients in the present study used toothpaste and toothbrush (90%) as tooth cleaning aid whereas Finger and Miswak was used by (0.6 and 0.3%) of the participants which was similar to the study conducted by Ali et al. ( 2012) in which, (88.0%) patients had preferred practices of using tooth paste followed by tooth powder (5.76%) and Miswak (2.64%), respectively, and study of Hind Al-Johani (2008) where almost all the patients (95.4%) used tooth brush for cleaning their teeth. Further, in our study about 9.6% of participants, who change their tooth brush within 3 months, were using tooth brush as mouth cleaning aid. As per model, tooth cleaning aids reported in our study have effect on tooth brush changing frequency, specifically Miswak. No supporting evidence related to this effect of Miswak is present, but it could be due to the greater manual effort for using Miswak for cleaning teeth which unintentionally come in tooth brushing practice of participants and therefore, more chance of toothbrush worn lead to early replacement of tooth brush.
Our study shows that those who change their tooth brush within 3 months were using tooth brushes with medium and soft bristles (44 and 38% respectively). Bending and splaying of bristles was selected as the main indicator that a toothbrush needs to be renewed. This is well appreciated in our study as tooth brushes with more bristle wear were replaced more frequently as compared to hard bristle tooth brushes. A clinical trial on plaque removing efficacy of new and worn old tooth brushes, revealed that there was a statistically significant relationship between the toothbrushes and plaque values that were increasing in group of students that did not change toothbrushes, therefore it is recommended to replace the tooth-brush as soon as bristle splaying and matting is observed because it loses its cleaning ability. Trial concluded that toothbrushes can lose their ability to properly remove plaque after a period of three months (AL-Naimi, 2009).
This study concluded that about two-third of participants change their tooth brush every 3 months, which is a recommended oral hygiene practice. The results suggest that different socio-demographic and dental variables specifically monthly income, tooth brushing frequency, tooth brush type and use of other mouth cleaning aids, may influence the frequency of tooth brush changing. Further, oral health inequities in our population can influence oral self-care behaviors and to observe these trends have an impact on behavioral patterns in other populations it is something that must be determined by future studies addressing patterns of socio-cultural behaviors.
The authors have not declared any conflict of interests.
The authors’ are thankful to the entire participant who contributed in the study.
REFERENCES
|
Ali NS, Khan M, Butt M, Riaz S (2012). Implications of practices and perception on oral hygiene in patients attending a tertiary care hospital. J. Pak. Dent Assoc. 1:20-30.
|
|
|
|
AL-Naimi RJ. 2009. Evaluation of Toothbrush Wear on Tooth brushing Efficiency. Al–Rafidain Dent J. 9(1):51-56.
|
|
|
|
|
Al-Omiri MK, Al-Wahadni AM, Saeed KN (2006). Oral health attitudes, knowledge, and behavior among school children in North Jordan. J. Dent Educ. 70:179-87.
|
|
|
|
|
Ataullah KM, Khan AA (2010). Oral health related knowledge, attitude and practices among patients – a study. Pak. Oral Dental J. 30(1).
|
|
|
|
|
Bhat PK, Kumar A, Aruna CN (2010). Preventive oral health knowledge, practice and behaviour of patients attending dental institution in Bangalore, India. J. Int. Oral Health 3:28-38.
|
|
|
|
|
Casanova-Rosado AJ, Medina-Solís CE, Casanova-Rosado JF, Vallejos-Sánchez AA, Minaya-Sánchez M, Mendoza-Rodríguez M, Maupomé G (2014). Tooth brushing frequency in Mexican schoolchildren and associated socio-demographic, socioeconomic, and dental variables. Medical science monitor: Int. Med. J. Exp. Clin. Res. 20:938-944.
|
|
|
|
|
Herrera MS, Lucas-Rincón SE, Medina-Solís CE et al. (2009). Socioeconomic inequalities in oral health: factors associated with tooth brushing frequency among Nicaraguan schoolchildren. Rev. Invest Clin. 61:489-960.
View
|
|
|
|
|
Johani HA (2008). Oral Hygiene Practice among Saudi Patients in Jeddah. Cairo Dent J. 24:395-401
|
|
|
|
|
Kolawole KA, Oziegbe EO, Bamise CT (2011). Oral hygiene measures and the periodontal status of school children. Int. J. Dent Hyg. 9:143-48
Crossref
|
|
|
|
|
Maes L, Vereecken C, Vanobbergen J, Honkala S (2006). Tooth brushing and social characteristics of families in 32 countries. Int. Dent J. 56:159-167
Crossref
|
|
|
|
|
Martens L, Vanobbergen J, Leroy R, Lesaffre E, Declerck D (2004). Variables associated with oral hygiene levels in 7-year-olds in Belgium. Community Dent Health 21:4-10.
|
|
|
|
|
Molina-Frechero N, Pierdant-Rodríguez AI, Oropeza-Oropeza A, Bologna-Molina R (2012). Fluorosis and dental caries: an assessment of risk factors in Mexican children. Rev. Invest Clin. 64:67-73.
|
|
|
|
|
Mubeen N, Nisar N (2015). Factors' affecting mother's brushing technique of less than five years age children in Pakistan. J. Dent. Oral Hyg. 7(6):86-90.
|
|
|
|
|
Oberoi SS, Mohanty V, Mahajan A, Oberoi A (2014). Evaluating awareness regarding oral hygiene practices and exploring gender differences among patients attending for oral prophylaxis. J. Indian Soc. Periodontol. 18(3):369-374.
Crossref
|
|
|
|
|
Petersen PE, Hoerup N, Poomviset N, Prommajan J, Watanapa A (2001). Oral health status and oral health behaviour of urban and rural schoolchildren in Southern Thailand. Int. Dent. J. 51:95-102.
Crossref
|
|
|
|
|
Pita-Fernández S, Pombo-Sánchez A, Suárez-Quintanilla J, Novio-Mallón S, Rivas-Mundina B, Pértega-Díaz S (2010). Clinical relevance of tooth brushing in relation to dental caries. Aten Primaria. 42:372-379.
Crossref
|
|
|
|
|
Rajab LD, Petersen PE, Bakaeen G, Hamdan MA (2002). Oral health behaviour of schoolchildren and parents in Jordan. Int. J. Paediatr. Dent. 12:168-76
Crossref
|
|
|
|
|
Rosema N, Hennequin-Hoenderdos N, Versteeg P, Palenstein Helderman WH, Velden U, Weijden GA (2013). Plaque-removing efficacy of new and used manual toothbrushes – a professional brushing study. Int. J. Dent Hyg. 11(4):237-243.
Crossref
|
|
|
|
|
Schluter PJ, Durward C, Cartwright S, Paterson J (2007). Maternal self-report of oral health in 4-year-old Pacific children from South Auckland, New Zealand: findings from the Pacific Islands Families Study. J. Public Health Dent. 67:69-70.
Crossref
|
|
|
|
|
Shah MN, Akhtar S, Khan MA., Shah F (2015). Tooth brushing habits and knowledge among patients visiting Khyber College of dentistry. JKCD 5:54-56.
|
|
|
|
|
Sheiham A, Watt RG (2000). The Common Risk Factor Approach: A rational basis for promoting oral health. Commun. Dent Oral Epidemiol. 28(6):399-406.
Crossref
|
|
|
|
|
Taschner M, Rumi K, Master AS, Wei J, Strate J, Pelka M (2012). Comparing efficacy of plaque removal using professionally applied manual and power toothbrushes in 4- to 7-year-old children. Pediatr. Dent. 34:61-65.
|
|
|
|
|
Vallejos-Sánchez AA, Medina-Solís CE, Casanova-Rosado JF (2006). Factors associated with the practice of tooth brushing among school. Rev. Mex. Pediatr. 73(4):167-171.
|
|
|
|
|
Wierzbicka M, Petersen PE, Szatko F, Dybizbanska E, Kalo I (2002). Changing oral health status and oral health behaviour of schoolchildren in Poland. Community Dent. Health 19:243-250.
|
|
|
|
|
Zhu L, Petersen PE, Wang HY, Bian JY, Zhang BX (2003). Oral health knowledge, attitudes and behaviour of children and adolescents in China. Int. Dent. J. 53:289-298.
Crossref
|
|
|
|